HIV
6th IAS Conference on HIV Pathogenesis, Treatment and Prevention (IAS 2011)
NRTIs: Sorting Risk Relationships in Aging HIV Patients
Rome – In most industrialized countries, including Canada, the phenomenon of accelerated aging is now widely considered the most significant issue for prolonging the lifespan of patients with human immunodeficiency virus (HIV). Although the first signal of earlier-than-expected, age-related morbidity and mortality was generated several years ago by a rising rate of cardiovascular events in relatively young HIV patients, it is now clear that age-related diseases are occurring earlier across a spectrum of physiological systems, including the kidneys, the skeleton, and the central nervous system (CNS). At the IAS 2011 meeting, controlling age-related diseases was identified as an urgent clinical need in parts of the world where the median age of HIV patients is rising. Despite evidence that HIV-driven inflammatory processes may be a significant source of accelerated aging, individualizing choice of pharmacologic agents to avoid exacerbating the risk of specific age-related events appears to be a critical part of strategies toward risk reduction.
The concern about accelerating age-related disease processes in patients with human immunodeficiency virus (HIV) is no longer new, but data are maturing, permitting a better quantification of risk, a better understanding of specific risk factors for different types of age-related diseases, and a more detailed understanding of how risk can be minimized. In the past, some of the concern was driven by changes in surrogates rather than actual events, such as loss of bone mineral density (BMD) instead of fracture rates, but as a larger proportion of patients reaches the age when events occur, true risk is being calculated with new accuracy.
“It is now clear that the processes of aging are occurring at a more accelerated rate in patients with HIV, including those with optimally-suppressed viral loads, but we are still learning what strategies to employ toward reducing the risk of events.”
“It is now clear that the processes of aging are occurring at a more accelerated rate in patients with HIV, including those with optimally-suppressed viral loads, but we are still learning what strategies to employ toward reducing the risk of events,” reported Dr. Judith Feinberg, Professor of Medicine, University of Cincinnati College of Medicine, Ohio. Chair of one of several symposia at the IAS 2011 meeting that addressed premature aging, Dr. Feinberg indicated that HIV care is likely to be redefined by the effort to balance relative risks.
Achieving Cardiovascular Risk Reduction
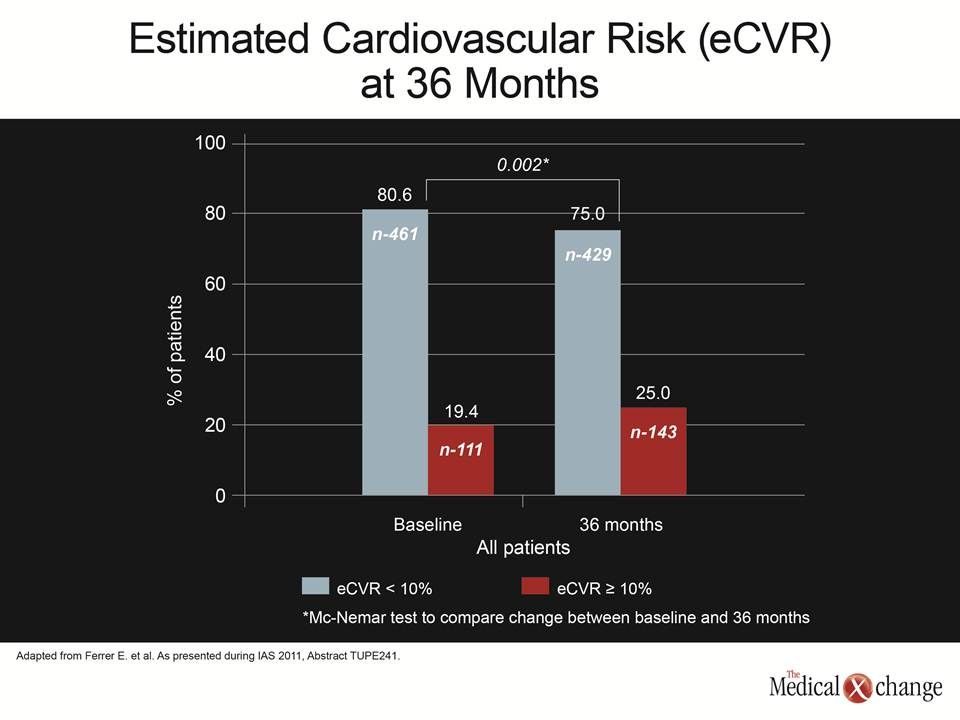
At this year’s IAS, discussion of renal impairment and bone mineral loss were dominant areas of interest. These do not displace the concern about the risk of early cardiovascular (CV) events, but the accumulating evidence suggests that CV risk is readily measured by conventional risk stratification. This particular clinical message was reiterated by a relatively large prospective multicentre cohort study. In data presented by Dr. Elena Ferrer, HIV Unit, Service of Infectious Diseases, Hospital Universitari de Bellvitge, Barcelona, Spain, the proportion of the 572 patients estimated to have a greater than 10% CV risk over the coming 10 years climbed from 19% to 25% (P=0.002) in just three years, but there were no surprises in the type of factors that drove this increase in risk (Fig. 1).
“The rising proportion of patients with moderate to severe risk of a CV event was related to traditional risk factors,” reported Dr. Ferrer, who noted that the average age in the cohort was only 41 years although the range was 22 to 83 years. It is notable that hyperlipidemia became a less prominent source of CV risk over time because of increasing use of statins. There was also some risk reduction achieved with smoking cessation, but these were countered by increasing waist circumference and rising rates of hypertension, which are also common in aging individuals without HIV.
One of the implications of this study is that CV risk management remains largely an issue of lifestyle modifications and, when appropriate, statin use. Specific changes in antiretroviral treatment to manage risk appear less important. Overall, the dyslipidemias associated with some antiretroviral agents, particularly protease inhibitors (PIs), are readily detected and usually treatable with lipid-lowering drugs.
Renal Impairment: Easier to Prevent than Reverse
In contrast, the attention paid to renal impairment, loss of BMD, and cognitive impairment is based on the prospect of modifying antiretroviral treatment to lower risk. In particular, declining renal function, which is also closely associated with increased CV risk, is an insidious process that may be difficult to reverse once it has begun.
Improvements in renal function are achieved by switching from antiretroviral regimens that contain agents associated with nephrotoxicity to those that that do not. The switch only provides a modest reversal of renal function impairment, but it may be very important for preventing further deterioration.
“Clinicians now know that adverse changes in renal function are common in patients with HIV, but it is not clear what steps should be taken when signs of renal dysfunction, such as rising rates of proteinuria or serum creatine are observed,” reported Dr. Lisa Manzini, Department of Biomedical Sciences, University of Modena, Italy. The lead author of a retrospective study of patients who had switched antiretroviral therapies, Dr. Manzini reported that improvements in renal function are achieved by switching from antiretroviral regimens that contain agents associated with nephrotoxicity to those that that do not. The switch only provides a modest reversal of renal function impairment, but it may be very important for preventing further deterioration.
In the study, patients were evaluated who switched from tenofovir (TDF), which is one of the antiretrovirals most closely associated with renal toxicity, to abacavir (ABC), which is also a nucleoside reverse transcriptase inhibitor (NRTI) but does not have a strong association with renal dysfunction. About half of the 83 patients who switched did so because of proteinuria while the other half switched because of rising rates of serum creatinine or hypophosphoremia. Only 22% had hypertension at the time of the switch, about one third had a hepatitis co-infection, and one third had a previous acquiredimmune deficiency syndrome(AIDS) event. Although there was no significant change in serum creatinine or estimated glomerular filtration rate (eGFR) within six months of the switch, there was a highly significant reduction in proteinuria (P<0.001).
“Some of the switches were made on the basis of very early signs of renal toxicity, which demonstrates the concern about TDF,” Dr. Manzini reported. Although she reported that there is no guideline and little data to support an improvement in outcome with a switch at the earliest signs of renal dysfunction, “proteinuria improved significantly even in this short time of observation and among patients who were not very compromised.”
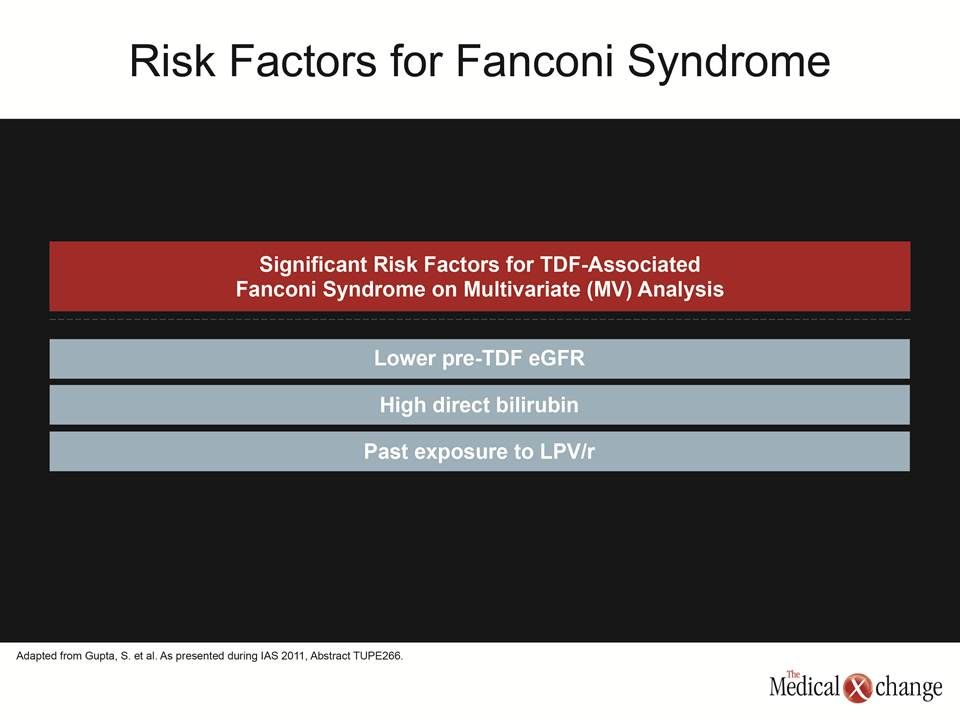
Only a minority of patients treated with TDF develops nephrotoxicity in long-term follow-up, but the problem has been in identifying those who are at risk, particularly if renal impairment is irreversible. In another study that attempted to identify risk factors for Fanconi syndrome in patients taking TDF, a low eGFR prior to starting TDF and past exposure to ritonavir-boosted lopinavir (LPV/r) were risk factors along with a high baseline direct bilirubin. However, discontinuation of TDF after the development of Fanconi syndrome (extra slide 1) did not necessarily provide a resolution of the disease state.
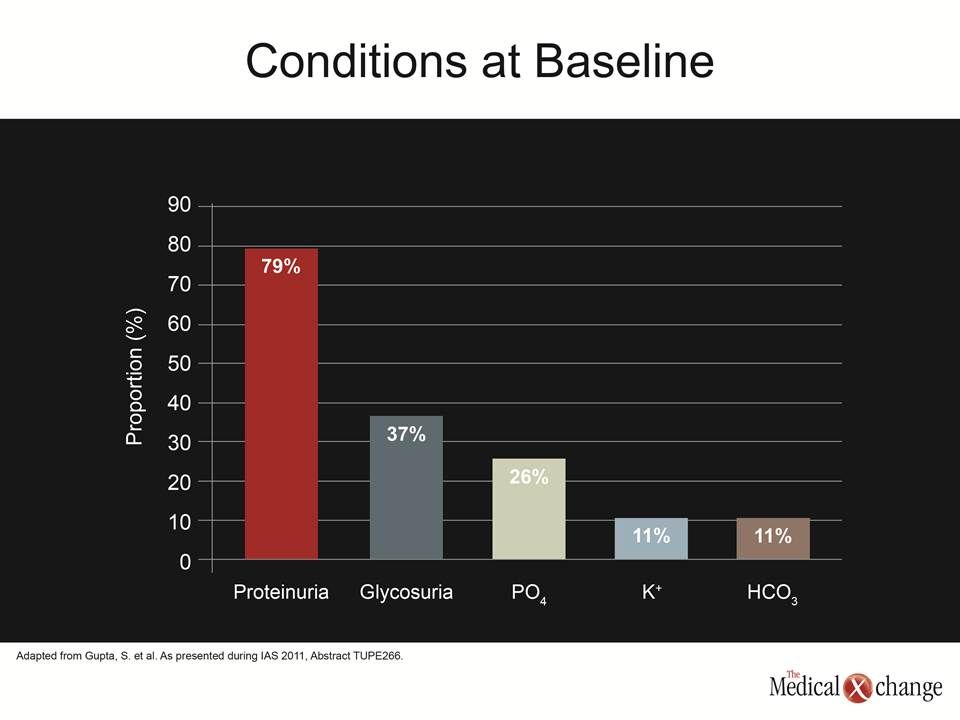
“After 48 weeks of follow-up, proteinuria resolved in nearly 60% of cases, but eGFR had returned within the normal range in fewer than half the patients after this length of time,” reported Dr. Samir K. Gupta, Division of Infectious Diseases, Indiana University School of Medicine, Indianapolis. In presenting these data, which were based on 19 Fanconi syndrome patients and 37 controls collected at nine participating centres, Dr. Gupta emphasized the variability in the presentation. Although a low eGFR (median level of 41 mL/min/1.73 m2) was characteristic, only 79% had proteinuria, 37% had glycosuria, and 11% had hyperkalemia (Fig. 2).
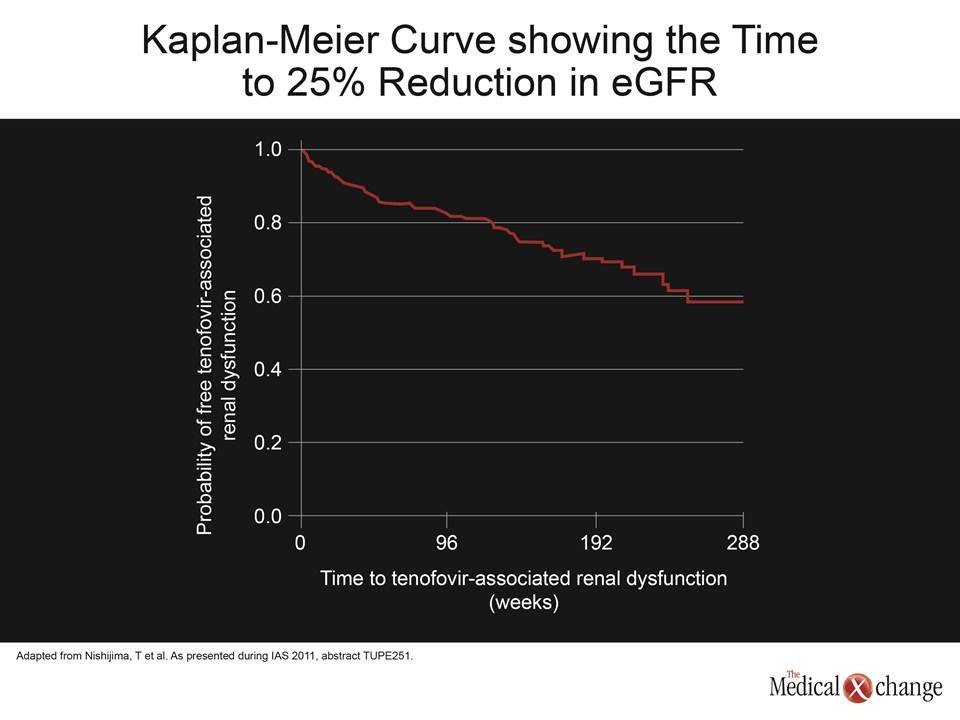
One risk factor for nephrotoxicity from antiretroviral agents may be a low body weight, judging from a single-centre cohort following TDF-related renal impairment in Japan. In this population of 495 patients, the incidence of TDF-associated renal dysfunction was 19.6%, but the authors found a significant association with weight and body mass index (BMI). While the median body weight in this population was only 61 kg, the hazard ratio (HR) of renal dysfunction increased 23% (HR 1.23, 95% CI 1.10 – 1.37; P<0.001) for each 5 kg reduction. A similar risk was observed with decreasing BMI. Other risk factors on multivariate analysis included higher baseline eGFR, lower baseline serum creatinine, older age, smoking, hepatitis C co-infection, and use of another nephrotoxic agent.
“TDF-associated renal dysfunction has not been well studied in relationship to body weight. Our results suggest that this is an important factor and may explain the relatively high rates of this complication in Japan,” reported Dr. Takeshi Nishijima, AIDS Clinical Center, National Center for Global Health and Medicine, Tokyo, Japan. “This may be an important issue in other populations with low body weight.” (extra slide 2)
Osteoporotic Fracture: Event Comparison
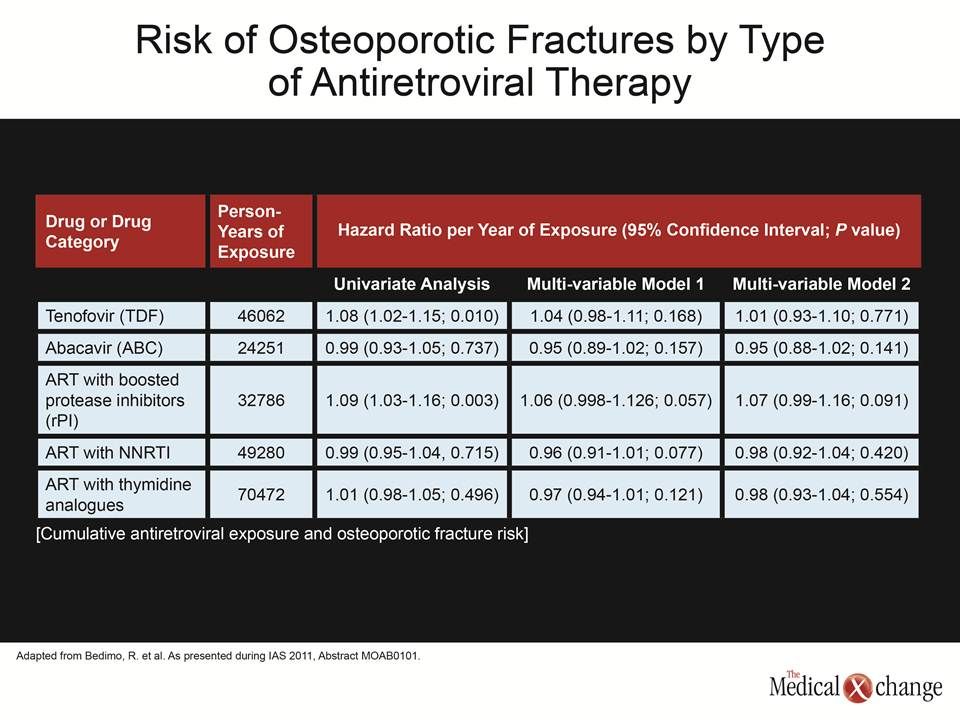
In the series of studies looking at age-related conditions at the IAS meeting, one of the most noteworthy looked at osteoporotic fracture rates in the context of antiretroviral therapies. This is one of the first large studies to look at events rather than the surrogate of BMD. The study found higher fracture rates in patients exposed to ritonavir-boosted PIs relative to non-nucleoside reverse transcriptase inhibitors (NNRTIs) and in patients exposed to TDF relative to ABC. This increase was modest and lost significance in a multivariate analysis that controlled for confounding variables, such as age, BMI, gender, and presence of other potentially nephrotoxic drugs, but the study is important because it was able to generate event data even though the average age of the population was only 45 years.
“On univariate analysis, the risk of an osteoporotic fracture was about 10% higher on TDF relative to ABC, but other factors, such as tobacco use and a BMI <20, were stronger predictors and the increased hazard ratio was no longer significant after we controlled for these variables,” reported Dr. Roger Bedimo, VA North Texas Health Care System, Dallas. He reported that there was a similar relative increase with combination therapy that featured a boosted PI relative to a NRTI, but this also fell below significance when controlling for traditional risk factors (Table 1).
The loss of significance when controlling for other risk factors does not exonerate TDF from risk, because longer term follow-up in an older age group may be needed to confirm an effect over time, but the important aspect of this study was the event-based design. Much of the data pointing to an early onset of age-related diseases in HIV-infected individuals, including numerous studies at the IAS meeting, have been based on surrogate measures, which may not be representative of actual risk of events or provide value for evaluating how different strategies mediate changes on hard outcomes, particularly measurable morbidity and mortality.
Cognitive Dysfunction: Looking for Clinical Significance
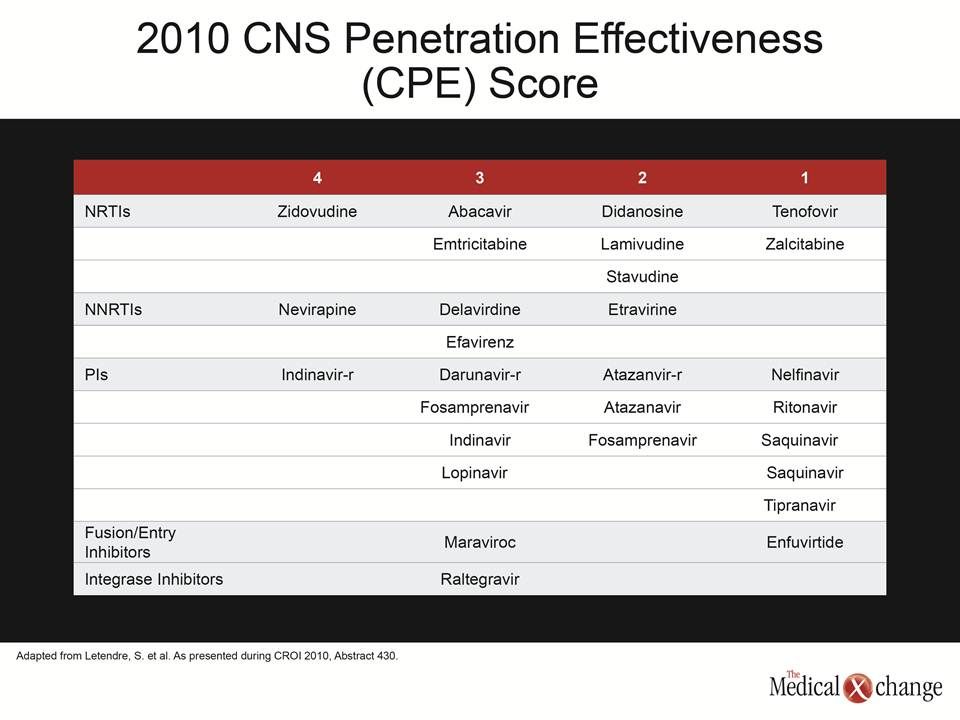
One potential example of the importance of conducting endpoint studies is the difficulty encountered so far in associating antiretroviral therapies that offer good central nervous system (CNS) penetration with a clinically meaningful reduction in risk of cognitive decline. In data from the Ontario HIV Treatment Network (OHTN) presented at the IAS, a comparison of neuropsychological performance in 255 patients who had serial testing was unable to find any association between an antiretroviral regimen with good CNS penetration effectiveness (CPE) and neurocognitive outcomes.
“We need to expand the number of factors we consider to include variables such as timing issues, duration of HIV infection, and duration of antiretroviral therapy.”
Again, this does not suggest that CPE, which is a formal system for rating the anticipated HIV control of a given antiretroviral agent in the CNS compartment, is not important, but it does suggest that the effort to identify better regimens may require more than just calculating the CPE value. According to Sean B. Rourke, who presented the data on behalf of OHTN, “we need to expand the number of factors we consider to include variables such as timing issues, duration of HIV infection, and duration of antiretroviral therapy.” The fact that higher CPE scores did not lead to a reduction in cognitive decline emphasizes the importance of altering therapy based on evidence of benefit rather than on hypotheses that might be too simplistic to account for the broad array of variables that influence clinical outcomes (Table 2).
Conclusion
There is now extensive and compelling evidence that age-related diseases occur earlier in individuals who are HIV positive. Stress across multiple systems mediated by chronic inflammation due to the HIV infection is strongly suspected of being an important factor, but it is likely that there are multiple contributing influences, including lifestyle choices and antiretroviral therapies. Many of the questions regarding age-related diseases will be answered by data accumulating in countries such as Canada with an increasing proportion of HIV infected patients reaching middle age and beyond. As events occur, there will be a major opportunity to conduct outcome-oriented studies that will yield evidence-based standards of optimal care.