oncology
2011 American Society of Clinical Oncology (ASCO) Annual Meeting
Phase III Trials Redefine Optimal Therapy in Gastroenterological Cancers
Chicago – Several large trials, including late breakers, presented at the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting have helped refine current standards for the treatment of cancers in the gastrointestinal (GI) tract. It is noteworthy that several agents resurfaced in effective regimens across different sites along the GI tract. According to the new data, targeted therapies, such as monoclonal antibodies (mABs) and tyrosine kinase inhibitors (TKIs) do appear to have a role in selected populations, but the new data are more remarkable for their support of cytotoxic agents. Overall, the innovations in treatment appear more likely to build on the advantages of current standard regimens, such as FOLFOX (leucovorin, 5-fluorouracil, and oxaliplatin) in colon cancer, than to replace these strategies. Two of the most important studies in regard to understanding the current direction of state-of-the-art therapy were conducted in the adjuvant setting for colon cancer, but preoperative therapy in rectal cancer was another area in which there are significant new data.
Late Breakers at ASCO Show Great Promise
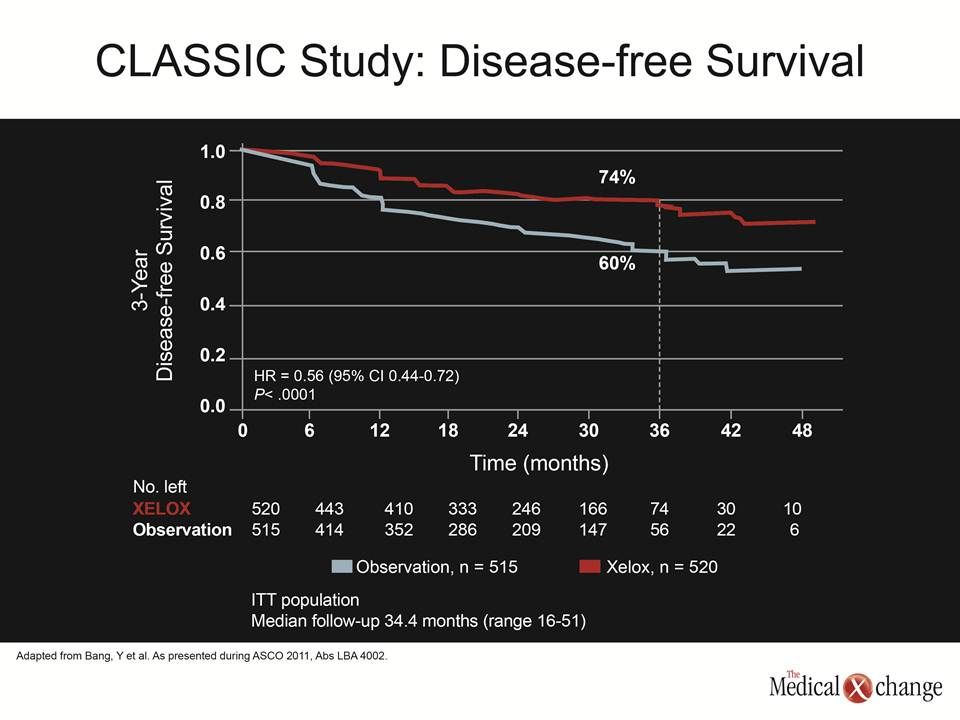
The phase III CLASSIC study, a late breaker at the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting, was among a series of studies that have the potential to alter treatment standards. In this study, the goal was to improve survival in patients with operable gastric carcinoma with adjuvant therapy. Currently, recurrence rates are in the range of 40% to 80% after D2 resections even with adequate surgical margins. In this multinational study, 1035 patients were randomized to no adjuvant therapy or 8 cycles of XELOX (capecitabine 1000 mg/m2 bid for days 1 to 14 every 3 weeks and oxaliplatin 130 mg/m2 on day 1 every three weeks) after a D2 resection. The interim results led the data and safety monitoring committee to recommend an early report.
Currently, recurrence rates are in the range of 40% to 80% after D2 resections even with adequate surgical margins.
“CLASSIC demonstrates superior efficacy for adjuvant XELOX versus observation alone following D2 resection,” reported Dr. Yung-Jue Bang, Seoul National University College of Medicine, Korea. The follow-up is not yet sufficiently mature to show an advantage for overall survival (OS), but there was a significant advantage for the adjuvant XELOX regimen for disease-free survival (DFS), the primary endpoint, and “this benefit was observed across all disease stages.” In this study, about half of the patients had stage II disease, slightly more than one third had stage IIIA disease, and almost all of the remaining had stage IIIB disease. The nodal status was N1/2 in about 90% of the patients. The remaining was N0. Nearly half of the resections were performed in the antrum with most of the remaining performed in the gastric body. Patients, who were eligible if they were free of macroscopic or microscopic disease after surgery, were required to have a Karnofsky performance status of at least 70%, and they had to be randomized within six weeks of surgery. The difference in the recurrence rates were large with 30.1% occurring in the observation arm and 18.1% in the XELOX arm. This translated into a DFS of 74% for XELOX vs. 60% for observation, producing a relative risk reduction of 44% (HR 0.56, 96% CI 0.44 – 0.72; P<0.0001) (Fig. 1). The relative reductions in recurrence were very similar and statistically significant across all stages of disease and when patients were stratified by age ≥65 years or younger. Not all subgroups showed a statistically significant benefit, but all trended in a favourable direction.
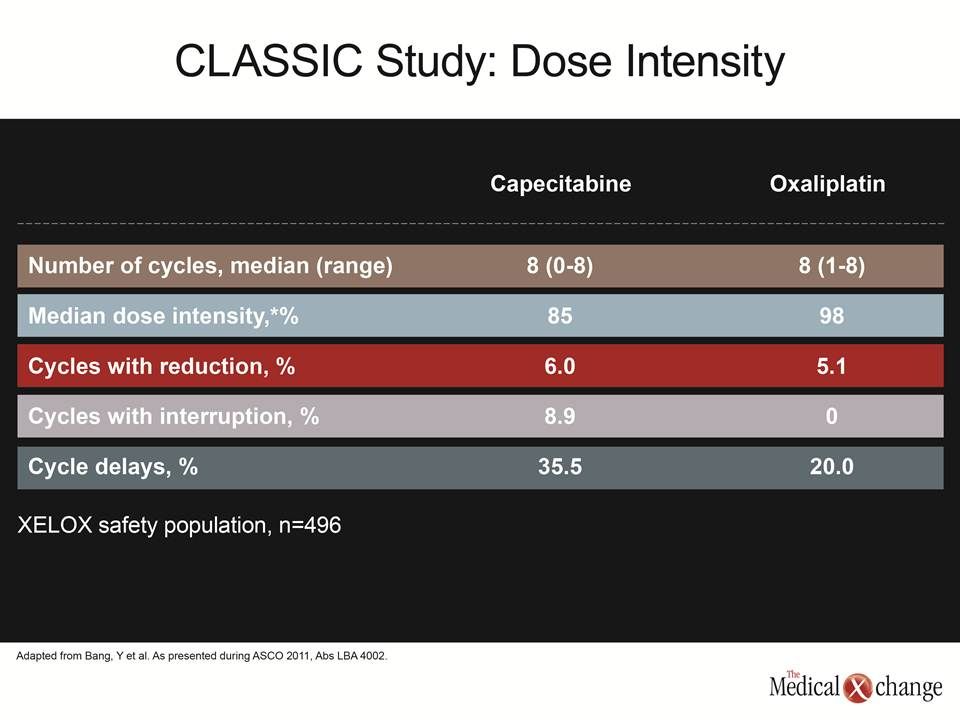
XELOX was reasonably well tolerated, producing no unexpected adverse events. The planned cycles and median number of cycles administered was the same.
XELOX was reasonably well tolerated, producing no unexpected adverse events. The planned cycles and median number of cycles administered was the same. Only 8.9% of cycles with capecitabine and 0% of cycles with oxaliplatin required dose interruption. The median dose intensity, which represents the proportion of drug received for the proportion planned, was 85% for capecitabine and 98% for oxaliplatin (Table 1). While grade 3 or 4 toxicities were more common on XELOX than on observation (54% vs. 6%), a substantial proportion of these were due to neutropenia or thrombocytopenia (30% vs. 0%). All the other grade 3 or higher events, such as nausea (8%) and diarrhea (2%) occurred in less than 10% of those randomized to XELOX. It is notable that the protection from recurrences was consistent across all sites when totalled numerically, including loco-regional (23 vs. 44), peritoneal (48 vs. 58), and distant (44 vs. 78). Patients will continue to be followed to evaluate a survival benefit. In follow-up so far, XELOX has been associated with a non-significant trend for a 26% reduction in death (HR 0.74, 95% CI 0.53 – 1.03; P=0.0775). While survival benefits are generally required to label any therapy a new treatment standard in oncology, Dr. Bang concluded that these data, which “support the use of adjuvant XELOX for gastric cancer,” have already altered current practice at his institution. The consistency across stages in the CLASSIC study is reassuring because there has been controversy about whether the benefit of adjuvant oxaliplatin is reserved primarily for the highest risk patients. In another presentation at ASCO that combined data from four National Surgical Adjuvant Breast and Bowel Project (NSABP) studies with more than 8,500 colon cancer patients, the addition of oxaliplatin to 5-fluorouracil/leucovorin appeared to yield a smaller benefit in stage II than stage III disease. However, both the lead author of the study, Dr. Greg Yothers, Department of Biostatistics, University of Pittsburgh, Pennsylvania, and the ASCO-invited discussant for this and several other presentations, Dr. Howard S. Hochster, Director of the GI Oncology Center, Yale University Cancer Center, New Haven, Connecticut, reported that an interaction between oxaliplatin and disease stage is unlikely and not supported by this or other evidence. Rather, other reasons for a lower level of benefit in stage II patients, such as lack of statistical power and high rates of non-cancer related deaths, are suspected. Indeed, while acknowledging that wide confidence intervals prevented significance, Dr. Hochster pointed to “a strong overall effect for oxaliplatin in both stages II and III on OS, DFS, and time to relapse [TTR]” on the basis of median improvements in hazard ratios. While he suggested that the toxicity of aggressive chemotherapy regimens may not be warranted in low-risk stage II patients, he noted that there is a large body of evidence, including that generated from the NSABP studies, that clinicians should “consider using FOLFOX for high-risk stage II colon cancer with appropriate discussion [with the patient].”
The AVANT Study: Disappointing Data
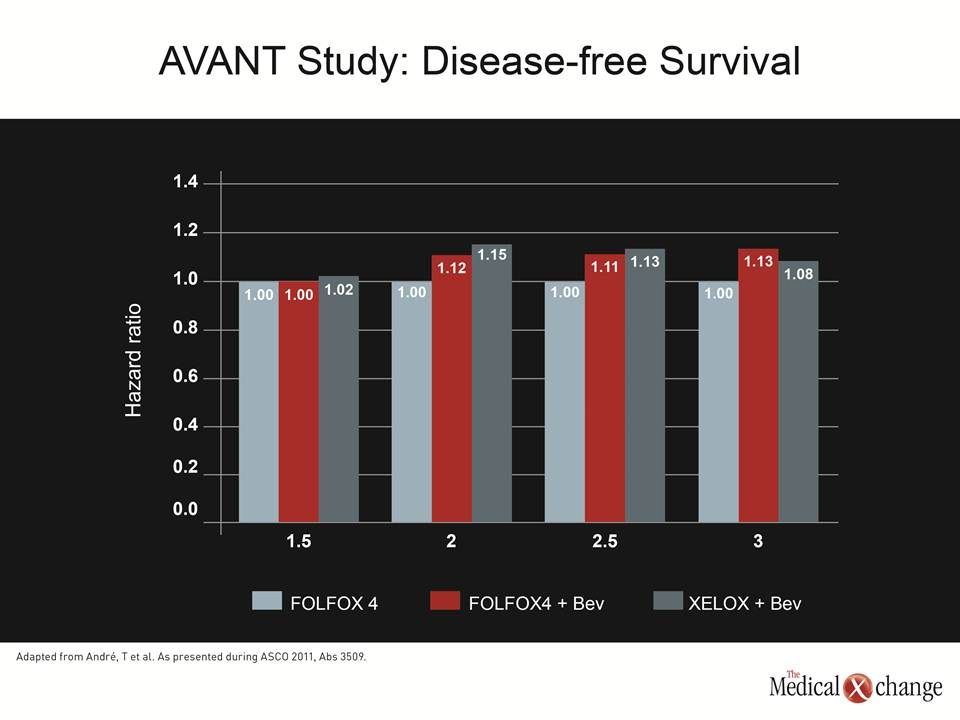
In colon cancer, adjuvant chemotherapy after resection has long been the standard with several studies planned or on-going to build on established regimens. The most recent, another multinational phase III trial called AVANT, tested the ability of the monoclonal antibody (mAB) bevacizumab to improve DFS rates achieved with either FOLFOX4 or XELOX. The results were disappointing. Although results were presented at the ASCO 2011 Gastrointestinal Cancers Symposium in January of this year, the secondary analyses presented at the 2011 ASCO Annual Meeting were no more promising. Statistically, there were no differences between the arms, although patients tended to do worse with bevacizumab. “Even in the subgroup analyses, we did not see any signal for a benefit from bevacizumab, although it is possible that biomarker studies from tissue samples may help us understand more,” reported Dr. Thierry André, Pitié-Salpêtrière Hospital, Paris, France. On the basis of the study hypothesis, which predicted an improvement in DFS with bevacizumab, Dr. André characterized this as “a negative study.” In AVANT, 3,541 patients with high-risk stage II or III colon cancer were randomized to six months of FOLFOX4 (85 mg/m2 of oxaliplatin on day 1 concurrently with 200 mg/m2/day of leucovorin, followed by bolus 400 mg/m2 of 5-fluorouracil and then a 22-hour infusion of 600 mg/m2 5-fluorouracil for two consecutive days on a cycle repeated every 2 weeks), FOLFOX4 plus bevacizumab given once weekly, or XELOX plus bevacizumab once weekly. In addition to the primary endpoint, the study included secondary analyses of OS and safety. With a median duration of 48 months of follow-up, FOLFOX4 alone provided the best DFS. Relative to FOLFOX4, FOLFOX4 plus bevacizumab produced a non-statistical 17% reduction in DFS (HR 1.17, 95% CI 0.98 – 1.39), while XELOX plus bevacizumab produced a non-statistical 7% reduction in DFS (HR 1.07, 95% CI 0.90 – 1.28). When assessed by time to DFS, the numerical advantage of FOLFOX4 was observed for the duration of the study. There were no differences in DFS assessed by stage of disease. When calculated as time to recurrence or new occurrence plus death, the same trends were observed. The interim analysis for OS even showed a slight statistical advantage for FOLFOX4 over FOLFOX4 plus bevacizumab (HR 1.31, 95% CI 1.03 – 1.67; P<0.05) (Fig. 2). “Why was it that bevacizumab was ineffective?” asked Dr. Hochster. He suggested that characteristics of an effective adjuvant therapy are likely to be different than they are for an effective agent in metastatic disease, which is where bevacizumab has previously shown activity. He indicated that this study provides the basis for rethinking the role of mABs at different stages of colon cancer.
PRIME Study: Promising Data
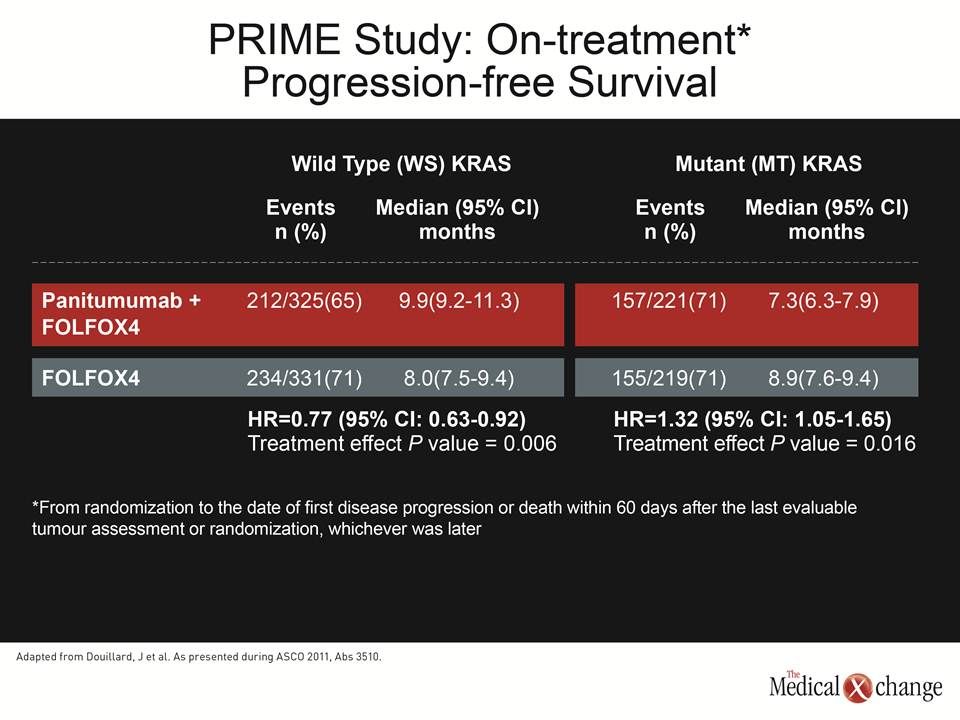
However, these data do not diminish the potential role of mABs for treatment of metastatic colorectal cancer (CRC). In another multicentre phase III study called PRIME, the addition of the mAB panitumumab to FOLFOX4 did yield significant improvements in progression-free survival (PFS) and a trend for improved OS in those patients with the wild type (WT) KRAS mutation. However, FOLFOX4 alone was superior to FOLFOX4 plus panitumumab in patients with mutant (MT) KRAS.
“In this, the final analysis of PRIME, panitumumab plus FOLFOX4, relative to FOLFOX4 alone, produced a statistically significant improvement in PFS, a trend towards improvement in OS, and a statistically significant improvement in response rate in patients with WT KRAS.”
“In this, the final analysis of PRIME, panitumumab plus FOLFOX4, relative to FOLFOX4 alone, produced a statistically significant improvement in PFS, a trend towards improvement in OS, and a statistically significant improvement in response rate in patients with WT KRAS,” reported Dr. Jean-Yves Douillard, Head, Department of Medical Oncology, Centre René Gauducheau, Saint-Herblain, France. In this study, 1,183 patients with previously untreated metastatic CRC and an ECOG performance status of 2 or lower were randomized to FOLFOX4 or FOLFOX4 plus panitumumab. Unlike bevacizumab, which binds to vascular endothelial growth factor (VEGF), panitumumab targets the epidermal growth factor receptor (EGFR). The stratification of patients by WT or MT KRAS for efficacy analysis was preplanned. After up to 44 months of follow-up, the PFS was improved by 20% in the panitumumab plus FOLFOX4 arm alone relative to FOLFOX4 alone in the WT KRAS group (HR 0.80, 95% CI 0. 67 – 0.95; P=0.01). In the MT KRAS group, there was a 27% reduction in PFS on FOLFOX4 with panitumumab relative to FOLFOX4 alone (HR 1.27, 95% CI 1.04 – 1.55; P=0.02). When restricted to the on-treatment period, each difference was slightly greater. Similar trends were observed for OS, but neither the 12% relative improvement (HR 0.88, 95% CI 0.73 – 1.06; P=0.17) or the 17% worsening (HR 1.17, 95% CI 0.95 – 1.45; P=0.15) on the mAB plus chemotherapy versus chemotherapy alone in the WT and MT groups, respectively, were clinically significant. (Table 2) The new phase III data for the treatment of locally advanced rectal cancer employ many of the same agents that have been effective in the colon. In the German CAO/ARO/AIO-04 multicentre study, 637 patients with stage II or III adenocarcinoma of the rectum within 12 cm from the anal verge were randomized to one of two treatment courses. In arm 1, patients received preoperative chemoradiation (CRT), surgery, and then adjuvant 5-fluorouracil (250 mg/m2 on days 1 to 14 and days 22 to 35). In arm 2, patients received CRT with 5-fluorouracil and oxaliplatin (50 mg/m2/days 1, 8, 22, 29), followed by surgery and 8 cycles of adjuvant chemotherapy according to modified FOLFOX6 regimen (2-hour infusion of 100 mg/m2 oxaliplatin and 400 mg/m2 leucovorin on Day 1, followed by 400 mg/m2 bolus on Day 1 followed by a 2.4 g/m2 infusion over 46 hours). Follow-up so far is insufficient to assess the primary endpoint of DFS, but the pathologic complete response (pCR) rates were significantly higher in the arm receiving oxaliplatin (17.6% vs. 13.1%; P=0.033). Importantly, presuming that this regimen does improve outcomes, the addition of oxaliplatin did not increase the rate of adverse events. “Preoperative grade 3 or 4 toxicity occurred in 21.6% in arm 1 and in 22.9% in arm 2, and overall postoperative complications were not different between both arms (21.0% and 21.9%),” reported Dr. Claus Rödel, Department of Radiation Therapy, University of Erlangen, Germany. He called the addition of oxaliplatin well tolerated but acknowledged that full analysis waits longer follow-up. However, there is considerable excitement and optimism about the likelihood of an important step forward in disease control with this protocol, according to the ASCO-invited discussant, Dr. Robert Glynne-Jones, Mount Vernon Cancer Center, Northwood, UK. Calling the study “absolutely fantastic,” he was impressed by the quality assurance for total mesorectal excision (TME) that led to good surgical results in nearly 75% of patients, the “stunning” pathological evaluation of a median 15 lymph nodes in each group, and the 60% completion rate of the preoperative regimen with full doses of radiation, oxaliplatin, and 5-fluorouracil. The only problem is that if this does, as expected, show a favourable impact on DFS, “we are not going to know which component—whether it was the oxaliplatin or the 5-fluorouracil in the preoperative or adjuvant setting—was the most important so you will have to buy into the whole package,” Dr. Glynne-Jones observed.
In combination with GEMOX, “the median PFS was 5.8 months on erlotinib and 4.2 months without, a difference that approached statistical significance [P=0.080].”
Not least important of new data relevant to the GI tract presented at ASCO 2011, another phase III study demonstrated a difference between two palliative chemotherapy regimens employed in patients with unresectable metastatic biliary tract carcinoma. In this study, 268 patients randomized to GEMOX (1,000 mg/m2 of gemcitabine plus 100mg/m2 of oxaliplatin daily for two weeks) or to GEMOX plus 100 mg of erlotinib, a tyrosine kinase inhibitor (TKI). Patients were eligible if they had histologically confirmed unresectable metastatic adenocarcinoma of biliary tract (CCC), ampulla of vater (AOV) or gall bladder (GB) and ECOG performance status of 2 or less. The primary endpoint was PFS. “With a median follow-up of 13.9 months, the median PFS was 5.8 months in the arm that received erlotinib and 4.2 months in the one that did not, a difference that approached but did not reach statistical significance [P=0.080],” reported Dr. Ho Yeong Lim, Division of Hematology-Oncology, Samsung Medical Center, Seoul, South Korea. However, in a subgroup analysis, “the median PFS was significantly longer for the CCC patient who received erlotinib relative to those who did not (5.9 vs. 3.0 months; P=0.049).” He also noted that the objective response rate was higher in those who received erlotinib. Overall, the data from these phase III studies suggests that cytotoxic agents remain the mainstay of treatment for a broad array of GI malignancies whether or not these are being used first-line, in the adjuvant setting, or for palliative treatment in the advanced disease setting. Targeted therapies can but do not necessarily boost response rates, suggesting that their application is more circumscribed and more dependent on the cancer stage.
Conclusion
A series of phase III trials presented at the 2011 ASCO Annual Meeting have contributed new information to state-of-the-art clinical practice in GI oncology both by confirming and refuting study hypotheses. In early stage disease, targeted therapies have not performed well so far. Many of the most commonly used therapies, such as variations on FOLFOX, remain the standard both in early and late stage disease on which new strategies are being built.