gastroenterology
Canadian Digestive Diseases Week (CDDW) 2011
Convenience and Communication: Strategies to Enhance Treatment Compliance in Ulcerative Colitis
Vancouver – Despite the evidence that long-term therapy is beneficial, “real-world” compliance with a maintenance regimen among patients with ulcerative colitis needs improvement. Research presented here focusing on persistence and adherence to 5-ASA therapies examined the practical utility and efficacy of once-daily dosing as well as the need for comprehensive, individualized patient information and education on the disease and its management.
Ulcerative colitis (UC) is a chronic, sometimes progressive inflammatory bowel disease (IBD) characterized by relapse and remission of symptoms, including increased stool frequency and rectal bleeding. The disease may have a significant impact on physical well-being and overall quality of life. About 90% of Canadian patients have UC that is mild to moderate, based on the severity of symptoms during an exacerbation and endoscopic evidence of disease. First-line medical treatment is 5-aminosalicylic acid (5-ASA) administered orally and/or rectally. Several studies have demonstrated that once a UC flare has subsided and mucosal healing initiated, continuing 5-ASA therapy reduces the risk of relapse and promotes disease quiescence. Conversely, incomplete healing of inflamed mucosa appears to increase the risk of flares. Repeated flares engender higher hospitalization rates and treatment costs as well as poorer disease outcomes (e.g., the need for surgery) and lower quality of life.
Dosing Convenience May Play a Role
Simplifying or enhancing the convenience of treatment regimens in UC may be a useful strategy to promote long-term adherence.
Despite the evidence that long-term therapy is beneficial, “real-world” compliance with maintenance treatment is disappointing; numerous studies suggest that fewer than half of patients take their medications as prescribed. Some studies have determined that patients are inconvenienced by the high pill burden and dosing frequency of most 5-ASA therapies. A recent study conducted in 208 patients in the US (Can J Gastroenterol 2011;25[suppl A]: A130-1; 134-5) supports the notion that simplifying or enhancing the convenience of treatment regimens in UC may be a useful strategy to promote long-term adherence and reduce disease recurrence.
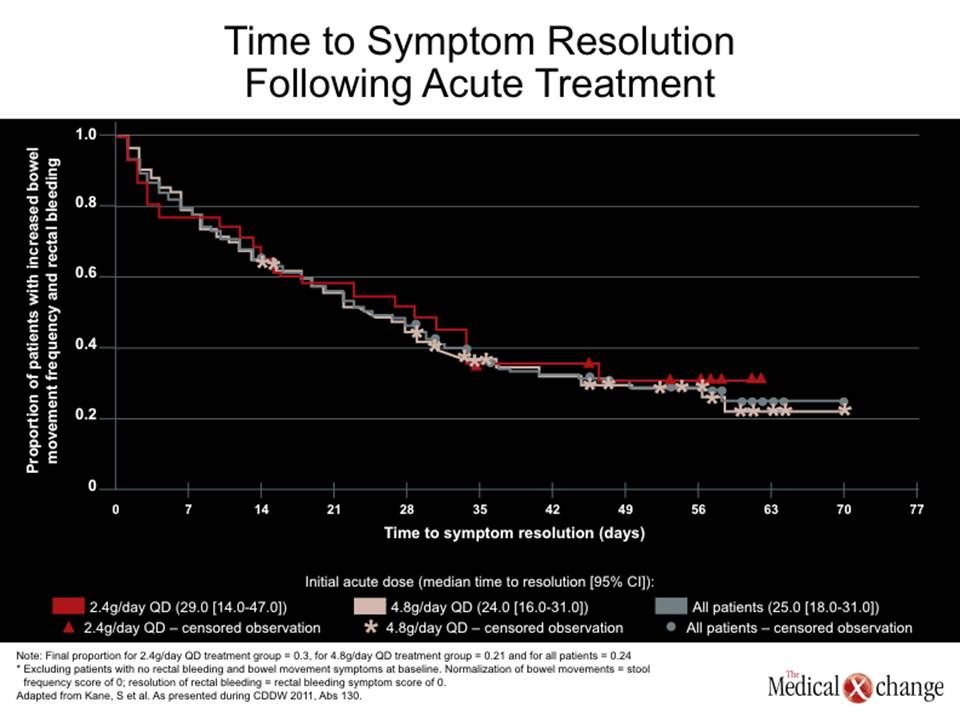
This open-label, multicentre phase IV trial, Strategies in Maintenance for Patients Receiving Long-term Therapy (SIMPLE), examined the clinical recurrence related to compliance in patients receiving multi-matrix system (MMX) mesalamine, an oral tablet given once daily for the maintenance of quiescent UC. Two doses were evaluated: 2.4 and 4.8 g/day. The study included adult patients with mild to moderate UC who had quiescent disease or achieved quiescence in an 8-week acute treatment phase; quiescence was defined as no rectal bleeding and no more than one bowel movement per day more than normal. Among patients taking part in the acute-treatment phase, 25% to 35% achieved resolution of rectal bleeding or bowel movement symptoms within seven days of starting MMX mesalamine treatment. The median time to combined symptom resolution was 25 days. (See Figure 1) (Fig. 1). Of the 138 patients who completed the maintenance phase of the trial, 79.2% and 77.3% were at least 80% compliant with therapy at 6 and 12 months, respectively.
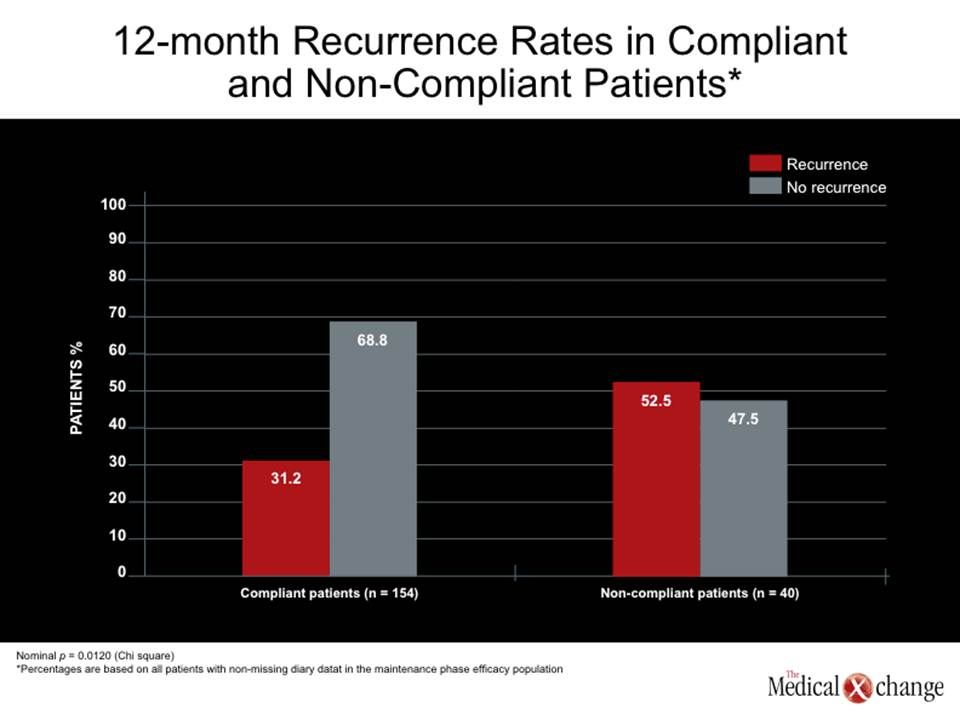
As shown below in Figure 2 (Fig. 2), a high rate of compliance was associated with significantly lower rates of disease recurrence over a one-year period (31% vs. 53% in noncompliant patients, P=0.012).
Overall, 77% of the patients were recurrence-free after 6 months of MMX mesalamine treatment and nearly two-thirds (64.4%) had no recurrence over the 12-month study duration.
Canadian Studies of Adherence and Persistence
Two studies conducted in Canadian patients also suggest that patients’ adherence and persistence with once-daily oral therapy is superior to that of 5-ASA treatments requiring more frequent dosing.
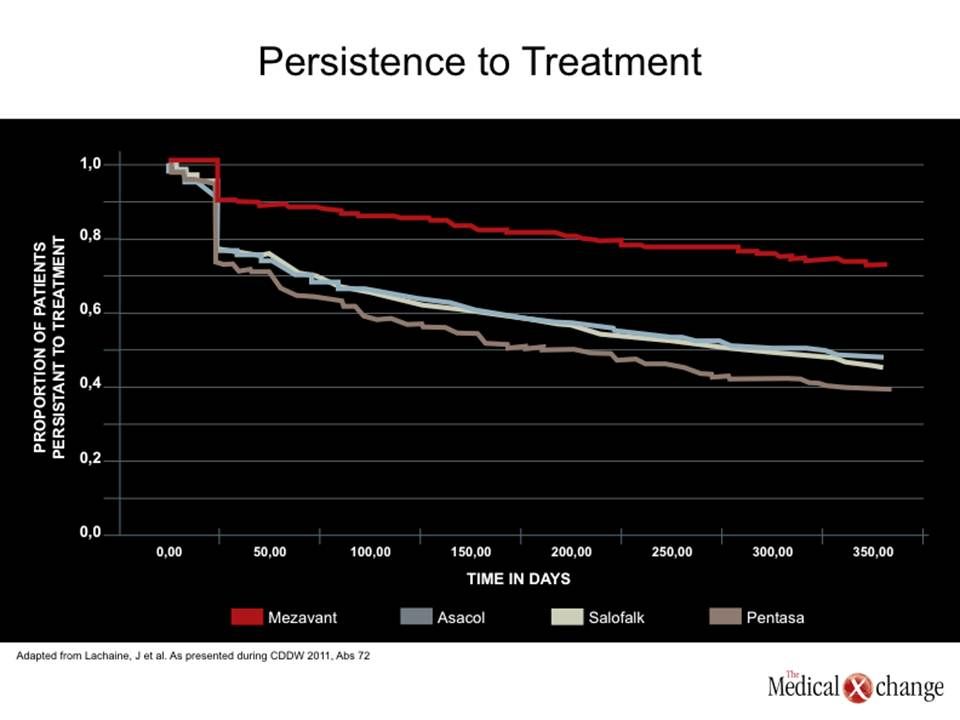
A five-year retrospective analysis of prescription claims from the Quebec provincial public health plan (Régie de l’assurance maladie du Québec [RAMQ]) database examined compliance among 1827 adults newly prescribed one of several mesalamine formulations (Can J Gastroenterol 2011;25[suppl A]:A72). The investigators determined that the proportion of patients who were at least 80% adherent to the MMX formulation of mesalamine was approximately double that of all other formulations (46.3% vs. 23.5% to 26.3%, P<0.001). Similarly, as illustrated in Figure 3 (Fig. 3), persistence with treatment over a one-year period was higher with MMX mesalamine (70.2% vs. 35.0% to 43.4%; P< 0.001).
The Quebec data agree with those of a six-month follow-up of treatment adherence and persistence among 15,545 patients throughout Canada who received 5-ASA therapy via private drug plans (Can J Gastroenterol 2011;25[suppl A]:A142). Seventy percent of patients receiving the once-daily MMX formulation of mesalamine continued therapy beyond their initial claim, compared with 45% to 52% with other formulations (P<0.0001). After two to three months, persistence with therapy was 62% with MMX mesalamine and ranged from 39% to 45% with other formulations. After six months, the rate was 44% with MMX mesalamine and less than 30% for the other agents.
“Once-daily dosing is an important strategy is ensuring compliance and probably the simplest and most significant advance in the field to help patients overcome compliance issues,” observed Dr. Remo Panaccione, Director of the Inflammatory Bowel Disease Clinic and Associate Professor of Medicine, University of Calgary.
Potential Factors in Noncompliance
Some studies have indicated that younger patients are less likely to be adherent than older patients. “We are dealing principally with young patients who don’t want to take medicine when they are feeling well. They are busy and have other things in their lives that take precedence,” noted Dr. Panaccione. This finding may also be explained by shorter disease duration and/or less intense disease activity or fewer experiences of complications in younger patients, as well as the desire to avoid the stigma of illness. The experience of adverse effects with treatment or simply having concerns about side effects may also reduce compliance.
Investigators from Toronto and Baltimore reported here that many patients with IBD try complementary and alternative medicine (CAM) in addition to their prescribed therapy. In this small study (55 patients), there was a trend for CAM users to forget to take their conventional medications, although overall compliance was not significantly affected (Can J Gastroenterol 2011;25[suppl A]:A207).
In an era in which most people look for health information on the Internet, physicians must be aware of the potential power of “misinformation, which in turn may potentially lead to suboptimal management,” according to researchers from the University of Ottawa. Of 89 patients surveyed, 56% said the Internet was their principal source of information on IBD; however, only 29% were consulting a website that is considered to have high-quality information (Can J Gastroenterol 2011;25[suppl A]:A218).
Communication and Education
“Patients should understand the concepts of induction and maintenance of remission and the possible ramifications of coming off therapy.”
These studies help stress the necessity of open dialogue between the physician and the patient and individualized education on UC and its management. “Education is an important cornerstone in ensuring compliance so that patients understand the reason they need to take therapy when they are feeling well – the concepts of induction and maintenance of remission – and the possible pitfalls or ramifications of coming off therapy such as increased risk off flares, hospitalization, and possibly surgery…. It is also important to let patients know that we realize that there is a temptation to be noncompliant, that we understand this may happen, and that it is important to know if non-compliance [occurs] because it may affect treatment decisions downstream,” commented Dr. Panaccione. Individualized selection of the therapeutic regimen should take into account factors that may enhance compliance, such as dosing convenience.