hypertension
American Society of Hypertension (ASH) 26th Annual Scientific Meeting and Exposition
Fixed-Dose Combinations: Comparing Similar Strategies when Degree of Blood Pressure Lowering is Important
New York – Due to the frequency with which hypertensive patients require more than one therapy to reach treatment goals, fixed-dose drug combinations have been widely embraced for convenience, but the efficacy of single-pill combinations are not necessarily comparable even when the component drug classes are the same. In a double-blind study conducted with a new angiotensin receptor blocker (ARB), a single-pill fixed-dose combination with a diuretic was more effective for reducing both clinic and ambulatory blood pressures than a similar coupling of agents from the same classes. The fixed-dose trial is consistent with a series of studies conducted previously with the same ARB, indicating that the features of this agent are unique relative to earlier generation drugs from the same class. The greater likelihood of reaching therapeutic targets has major implications for reducing the risk of cardiovascular events.
Antihypertensive agents have a broad array of characteristic differences, but blood pressure lowering efficacy has typically been of the same general magnitude, particularly among agents from within the same drug class. A series of studies with a new angiotensin receptor blocker (ARB) called azilsartan medoxomil (AZL-M), the most recent of which were conducted with the diuretic chlorthalidone (CLD) in a fixed-dose combination, have broken the pattern. In the largest of the studies so far, AZL-M/CLD was directly compared to olmesartan (OLM) plus the diuretic hydrochlorothiazide (HCTZ). Presented as a late breaker at the ASH 2011 meeting, the consistency of advantage was a key finding.
ASH 2011 Late Breaker: Forced-dose Study
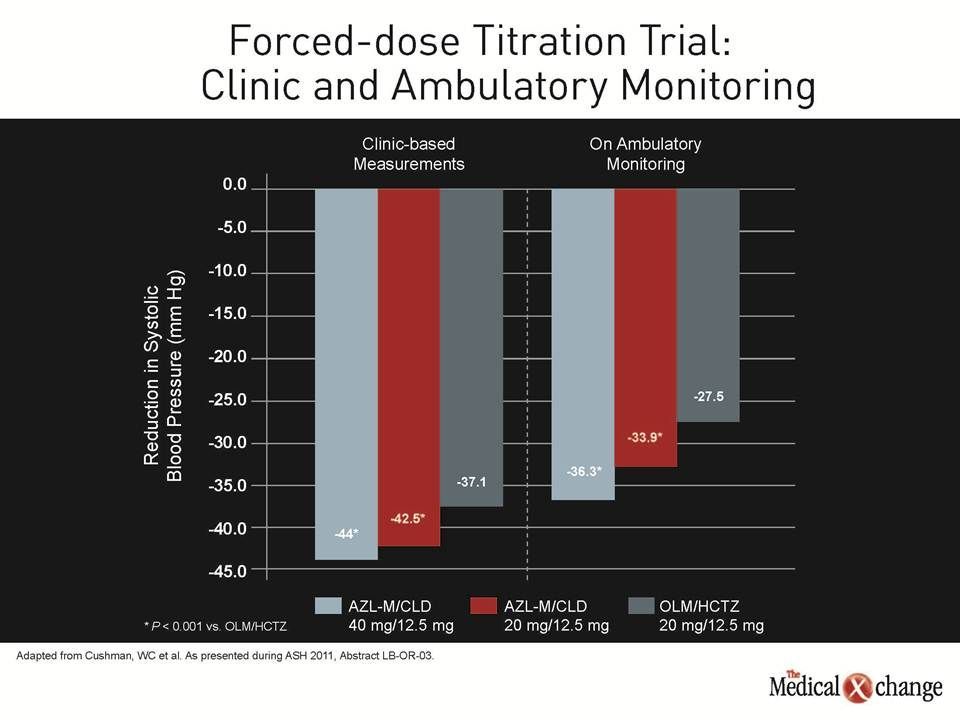
“The reductions in blood pressure on the AZL-M-based combination were greater for systolic and diastolic measures whether in the clinic or on ambulatory monitoring, and the differences were highly statistically significant,” reported Dr. William C. Cushman, Professor of Preventive Medicine, University of Tennessee College of Medicine, Memphis. He indicated that this is the first well-controlled, multicentre, forced-dose randomized study to show superiority for one ARB over another in a fixed-dose combination.
“The reductions in blood pressure on the AZL-M-based combination were greater for systolic and diastolic measures whether in the clinic or on ambulatory monitoring, and the differences were highly statistically significant.”
The results were, however, predicted by a series of studies that preceded this head-to-head comparison. AZL-M, which has been approved in the United States and is under regulatory review in Canada, is a long-acting ARB that has been associated with uncommon blood pressure lowering effect. Summarizing the series of studies conducted to date, Dr. Cushman reported that “we generally see an incremental 5 to 7 mm Hg reduction in blood pressures on AZL-M relative to the other ARBs.” He suggested that OLM was a reasonable choice for a head-to-head comparison because of the perception that this may be the most potent of the ARBs prior to AZL-M even if comparative studies with this agent relative to other ARBs have been inconsistent.
In this large multicentre forced-titration trial, 1070 patients with stage 2 hypertension were randomized to one of two starting doses of AZL-M (20 mg or 40 mg), both administered with 12.5 mg CLD in a single-pill combination, or 20 mg OLM in a single-pill combination with 12.5 mg HCTZ. After four weeks, the doses of the ARBs were doubled while the diuretic doses remained the same. After an additional four weeks, the dose of the diuretic was doubled. Efficacy and safety were compared at the end of 12 weeks on therapy.
Compared to the 37.1 mm Hg reduction in systolic blood pressure achieved with the OLM-based therapy in clinic-based measurements, the lower dose of AZL-M produced an additional 5.4 mm Hg reduction (P<0.001) and the higher dose produced an additional 6.9 mm Hg reduction (P<0.001). On ambulatory monitoring, the reductions were less on all three agents, but the magnitude of the increased reduction with AZL-M was at least as good. Compared to the 27.5 mm Hg reduction on OLM, the lower dose of AZL-M provided a 6.4 mm Hg addition reduction (P<0.001) and the higher dose provided an additional 8.8 mm Hg reduction (P<0.001) (Fig. 1). The reductions in diastolic blood pressure on both doses of AZL-M relative to OLM were highly statistically significant (P<0.001).
While serious adverse events were slightly higher on the highest dose of the AZL-M-based therapy relative to OLM- based therapy (2.8% vs. 2.2%), the rates were lowest on the lower dose of the AZL-M-based therapy (0.3%). The rate of adverse events leading to discontinuation were slightly higher on the lower dose of the AZL-M-based therapy relative to the OLM-based therapy (8.7% vs. 7.1%), but highest overall on the higher dose of the AZL-M-based therapy (14.8%). In general, however, Dr. Cushman characterized the arms as well tolerated.
“When you use a forced-titration scheme, then it sets up the most effective drugs for more side effects because patients are required to go up in dose whether or not there is a clinical need,” observed Dr. Cushman. He said that the forced-titration investigation was conducted in order to provide an opportunity to compare the antihypertensive effect in a rigid dosing strategy.
Titration-to-Goal Study Shows Similar Results
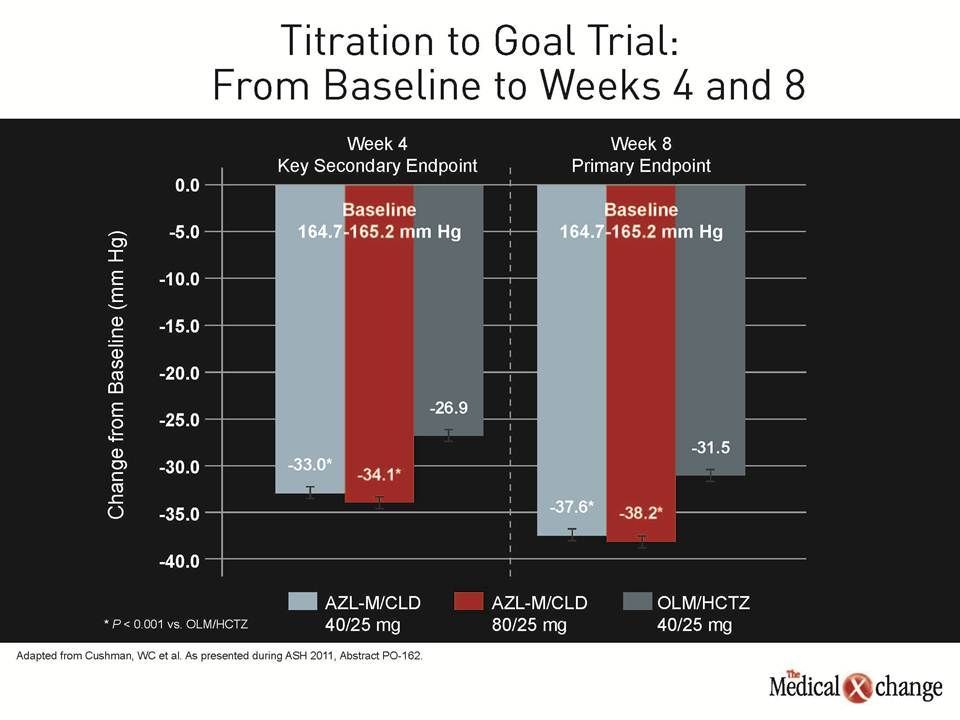
However, results of a titration-to-goal study produced very similar results. In that study, also presented at ASH 2011 by Dr. Cushman, 1085 patients were randomized to the same two initial doses of AZL-M plus CLD or to OLM/HCTZ in fixed-dose combinations. At four weeks, patients starting on the lower dose of the AZL-M-based therapy were eligible for 40 mg AZL-M plus 25 mg CLD, those on the higher dose were eligible for 80 mg AZL-M plus 25 mg CLD, and those randomized initially to 20 mg OLM and 12.5 mg HCTZ were allowed to receive 40 mg and 25 mg of those two agents, respectively. Efficacy and safety were evaluated at four and then eight weeks.
At week four, the OLM-based therapy lowered systolic blood pressure 26.9 mm Hg from baseline, but the lower dose of the AZL-M-based therapy produced another 6.1 mm Hg reduction and the higher produced an additional 7.1 mm Hg reduction (both P<0.001 vs. OLM-based therapy). At 8 weeks, the reduction in systolic blood pressure on the OLM-based therapy was 31.5 mm Hg, which was reduced an additional 6.1 mm Hg and 6.7 mm Hg, respectively, in those initially randomized to the lower- and higher-dosed AZL-M-based therapy (all P<0.001 vs. OLM) (Fig. 2).
The proportion of patients randomized to an OLM-based therapy who reached the systolic target blood pressure target at week 8 was 64.6% compared to 76% of both AZL-M- based groups (P<0.001) and the relative advantage for the AZL-M- based therapy was similar for the diastolic goals. For both goals together the proportions were 54.7% for OLM-based therapy versus 69.4% and 68.9%, respectively (P<0.001) for the lower and higher of the AZL-M-based therapies. Yet, despite these differences, the proportion of uptitrated at four weeks was lower in the AZL-M-based groups. “What we are seeing with AZL-M, whether or not it is combined with a diuretic, is that this is a more effective ARB for lowering blood pressure,” Dr. Cushman said. “I think this would be basically required of a new drug in this class, because otherwise why develop another ARB?”
Conclusion
A newly developed ARB, AZL-M (azilsartan medoxomil), has been associated with greater blood pressure lowering efficacy in a series of head-to-head studies with other agents within this class, including a new series of studies conducted in fixed-dose combinations. The agent appears to provide a safety and tolerability of the same general scale as that observed with previous ARBs. Most importantly, as demonstrated in the dose-titration trial, this agent can be used more effectively than a comparable ARB/diuretic combination for reaching treatment goals.