cardiology
2011 Canadian Hypertension Congress
Simplified Dosing with Single-pill Combinations: Focus on Blood Pressure Goals
Alliston – More than two thirds of patients with hypertension require two or more antihypertensive agents to achieve blood pressure (BP) goals. Combination therapy is so fundamental to effective BP control that the most recent Joint National Committee guidelines (JNC 7) recommend considering combination therapy as an initial strategy when BP is >20/10 mmHg above goal. To reduce complexity, there are now a variety of single-pill combinations, often suitable for once-daily dosing, to allow goals to be achieved and sustained with minimal demands of the patient and physician. While many of these combinations include a renin-angiotensin system (RAS) inhibitor because of favourable effects on multiple organ systems beyond the vasculature, including renal function and anti-hypertrophic effects on cardiac tissue, the key question has been which RAS inhibitor to use combined with which second agent.
Combination therapy is now the rule rather than the exception in the management of hypertension. The combination of two different mechanisms of action not only increases the likelihood of reaching targets, but “duration of control may be extended, with control throughout the day, and nighttime control, and morning surge in particular may be better controlled, and we know this is an important aspect leading to events,” noted Dr. Ernesto L. Schiffrin, Canada Research Chair in Hypertension and Vascular Research, Lady Davis Institute for Medical Research, and Professor, Department of Medicine, McGill University, Montreal, Quebec.
A single pill antihypertensive combination has obvious advantages. For the patient, a single pill reduces the complexity of treatment and is likely to improve adherence, according to Dr. Schiffrin, who observed “the fewer pills the better, and the less chance for patients to forget to take them.” He suggested that combination agents also reduce the “therapeutic turbulence” of starting and stopping multiple agents during complicated efforts to titrate more than one agent. For the physician, combination pills, which often employ relatively low doses of two effective drugs, are typically well tolerated while reducing the inherent complexity when two drugs are being titrated simultaneously.
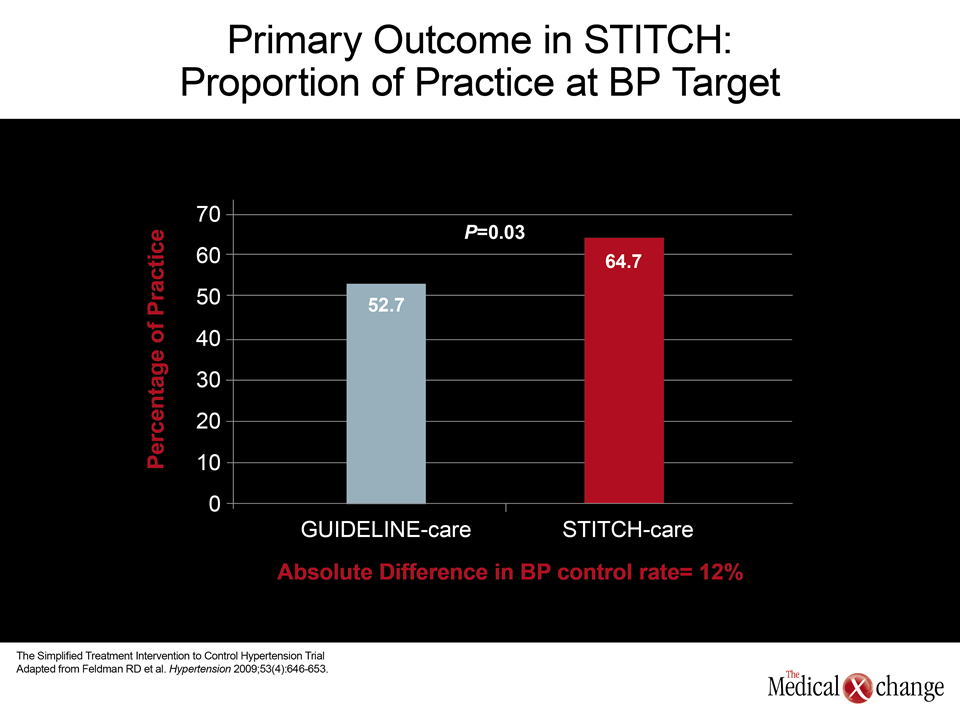
Of the studies demonstrating the benefit of combination therapy, the Simplified Treatment Intervention to Control Hypertension (STITCH) trial was cited by several experts, including Dr. Schiffrin, as being particularly persuasive. Conducted in Canada, the proportion of patients achieving target blood pressures (BP) was compared in family practices that used either a simplified algorithm with a fixed-dose combination or a guidelines-based titration scheme. The single-pill combination approach provided a 12% absolute increase in the proportion of patients at goal (64.7% versus 52.7%; P=0.03).
“Overall, when you use a single-pill combination rather than an individual drug, there’s a better antihypertensive benefit to adverse effect ratio, and potentially improved effects”, noted STITCH lead author, Dr. Ross Feldman, Robarts Research Institute, London, Ontario.
Weighing Available Combination Therapies
There are many potent fixed-dose, single-pill combinations. The majority of these include a renin-angiotensin system (RAS) inhibitor with another agent, typically a diuretic, but there are others, such as fixed-dose combinations with a RAS inhibitor and a calcium channel blocker (CCB). While there may be situations in which adding a CCB is attractive, such as in those individuals with angina or increased heart rate, the combination of a RAS inhibitor with a low-dose diuretic is among the most commonly employed single-pill dual therapies because they pose a low risk of hypotension, are generally well tolerated, provide complementary effects on BP control, and may have benefits on other organs adversely affected by elevated angiotensin. While both angiotensin receptor blockers (ARBs) and angiotensin-converting enzyme (ACE) inhibitors are options, ARBs are generally better tolerated.
Even when the choice is made to employ a single-pill combination of an ARB and a diuretic, there appear to be differences in currently available options.
However, even when the choice is made to employ a single-pill combination of an ARB and a diuretic, there appear to be differences in currently available options. Of ARBs, there have been long debates about the general efficacy of agents that differ substantially in pharmacokinetic (PK) features such as half-life and volume of distribution. While there has been a widespread perception that olmesartan, which has the longest half-life may be the most potent ARB, Dr. Schiffrin discussed recent data with the “new kid on the block” – azilsartan medoxomil (AZL-M). Like olmesartan, AZL-M has a half-life of approximately 12 hours, but it has a greater bioavailability (60% vs. 30%). Perhaps more importantly, it has a relatively strong affinity for and slow dissociation from the angiotensin II type 1 (AT-1) receptor, which is the key mediator of benefit from ARBs.
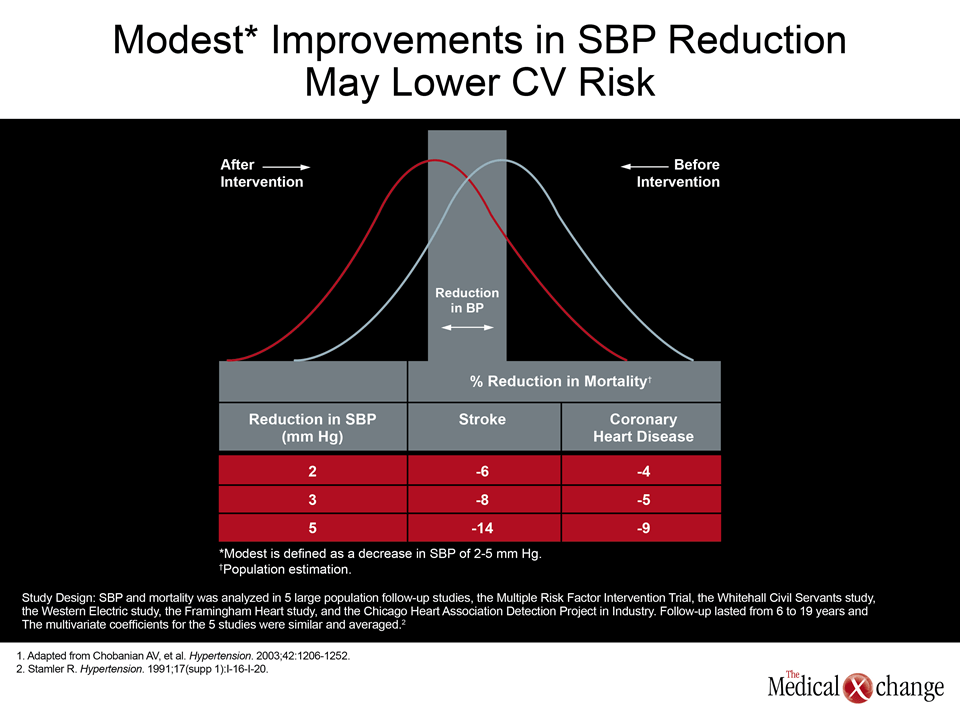
Lowering Systolic Blood Pressure to Reduce CV Events and CV-related Mortality
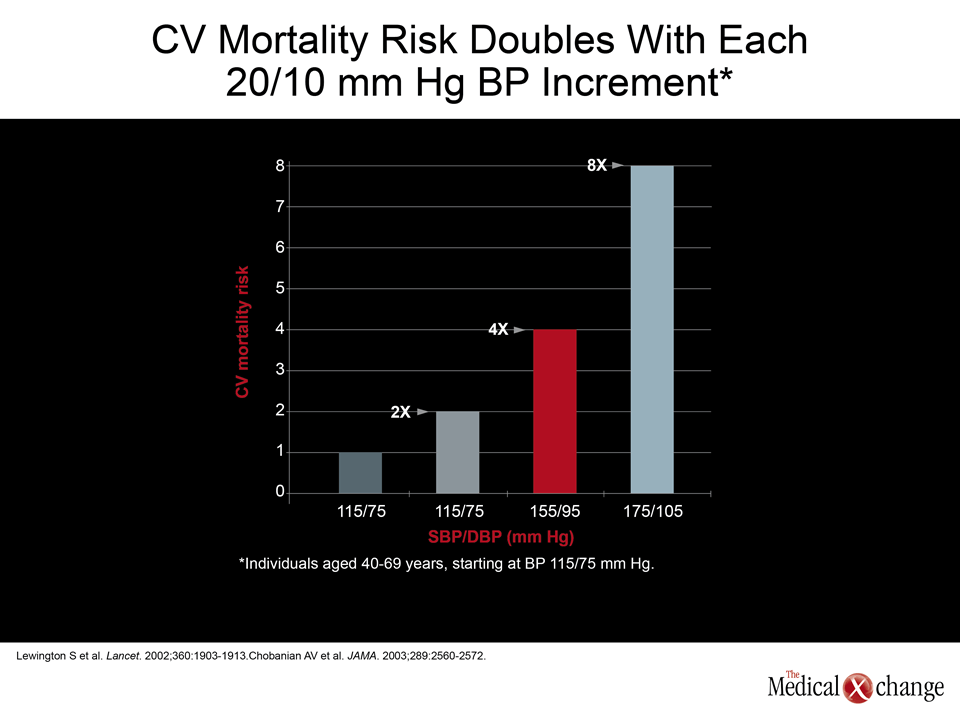
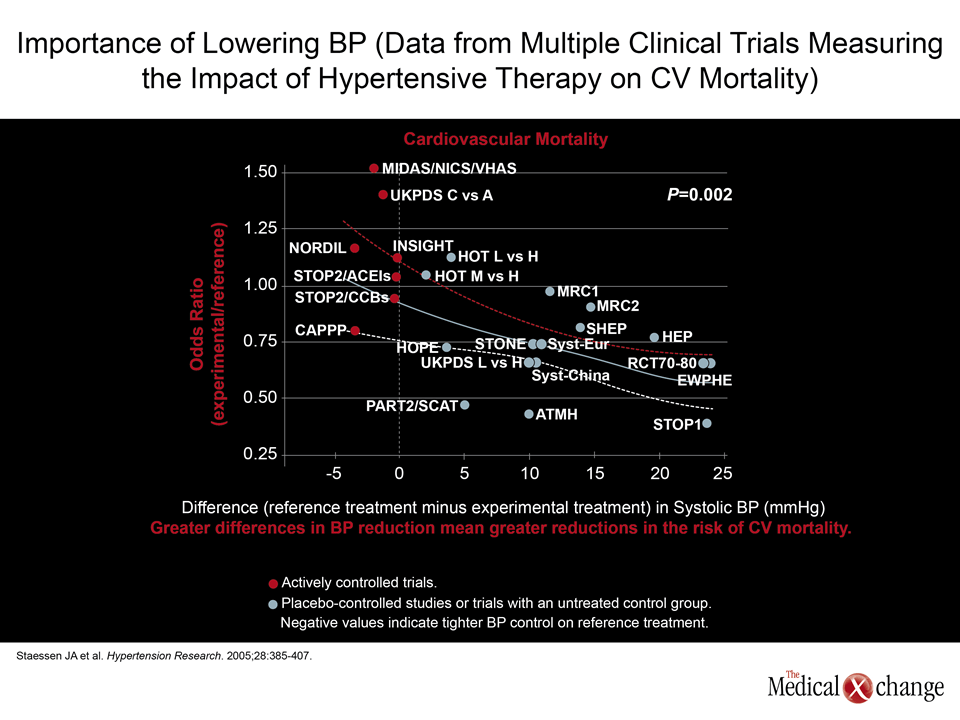
Numerous studies demonstrate a positive correlation between increasing SBP and increasing risk of CV events as well as CV-related mortality.
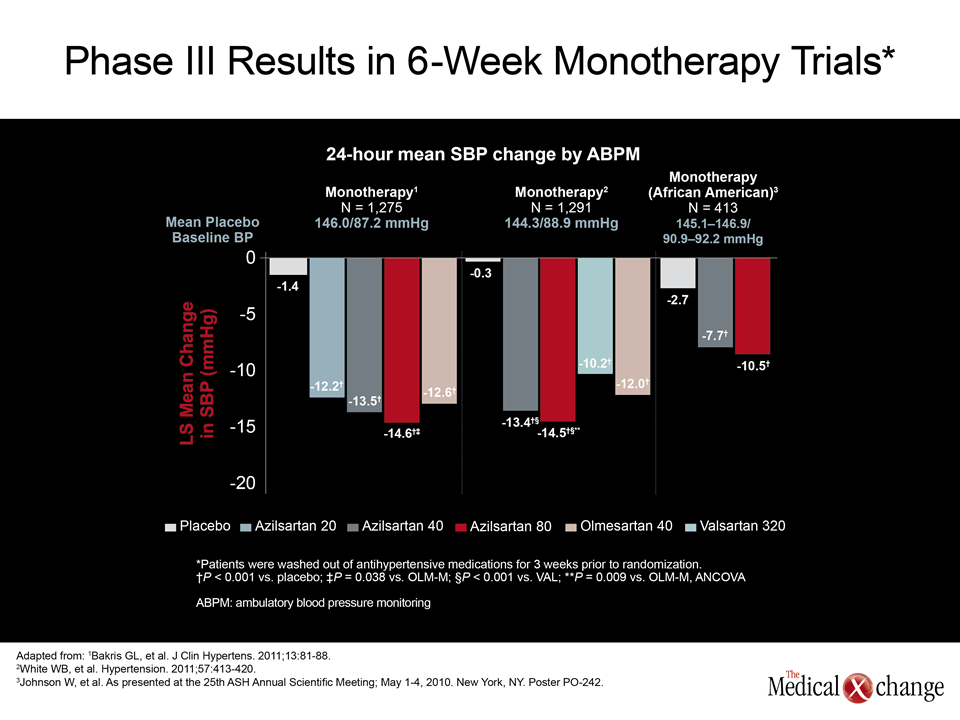
In phase III monotherapy comparisons between ARBs, the 80 mg dose of AZL-M was more effective in lowering systolic BP (SBP) than the highest marketed dose of valsartan (320 mg) or olmesartan (40 mg) (White WB et al. Hypertension 2011;57(3):413-20). Specifically, the mean reduction at the end of six weeks was 14.6 mmHg for AZL-M versus 10.2 mmHg for valsartan and 12.0 mmHg for olmesartan. No outcome data comparing these agents is available, but there are numerous studies demonstrating a positive correlation between increasing SBP and increasing risk of CV events as well as CV-related mortality (Fig. 1).
Diuretics are not all Equal
Similarly, diuretics also do not appear to be interchangeable. While many physicians appear to consider thiazide and thiazide-like diuretics to be similar, Dr. Phil McFarlane, St. Michael’s Hospital, Toronto, Ontario, cautioned that “true” thiazides are chemically different from the “thiazide-like” drugs. Moreover, all these agents are fairly short-acting, with the exception of chlorthalidone (CLD) which has a long half-life. According to Dr. McFarlane, and further supported by Dr. Schiffrin, CLD is making a comeback in hypertension circles. With 40 years of research success behind it, this diuretic has been less popular among doctors of late than hydrochlorothiazide (HCTZ), even though it is more effective in preventing events, reported Dr. Schiffrin. “We’re in this situation where the most potent diuretic has been sort of left behind. But not anymore; there has been a sort of rebirth.”
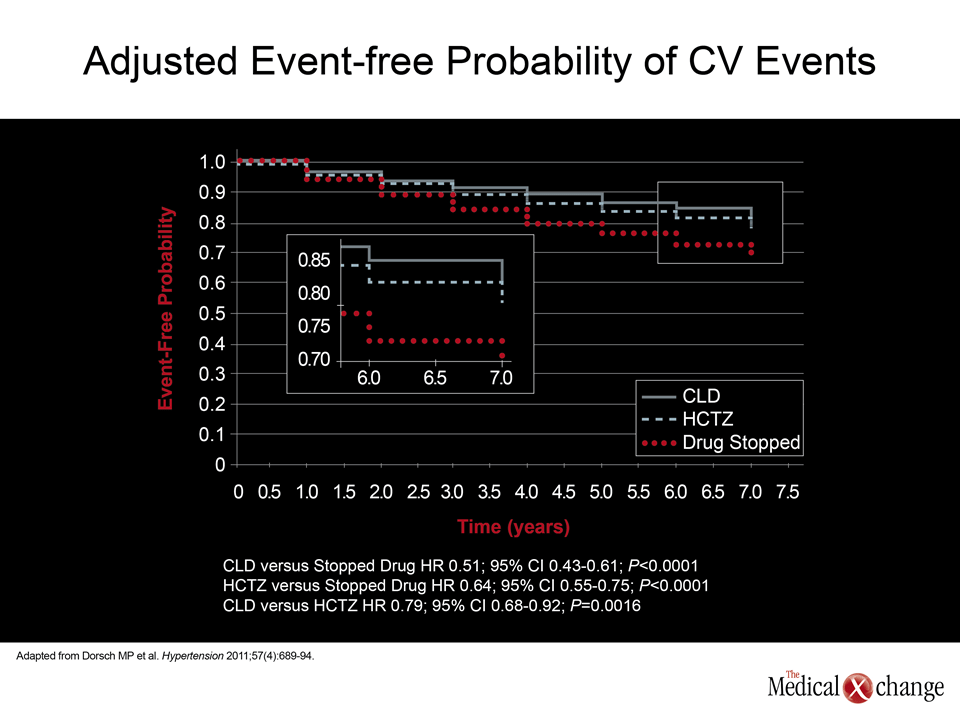
In, a new analysis of the Multiple Risk Factor Intervention Trial (MRFIT), CLD was associated with a highly significant 21% reduction (P=0.0016) in CV events compared with those taking HCTZ (Dorsch MP et al. Hypertension 2011;57(4):689-94) (Fig. 2). Although potassium levels were lower and uric acid levels were higher in those taking HCTZ related to CLD, patients taking CLD had lower BP, as well as lower total and low-density lipoprotein cholesterol.
Combination Therapies Focus on BP Targets
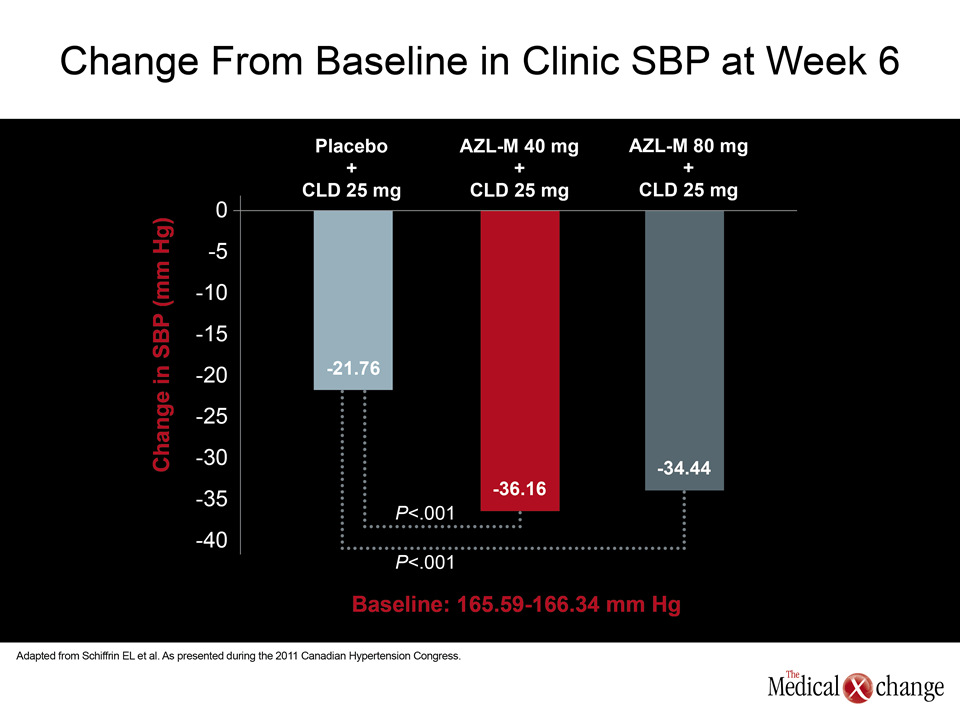
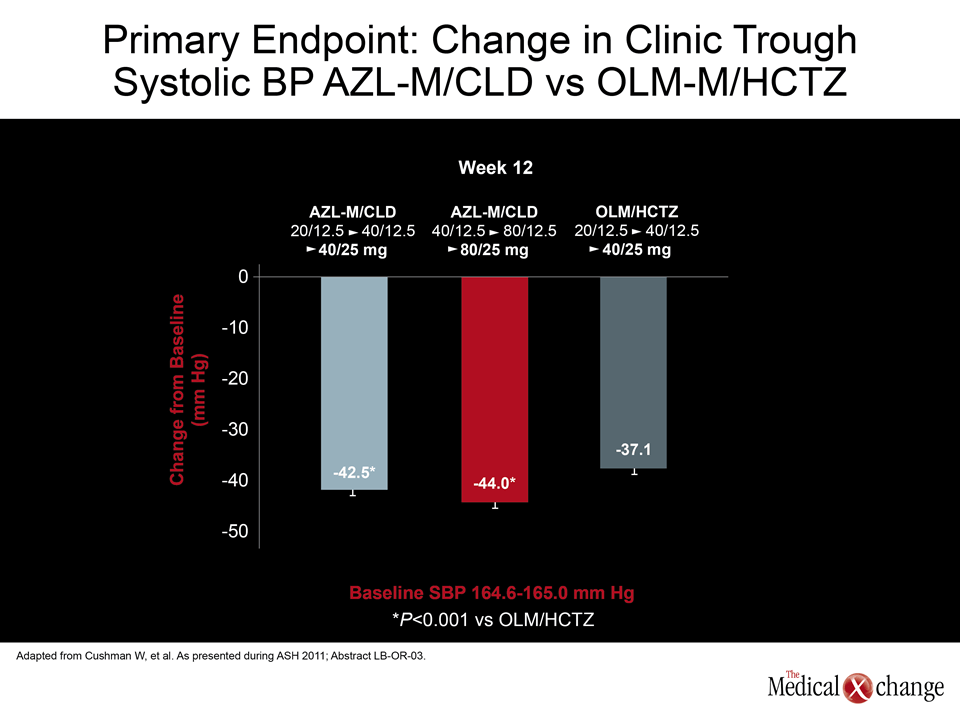
Given the advantages of AZL-M for BP control relative to other ARBs and the greater CV protection associated with CLD relative to HCTZ in the MRFIT trial, it is logical that these agents would be attractive in a fixed-dose, single-pill combination. Indeed, a forced-titration trial comparing a fixed dose combination of AZL-M (20 or 40 mg) in combination with 12.5 mg of CLD to 20 mg olmesartan with 12.5 mg of HCTZ associated both doses of AZL-M with significantly greater reductions in SBP (-6.4 and -8.8 mmHg, respectively; P<0.001). Emphasizing the additive benefits of AZL-M and CLD, Dr. Schiffrin, who characterized the AZL-M/CLD fixed-dose combination as “unique,” noted that a moderate AZL-M dose of 40 mg almost doubled the median reduction in SBP compared to CLD alone (-36.16 vs. 21.76 mmHg). In the absence of outcome data to demonstrate a relative advantage of any single-pill combination over another, Dr. Schiffrin indicated that this is a reasonable first-line approach in individuals who require more than one agent to achieve BP targets.
Conclusion
Combination therapy is now the rule rather than the exception in effective BP control. While multiple pills pose a risk of complicated dosing schemes, highly effective single-pill combinations are associated with simplified dosing, effective BP control, and a high degree of tolerability. For optimal risk reduction, the specific drugs in the single-pill combinations are likely to be relevant not only for optimal BP control but tolerability as well as prevention of end organ events. This explains the interest in combining ARBs and diuretics to increase the proportion of patients who reach treatment targets.
Additional Slides
Figures 3 (Fig. 3), 4 (Fig. 4), 5 (Fig. 5), 6 (Fig. 6), 7 (Fig. 7) and 8 (Fig. 8).