Psychiatry
164th Annual Meeting of the American Psychiatric Association
Adolescents with ADHD: Long-term Therapy is Safe and Effective
Honolulu – Attention deficit hyperactivity disorder (ADHD) is commonly misperceived as a condition of childhood. Yet, a large proportion of individuals have persistent symptoms of ADHD into adolescence and adulthood. Left untreated, the symptoms can exert particularly negative effects in adolescents, such as learning difficulties and emotional problems that can have life-long adverse consequences, including increased drug use, teen pregnancy, and car accidents. Adolescents with ADHD may benefit from long-term therapy with a stimulant agent, but the potential adverse effects and long-term efficacy of chronic use of such drugs has not been well documented. This report summarizes results of a study on a new, long-term stimulant for teenagers with moderately severe ADHD.
A long-term experience with lisdexamfetamine dimesylate (LDX) in adolescents with attention-deficit hyperactivity disorder (ADHD) demonstrated that the long-acting agent is effective at exerting persistent control over symptoms of ADHD, with a safety profile similar to that seen in short-term studies in this population.
As reported by Dr. Ann C. Childress, Center for Psychiatry and Behavioral Medicine, Las Vegas, Nevada, “It has a safety and efficacy profile consistent with other studies in children and adults [Wigal SB, Kollins SH, Childress AC, Adeyi B. Child Adolesc Psychiatry Ment Health. 2010 Dec 14;4:32; Adler LA, Goodman DW, Kollins SH, et al. J Clin Psychiatry. 2008 Sep;69(9):1364-73]. There are some modest increases in bloodpressure and pulse in this long-term study.”
Adolescents enrolled in a multicentre study of LDX maintained significant improvements through one year in core symptoms of ADHD, consistent with results seen in studies of the drug in children and adults, according to Dr. Childress, who presented these results at this year’s American Psychiatric Association meeting.
A long-acting prodrug stimulant, LDX is indicated for the treatment of ADHD in children, adolescents, and adults in Canada and the United States. Relative to other stimulants, the agent has a long duration of action designed to permit control of symptoms over a longer period of the day. This is potentially important because ADHD has an important negative impact on social and family interactions that may produce as great or greater morbidity than impairment in school performance. Widely studied in younger children, the efficacy of LDX in adolescents was outlined in a recently published 4-week, randomized, double-blind, placebo-controlled parallel group trial (J Am Acad Child Adolesc Psychiatry. 2011 Apr;50(4):395-405. Epub 2011 Mar 3). These data build on those findings.
“This is a long-term safety study, and LDX looks like other stimulants,” observed Dr. Childress. She characterized this as “good news,” because of the longer duration of action of LDX.
In the prior short-term study, adolescents from ages 13 through 17 years were randomized to either placebo or LDX in doses of 30, 50, or 70 mg per day in a forced-dose titration fashion. Participants had to have at least moderately symptomatic ADHD, defined as a score on the ADHD Rating Scale IV (ADHD-RS-IV) of 28 or greater.
This study was a 52-week, open-label extension of the original 4-week, parallel group, double-blind, placebo controlled, fixed-dose study. The current study began with a 4-week dose-optimization phase in which LDX was titrated up or down at 20 mg increments once weekly from a 30 mg baseline dose, to a maximum dose of 70 mg/day. In the 48-week maintenance phase, patients were seen once monthly, and optimized doses were either continued or further titrated up or down as needed, up to the maximum 70 mg/day dose.
Safety and Efficacy Outcomes
Safety endpoints included treatment-emergent adverse events (TEAEs), defined as adverse events (AEs) that worsened from the first day of treatment in the current study until the third day after the end of therapy, vital signs (including changes in systolic [SBP] and diastolic blood pressure [DBP] from baseline), electrocardiograms, laboratory values, and the Columbia-Suicide Severity Rating Scale (C-SSRS).
The primary efficacy endpoint was change from baseline (of the original 4-week study) in ADHD-RS-IV scores. Secondary measures were improvement in severity in the Clinical Global Impressions-Improvement (CGI-I), and scores on the Youth Quality of Life-Research Version (YQOL-R).
A total of 269 adolescents were enrolled, 265 were included in the safety and efficacy results, and 156 completed the 48-week maintenance phase. Reasons for discontinuation included AEs in 6.7% of participants, and refusal to participate further in 11.5%.
Safety Results
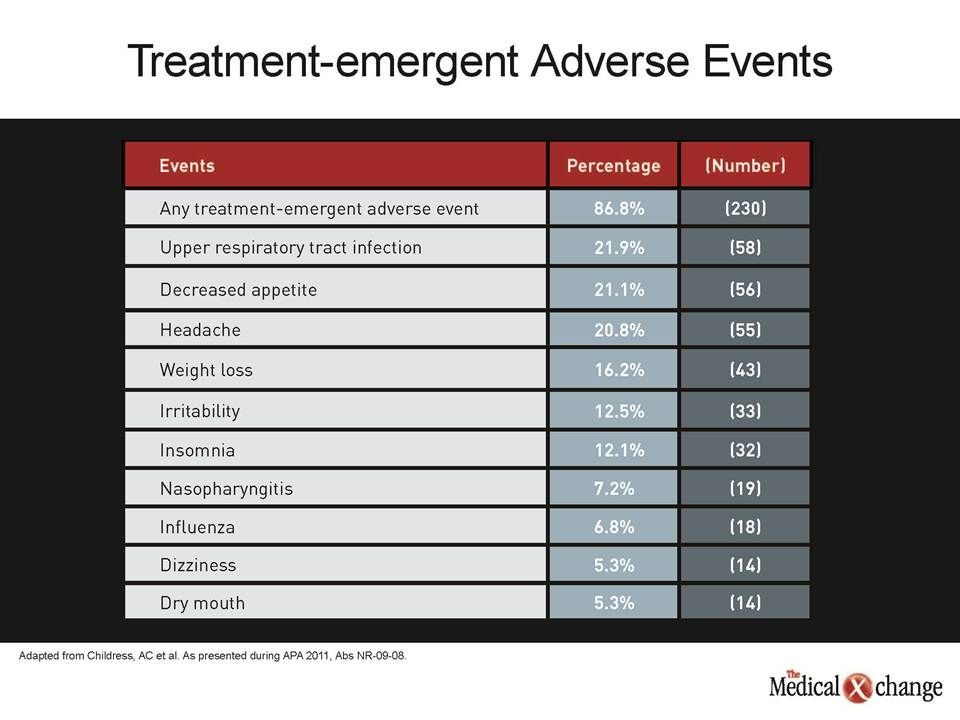
The safety analysis showed that TEAEs occurring in 5% or more of participants included (in descending order of frequency) upper respiratory tract infections in 21.9%, decrease in appetite in 21.1%, headache in 20.8%, weight loss in 16.2%, irritability in 12.5%, insomnia in 12.1%, nasopharyngitis in 7.2%, influenza in 6.8%,and dizziness and dry mouth in 5.3% each. Most of the events were mild or moderate in severity, the authors noted (Table 1).
There were 15 serious AEs reported in 10 subjects. These included, in order of frequency, 4 cases of syncope, 2 of aggression, and 1 each of ectopic pregnancy, hydrocele, joint sprain, pelvic fracture, pneumonia, testicular torsion, traumatic liver injury, vasovagal syncope, and wrist fracture.
Thirty-three participants (12.5%) met pre-determined SBP outlier criteria of 120 mm Hg or higher and a change from baseline of at least 10 mm Hg; 4 (1.5%) had an SBP of 140 mm Hg or greater at study end. Twenty subjects (7.5%) met the DBP outlier criteria of 80 mm Hg or higher with an increase from baseline of 10 mm Hg or greater; no participants had a DBP exceeding 90 mm Hg at study end. Eleven participants met the pulse outlier criteria of 100 or more beats-per-minute (BPM) with an increase from baseline of at least 15 BPM; none had a pulse rate of 120 BPM or more at study end. There were only a few changes in z-score weight, height and BMI.
Efficacy Results
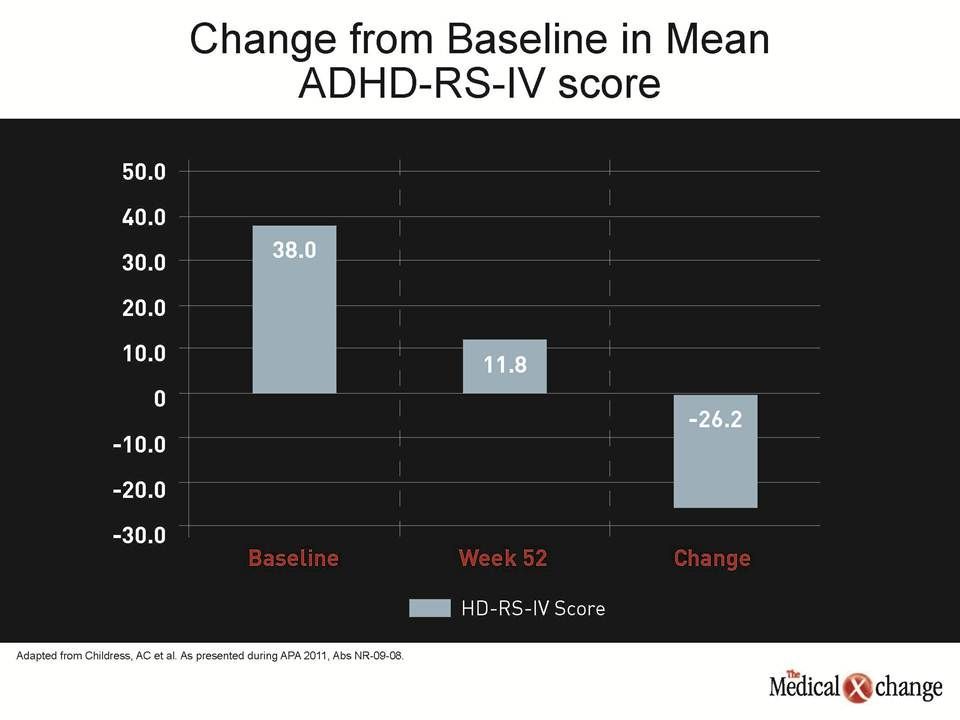
While the main objective of the study was safety, the study did reconfirm the efficacy of LDX. Over the course of follow-up, the mean change in ADHD-RS-IV total score was -26.2 (standard deviation [SD] 9.75; 2-sided 1 sample t-test P<0.001). The baseline mean score was 38 (7.00) (Fig. 1).
Moreover, at all follow-up visits, there were significant changes in sub-scale scores of inattention (change score of -15.1 [6.05] with a baseline of 22.6 [3.35], P<0.001), and hyperactivity/impulsivity (change score of -11.1 [5.89] with a baseline of 15.4 [6.9], P<0.001). Improvement in CGI-I scores of 1 or 2 was seen in 91.2% at the end of the dose-optimization phase, 97.8% at week 28, 98.1% at week 52, and 87.2% at the maintenance-phase endpoint.
Not least important, the participants also reported an improved quality of life on the YQOL-R questionnaire. Mean scores on the 100-point scale, with higher scores reflecting improvement in quality of life, increased from 79.8 (11.28) at baseline, to 84.6 (9.36) at week 28, 84.9 (10.04) at week 52, and 83.9 (11.0) at endpoint.
Conclusion
ADHD is a chronic disorder that begins in childhood but typically persists, often producing significant symptoms during adolescence and into adulthood. While the initial focus of ADHD treatment was on improving attention and controlling disruptive behaviour in the classroom, it is now well accepted that the focus on school performance is too narrow. ADHD can impair the ability to participate in extracurricular activities and form social bonds while producing family discord. The consequences of ADHD in teen years can include a variety of risk-taking behaviour that can have significant adverse consequences for development and adult wellbeing. The evidence that long-acting ADHD therapies can be used safely long-term in adolescents has important implications for outcome.