Expert Review
Gastroenterology: Expert Review and Commentary from Published Literature
Bile Acid Sequestrants: Putting a Unique Mechanism to Work
Pierre Paré, MD, FRCPC, FACG
CHAUQ-Hôpital du SaintSacrement, Québec, QC
Bile acid sequestrants were initially developed for the treatment of hypercholesterolemia, but it is significant that essentially all the activity of these agents is confined to the gastrointestinal (GI) tract. The binding of bile acid in the intestine inhibits a key mechanism of cholesterol transport, but the GI applications of these agents are also considerable. Over the last decade, as statins have become the dominant treatment for elevated low density lipoprotein (LDL) cholesterol, GI applications have grown in relative importance. Although drugs in this class have been available for 50 years, the broad clinical applications deserve to be revisited. There has been a recent resurgence in the use of bile acid sequestrants for cardiovascular protection due to the intolerability of the very high doses of statins, but these agents are also relevant for use with several GI disorders.
History and Mechanism of Bile Acid Sequestrants
Bile acid activity, which is mediated by the liver, has relevance to a variety of physiologic and pathologic processes. A by-product of cholesterol synthesis in the liver, bile acids are cytotoxic but are normally rendered impermeable to cell membranes due to conjugation with amino acids. Bile acids have an important role in cholesterol homeostasis by moving cholesterol from the hepatocyte to the intestine for fecal excretion through a solubilization process, by transporting dietary lipids from the intestine back to the liver, and by serving as a negative feedback signal to the liver to increase cholesterol production.
In pathologic processes driven by bile acids, sequestrants are effective for controlling disease expression.
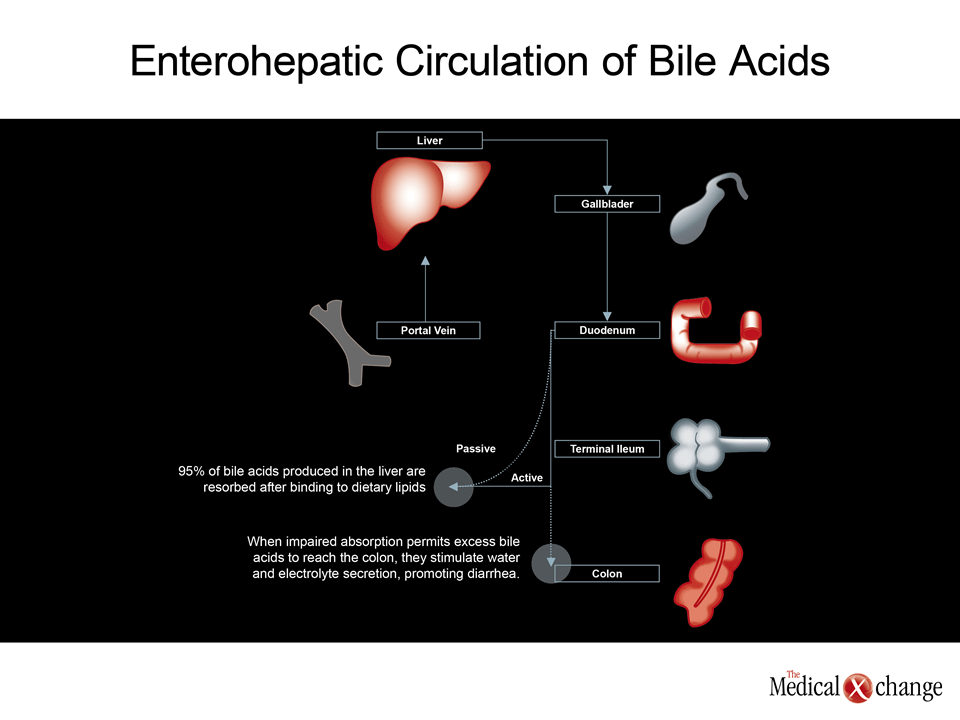
However, the activity of bile acids is not confined to cholesterol regulation. Bile acids also promote dietary absorption of several essential elements such as iron and calcium,(1) play a role in regulation of motility,(2) influence the intestinal absorption of water and electrolytes,(3)help regulate glucose metabolism,(4) and exert bacteriostatic effects both through regulation of motility and by inhibiting bacterial adhesion to the intestinal mucosa.(5) In patients with insufficient bile acids, such as those with short bowel syndrome, replacement may be necessary to normalize lipid and fat absorption. In pathologic processes driven by bile acids, sequestrants are effective for controlling disease expression. (Fig. 1) Bile acid sequestrants were pursued in the 1950s as a means of lowering lipids in humans based on a series of observations in animals. The currently available bile acid sequestrants include colesevelam, colestipol, and cholestyramine. Although the chemical compositions of these agents differ, all bind to the major bile acids to form an insoluble complex that prevents reabsorption and leads to fecal excretion. Moreover, the depletion of bile acid stores promotes increased bile acid synthesis which reduces the pool of intracellular cholesterol, thereby helping to maintain a lower cholesterol level. Appreciation for the effects of bile acid sequestrants has led to the use of these agents for several other clinical applications, particularly diarrhea of various etiologies.
Earliest Indication: Cardiovascular Disease Prevention
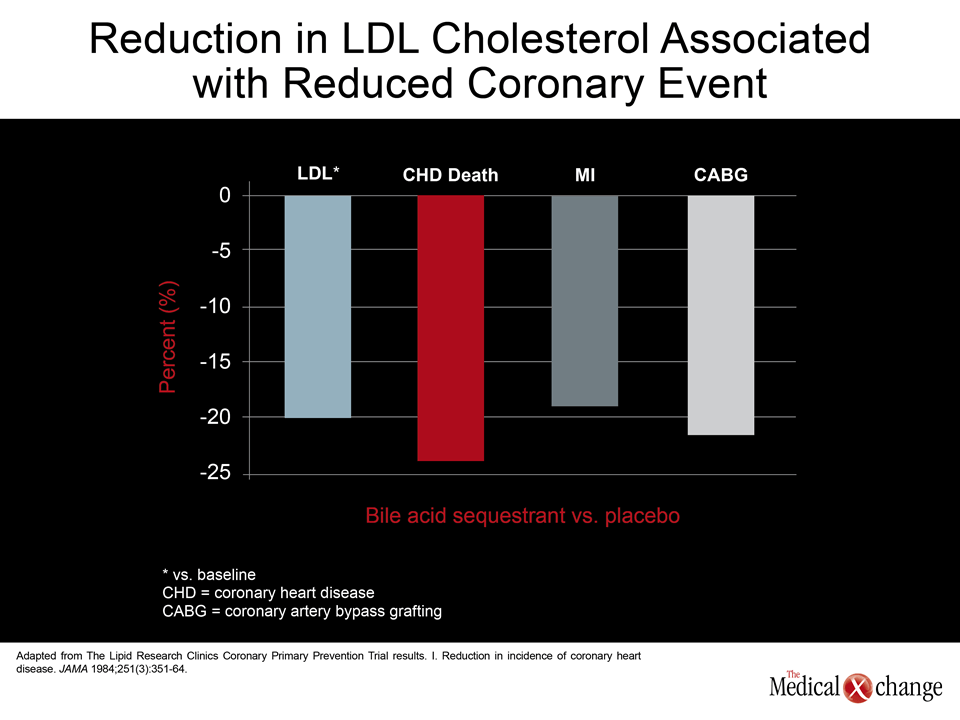
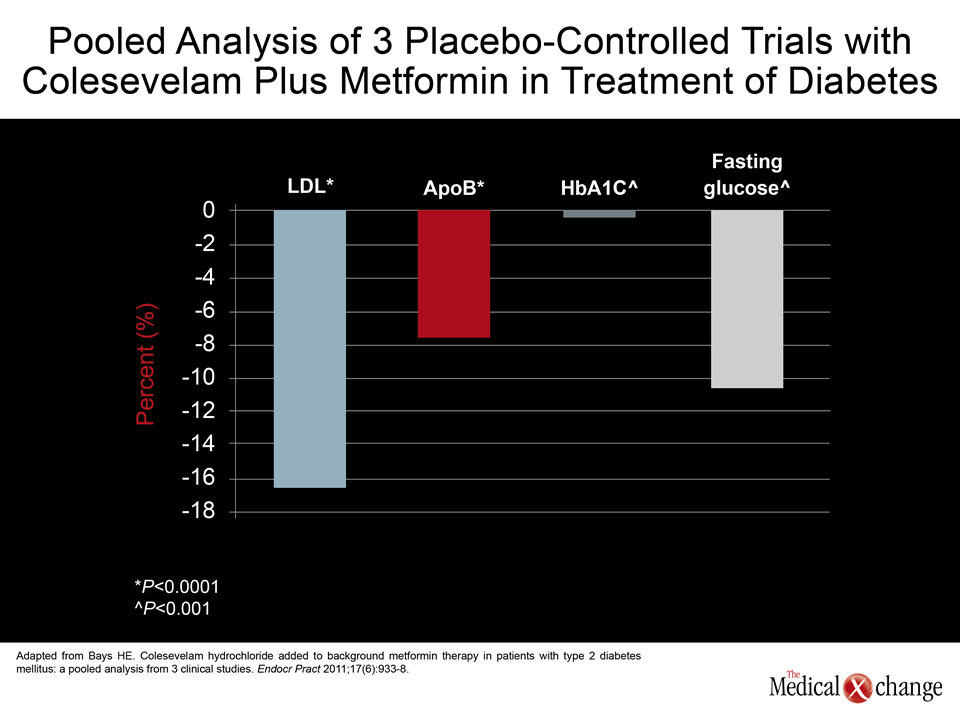
Bile acid sequestrants reduce cholesterol levels by 15% to 30%, almost all of which is in the form of LDL cholesterol.(6)A series of trials have validated that this degree of cholesterol lowering is effective for the treatment of cardiovascular disease (CVD). In the placebo-controlled Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT), for example, the 12% reduction in LDL was associated with a 19% reduction in coronary events (Fig. 2).(7) An angiographic-controlled trial was able to show that the reductions in LDL reduced progression of atherosclerosis.(8) Bile acid sequestrants have been recommended for primary control of CVD by the National Cholesterol Education Panel (NCEP) since 1984. Due to the fact that bile acid sequestrants exert their pharmacologic effect almost exclusively in the GI tract with very little systemic absorption, these agents are generally well tolerated. The most common adverse events associated with these agents have been GI related, including constipation, but these develop in a minority of patients at commonly-used doses. Approved for use in children, the safety of these agents was a primary reason that they became a first-line agent for treatment of hypercholesterolemia. With the introduction of statins, bile acid sequestrants were largely replaced as first-line agents but continued to be used adjunctively for those who were not able to reach treatment targets or as a replacement for those who were statin intolerant. Their LDL-lowering effects can be synergistic with other lipid-lowering agents. A rising rate of statin intolerance has refocused interest in alternative lipid-lowering agents, including bile acid sequestrants. Although such side effects as myalgia, myositis, and rhabdomyolysis have been associated with statins from the earliest clinical trials, these events, like liver enzyme abnormalities, are being encountered with more frequency because much higher doses are being prescribed than those initially. High dose statin therapy is a consequence of more rigorous LDL targets in large segments of the population at risk for CVD. Once considered uncommon, statin intolerance has been recently reported in up to 20% of patients taking these agents.(9) For statin intolerance or for patients who cannot reach LDL targets on statin therapy alone, bile acid sequestrants remain among the best options for lipid control. The first class of agents to demonstrate protection against CVD through lipid lowering, bile acid sequestrants have a well-established record of efficacy and safety. Although traditionally administered as a powder mixed with food or liquid, newer tablet formulations have increased convenience and reduced issues of taste, facilitating use in the chronic regimens required for CV risk reduction. Bile acid sequestrants may be of particular value in the treatment of hypercholesterolemia in diabetics, because these agents have also been associated with a modest but clinically significant improvement in glycemic control. In a double-blind study with colesevelam in type 2 diabetes patients poorly controlled on their current regimen, the addition of the bile acid sequestrant lowered the HbA1c significantly, although the exact mechanism remains unclear.(10)However, another double-blind study testing colesevelam in combination with metformin also documented clinically significant reductions in serum lipids and blood glucose levels, yielding the conclusion that this is an attractive initial combination in patients with both metabolic abnormalities.(11)In a pooled analysis of three placebo-controlled trials, colesevelam was associated with a 16.5% reduction in LDL (P<0.001), a 7.4% reduction in ApoB (P<0.001), a 0.5% reduction in HbA1c (P<0.001), and a 10% reduction in fasting glucose (P<0.001).(12) (Fig. 3)
GI Disease: A Useful Drug Effect
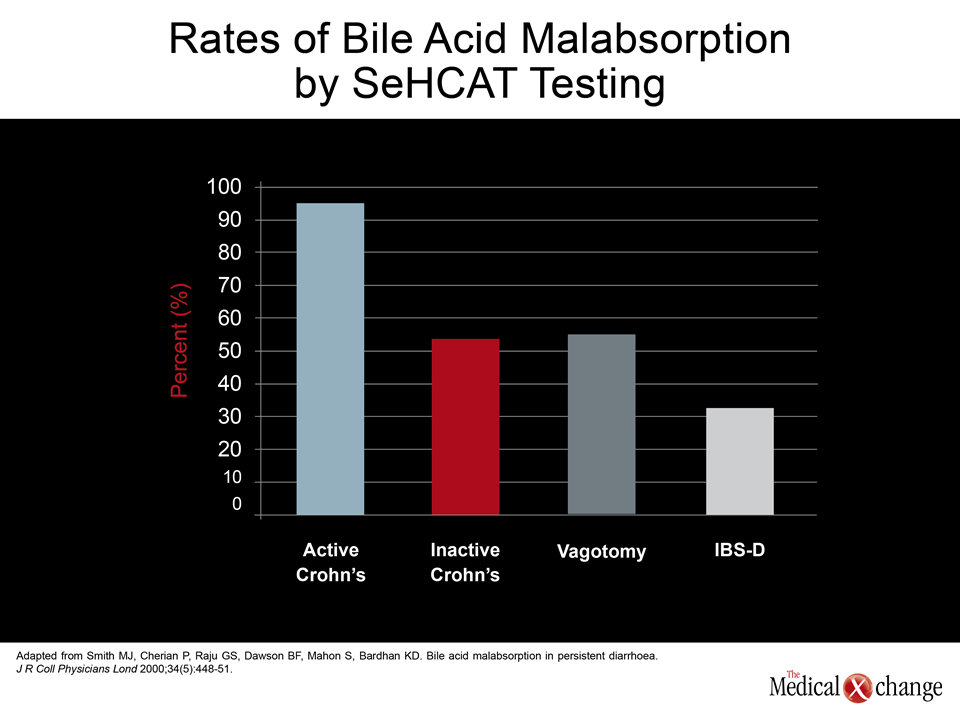
The most important role of bile acid sequestrants in the control of GI-related disorders has stemmed from its value in the control of diarrhea related to bile acid malabsorption. This condition has numerous etiologies, including Crohn’s disease, cholecystectomy, ileal resection, vagotomy, and celiac disease. In normal physiologic function, bile acids flow into the duodenum after a meal-stimulated gallbladder contraction then pass into the intestine where, among other activities, they bind to dietary lipids for transport back to the liver. Normally, 95% of the bile acids are reabsorbed and the remainder is excreted by the fecal route.(13) When bile acid absorption is disturbed, the increased proportion of bile salts that reach the colon are deconjugated by resident bacteria and then appear to interact with enterocytes and other cells in the brush-border membrane. The complex mechanisms by which bile salts stimulate water and electrolyte secretion, producing watery diarrhea and, in some cases, steatorrhea, include stimulation of anion secretion, upregulation of cyclic AMP (cAMP) activity, increasing cytosolic calcium levels, increasing prostaglandin synthesis in lamina propria cells, stimulating enteric neurons to produce propulsive motor contractions, and increasing tight junction permeability to fluid and electrolytes.(14) When administered orally and transported into the small intestine, the bile acid sequestrants colesevelam, colestipol, and cholestyramine bind to bile acids to form an insoluble complex that can pass through the large intestine with reduced or minimal stimulation of water and electrolyte secretion. While the beneficial effect on diarrhea from bile acid sequestrants in individuals with bile acid malabsorption is a logical expectation, there are clinical studies that confirm the ability of increased bile acid to produce secretory diarrhea as well as studies to demonstrate that bile acid sequestrants counter this effect. In one set of randomized trials published together, administration of the bile acid chenodeoxycholate (CDC) to healthy volunteers significantly increased stool frequency, reduced stool consistency, and accelerated colonic transit.(15) In an accompanying study, the administration of colesevelam to patients with irritable bowel syndrome (IBS) and bile acid malabsorption was associated with a reduction in stool frequency, firmer stool consistency, and a slower transit time relative to placebo. Approximately 30% of patients with Crohn’s disease develop bile acid malabsorption.(16) After cholecystectomy, increased stool frequency and loose stools at least partially due to bile acid malabsorption are also commonly reported.(17) Diarrhea subsequent to ileal resection is also common and attributed to a change in bile acid absorption.(18) A double-blind study has confirmed an improvement in diarrhea secondary to ileal resection with bile acid sequestrants.(19) Although vagotomy and celiac diseases are relatively rare causes of bile acid malabsorption, idiopathic bile acid absorption does occur.(20) Recently, it has been demonstrated that at least some of these cases are due to a defect in fibroblast growth factor-19 (FGF-19), which is produced in the ileal enterocytes, and is a negative feedback for bile acid synthesis.(21) However, bile acid malabsorption regardless of etiology is easily diagnosed by selenium homocholic acid taurine (SeHCAT) testing. Bile acid sequestrants have been used empirically, if more sparingly, for other forms of diarrhea, including the treatment of Clostridium difficile for which the mechanism appears to be their ability to absorb toxins released by the bacteria.(22) However, the anecdotal reports of efficacy from treating idiopathic chronic diarrhea with bile acid sequestrants may at least partially if not mostly stem from control of undiagnosed bile acid malabsorption. In a study of 304 patients with diarrhea who were stratified by their accompanying diagnosis, the rates of bile acid malabsorption as detected with SeHCAT was 97% in those with active Crohn’s disease, 54% in those with Crohn’s disease in remission, 55% in those with vagotomy and pyloroplasty with or without cholecystectomy, and 33% in those with IBS. The authors noted that bile acid sequestrants were frequently effective in such patients.(22) (Fig. 4) There are other, although much less common, clinical applications for bile acid sequestrants, particularly the treatment of pruritus associated with chronic liver disease or biliary obstruction. Although ursodeoxycholic acid (UDCA) is often preferred for this indication, the majority of patients will achieve at least a partial response to a bile acid sequestrant within two weeks.(23) These agents have also been used as an adjunctive therapy for hyperthyroidism because of their ability to lower thyroxine levels by increasing L-thyroxine elimination. Although these are empirical uses for which supportive data are relatively modest, they are consistent with the expected effects of increasing the excretion of bile acids from the small intestine.
Bile Acid Sequestrants: First vs. Second Generation
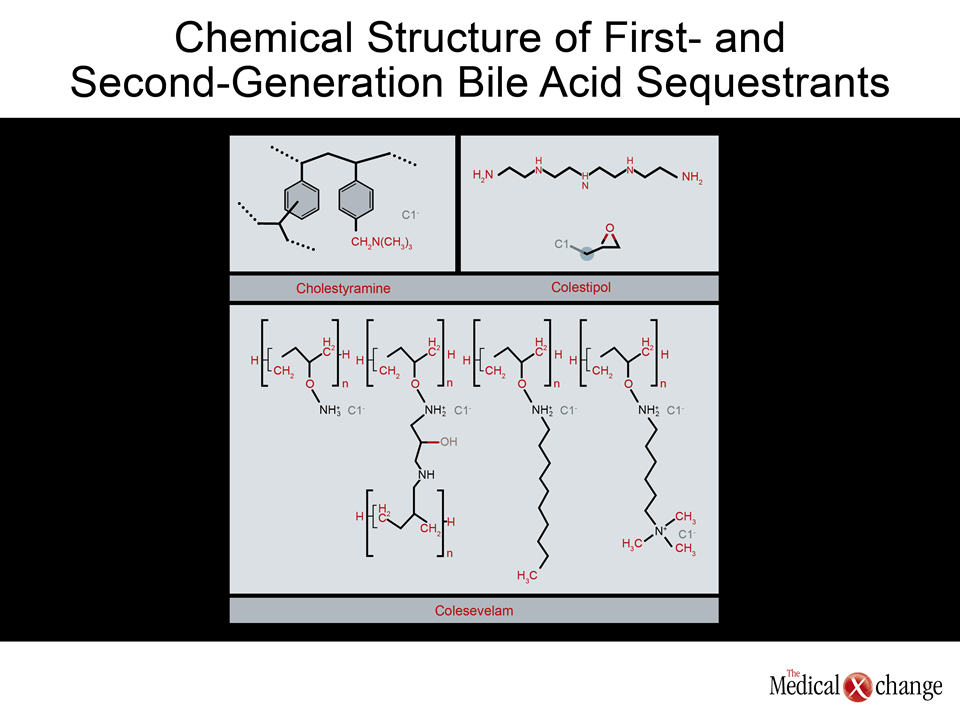
The bile acid sequestrants do not appear to be interchangeable. Cholestyramine and colestipol, which are generally considered to be the first-generation agents, have different chemical structures but comparable effects on bile acid absorption and, consequently, lipid reductions. Both of these agents are formulated in a powder that can be mixed with food or water. Both agents interfere with intestinal absorption of vitamins A and K as well as a substantial list of pharmacologic agents, including warfarin, penicillin, propranolol, and digoxin.(24) However, the greatest limitation of the first-generation agents has been the GI side effects, particularly bloating, abdominal pain, nausea, and flatulence. Colesevelam, a second-generation bile acid sequestrant, has been characterized as being four to six times more potent than the first-generation agents, which is attributed to greater binding on the target.(25) In addition, the chemical structure of colesevelam contains side chains that are credited with increasing its specific interaction with bile salts while reducing the likelihood of interactions with other agents (Fig. 5).(26)Its preference for hydrophobic chenodeoxycholic and deoxycholic bile acids relative to hydrophilic bile salts may also be important to its specificity of action on bile acid sequestration and the relatively low risk of drug-drug interactions.
For clinical application, the two most important advantages of the second-generation agent include a low relative rate of adverse events and the availability of a tablet formulation, both of which are relevant to compliance.
For clinical application, the two most important advantages of the second-generation colesevelam include a low relative rate of adverse events and the availability of a tablet formulation, both of which are relevant to compliance. Although adverse events common to other bile acid sequestrants can occur on colesevelam, they occur less frequently and with less severity relative to the first-generation agents.(27-28) While patients often complain of the taste and the powdered formulations of bile acid sequestrants, compliance rates of greater than 90% with colesevelam have been reported.(25) It is likely that many patients will prefer the convenience of a tablet over the extra step of employing a sachet formulation. Relative to powdered formulations of bile acid sequestrants, one of the most notable advantages of statins at the time of their introduction was an ability to achieve relatively large reductions in cholesterol with a single pill. Produced in a 625 mg tablet, colesevelam has a recommended starting dose of 3.75 g/day, which can be achieved with six pills taken once daily or three pills taken twice daily. Higher doses may be required to achieve maximum efficacy with this agent. However, much lower doses are typically effective for control of diarrhea related to bile acid malabsorption. In one patient series, adequate effect was achieved with as little as two pills but no more than six pills daily.(28) Underscoring the differences between bile acid sequestrants, colesevelam, unlike both cholestyramine and colestipol, has not been found to be more effective than placebo in controlling pruritus associated with chronic liver disease or biliary obstruction.(29) While UDCA is considered the first-line therapy in these patients with cholestyramine or colestipol employed as second-line or adjunctive agents,(30) this difference does introduce the issue of tailoring the use of bile acid sequestrants in those with multiple therapeutic targets. For example, while these agents might be attractive in patients with biliary obstruction and elevated cholesterol, bile acid sequestrants in general might be a particularly attractive therapy alone or in combination with statins for cholesterol lowering in individuals with both hyperlipidemia and diabetes due to their favourable effect on glucose metabolism.
Conclusion
Bile acid sequestrants have a long history in the treatment of both elevated cholesterol and GI disorders. The mechanisms, the risks, and the efficacy of these agents are well described. A tablet formulation of a second-generation agent is facilitating resurgence in the use of these agents that is being driven by growing rates of intolerance to statins and the increasing appreciation for the substantial prevalence of bile acid malabsorption. By reducing the risk of adverse events and improving the convenience of oral administration, the second-generation tablet has the potential to improve compliance essential to achieve the benefits documented over the past 50 years of clinical use.
References
1. Hylemon PB, Zhou H, Pandak WM, Ren S, Gil G, Dent P. Bile acids as regulatory molecules.J Lipid Res 2009;50(8):1509-20.
2. Bajor A, Gillberg PG, Abrahamsson H. Bile acids: short and long term effects in the intestine. Scand J Gastroenterol 2010;45(6):645-64.
3. Bijvelds MJ, Jorna H, Verkade HJ, et al. Activation of CFTR by ASBT-mediated bile salt absorption. Am J Physiol Gastrointest Liver Physiol 2005;289(5):G870-9.
4. Thomas C, Auwerx J, Schoonjans K. Bile acids and the membrane bile acid receptor TGR5–connecting nutrition and metabolism. Thyroid 2008;18(2):167-74.
5. Pumbwe L, Skilbeck CA, Nakano V, Avila-Campos MJ, Piazza RM, Wexler HM. Bile salts enhance bacterial co-aggregation, bacterial-intestinal epithelial cell adhesion, biofilm formation and antimicrobial resistance of Bacteroides fragilis. Microb Pathog 2007;43(2-3):78-87.
6. Ascaso JF. [Advances in cholesterol-lowering interventions]. Endocrinol Nutr 2010;57(5):210-9.
7. The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251(3):351-64.
8. Watts GF, Lewis B, Brunt JN, et al. Effects on coronary artery disease of lipid-lowering diet, or diet plus cholestyramine, in the St Thomas’ Atherosclerosis Regression Study (STARS). Lancet 1992;339(8793):563-9.
9. Fernandez G, Spatz ES, Jablecki C, Phillips PS. Statin myopathy: a common dilemma not reflected in clinical trials. Cleve Clin J Med 2011;78(6):393-403.
10. Bays HE, Goldberg RB, Truitt KE, Jones MR. Colesevelam hydrochloride therapy in patients with type 2 diabetes mellitus treated with metformin: glucose and lipid effects. Arch Intern Med 2008;168(18):1975-83.
11. Rosenstock J, Fonseca VA, Garvey WT, et al. Initial combination therapy with metformin and colesevelam for achievement of glycemic and lipid goals in early type 2 diabetes. Endocr Pract 2010;16(4):629-40.
12. Bays HE. Colesevelam hydrochloride added to background metformin therapy in patients with type 2 diabetes mellitus: a pooled analysis from 3 clinical studies. Endocr Pract 2011;17(6):933-8.
13. Wolkoff AW, Cohen DE. Bile acid regulation of hepatic physiology: I. Hepatocyte transport of bile acids. Am J Physiol Gastrointest Liver Physiol 2003;284(2):G175-9.
14. Tilson MD. Pathophysiology and treatment of short bowel syndrome. Surg Clin North Am 1980;60(5):1273-84.
15. Odunsi-Shiyanbade ST, Camilleri M, McKinzie S, et al. Effects of chenodeoxycholate and a bile acid sequestrant, colesevelam, on intestinal transit and bowel function. Clin Gastroenterol Hepatol 2010;8(2):159-65.
16. Nyhlin H, Merrick MV, Eastwood MA. Bile acid malabsorption in Crohn’s disease and indications for its assessment using SeHCAT. Gut 1994;35(1):90-3.
17. Sauter GH, Moussavian AC, Meyer G, Steitz HO, Parhofer KG, Jungst D. Bowel habits and bile acid malabsorption in the months after cholecystectomy. Am J Gastroenterol 2002;97(7):1732-5.
18. Hofmann AF, Poley JR. Role of bile acid malabsorption in pathogenesis of diarrhea and steatorrhea in patients with ileal resection. I. Response to cholestyramine or replacement of dietary long chain triglyceride by medium chain triglyceride. Gastroenterology 1972;62(5):918-34.
19. Jacobsen O, Hojgaard L, Hylander Moller E, et al. Effect of enterocoated cholestyramine on bowel habit after ileal resection: a double blind crossover trial. Br Med J 1985;290:1315-8.
20. Pattni S, Walters JR. Recent advances in the understanding of bile acid malabsorption. Br Med Bull 2009;92:79-93.
21. Hofmann AF, Mangelsdorf DJ, Kliewer SA. Chronic diarrhea due to excessive bile acid synthesis and not defective ileal transport: a new syndrome of defective fibroblast growth factor 19 release. Clin Gastroenterol Hepatol 2009;7(11):1151-4.
22. Taylor NS, Bartlett JG. Binding of Clostridium difficile cytotoxin and vancomycin by anion-exchange resins. J Infect Dis 1980;141(1):92-7.
23. Pusl T, Beuers U. Extrahepatic manifestations of cholestatic liver diseases: pathogenesis and therapy. Clin Rev Allergy Immunol 2005;28(2):147-57.
24. Reiner Z. Combined therapy in the treatment of dyslipidemia. Fundam Clin Pharmacol 2010;24(1):19-28.
25. Steinmetz KL. Colesevelam hydrochloride. Am J Health Syst Pharm 2002;59(10):932-9.
26. Bays H, Dujovne C. Colesevelam HCl: a non-systemic lipid-altering drug. Expert Opin Pharmacother 2003;4(5):779-90.
27. Aldridge MA, Ito MK. Colesevelam hydrochloride: a novel bile acid-binding resin. Ann Pharmacother 2001;35(7-8):898-907.
28. Puleston J, Morgan H, Andreyev J. New treatment for bile salt malabsorption. Gut 2005;54(3):441-2.
29. Kuiper EM, van Erpecum KJ, Beuers U, et al. The potent bile acid sequestrant colesevelam is not effective in cholestatic pruritus: results of a double-blind, randomized, placebo-controlled trial. Hepatology 2010;52(4):1334-40.
30. Kremer AE, Beuers U, Oude-Elferink RP, Pusl T. Pathogenesis and treatment of pruritus in cholestasis. Drugs 2008;68(15):2163-82.
Bile Acid Sequestrants: Putting a Unique Mechanism to Work
Bile acid sequestrants were initially developed for the treatment of hypercholesterolemia, but it is significant that essentially all the activity of these agents is confined to the gastrointestinal (GI) tract. The binding of bile acid in the intestine inhibits a key mechanism of cholesterol transport, but the GI applications of these agents are also considerable. Over the last decade, as statins have become the dominant treatment for elevated low density lipoprotein (LDL) cholesterol, GI applications have grown in relative importance. Although drugs in this class have been available for 50 years, the broad clinical applications deserve to be revisited. There has been a recent resurgence in the use of bile acid sequestrants for cardiovascular protection due to the intolerability of the very high doses of statins, but these agents are also relevant for use with several GI disorders.
Show review