HIV
13th European AIDS Clinical Society (EACS) Conference
NRTI Selection when Avoiding Non-Infectious Co-Morbidities of HIV
Belgrade – Typical of recent scientific conferences on human immunodeficiency virus (HIV), non-infectious co-morbidities of HIV, particularly age-related processes, consumed much of the focus at this year’s EACS conference. New EACS guidelines distributed at the meeting (also available at www.europeanaidsclinicalsociety.org) include substantial attention to these topics, including bone mineral density loss, kidney disease, and cardiovascular risk. Selection of nucleoside reverse transcriptase inhibitor (NRTI) backbones, like the selection of drugs from other classes used in HIV control, is being increasingly based on risk of non-infectious complications relative to the specific risk profile of the patient. This was reflected throughout the EACS conference but was most vividly highlighted in a debate in which three case studies, representing different sets of risks for non-infectious co-morbidities, provided a forum to identify the issues most important for drug selection.
Antiretroviral Therapies and Disease Risk
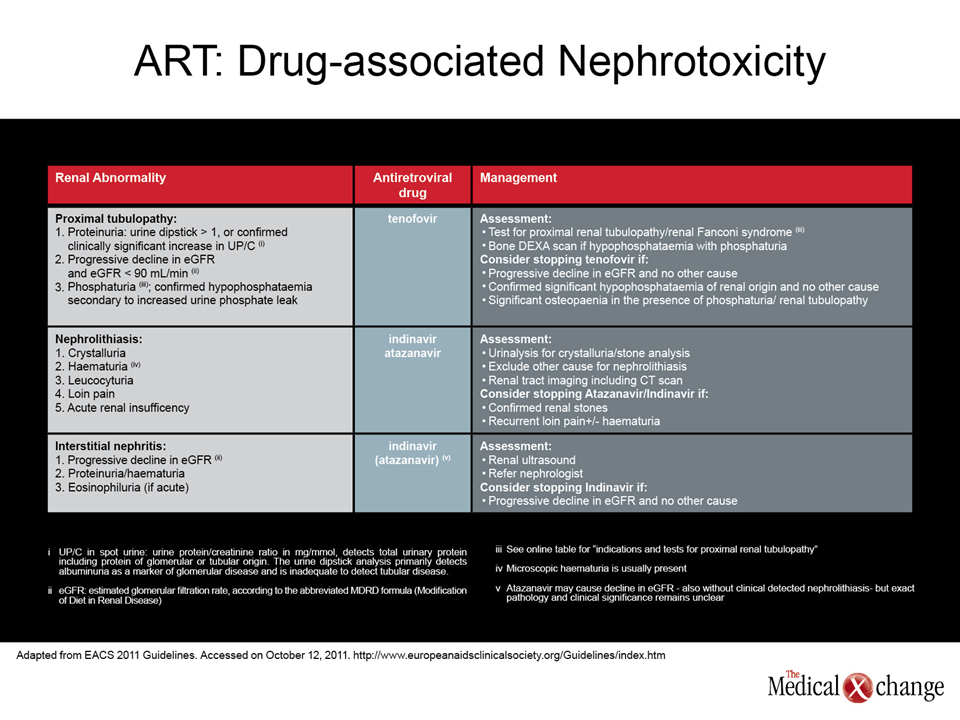
According to the recently released EACS guidelines, non-infectious co-morbidities, which include cardiovascular (CV), renal, hepatic, metabolic, neoplastic, central nervous system, and bone pathologies, are increasingly important in human immunodeficiency virus (HIV) management “as a consequence of increased life expectancy resulting from effective antiretroviral therapy.” While it is the antiretroviral therapies that are permitting patients to survive to an age where the risks of diseases in these organs increase markedly, there is also concern that antiretroviral therapies can exacerbate or, at least, fail to attenuate some of these risks. This has provided a major reorientation in drug selection for nucleoside reverse transcriptase inhibitors (NRTIs) as well as other antiretrovirals.
NRTI backbones have different strengths and weaknesses in regard to risk of co-morbidities.
“We can be confident that both [NRTI] backbones are effective, so efficacy is not the issue. We must cope with the co-morbidities,” reported Dr. Paolo Maggi, Professor of Infectious Disease, University of Bari, Italy. By both NRTI combinations, Dr. Maggi, who participated in one of the three debates regarding NRTI selection in specific cases, was referring to abacavir (ABC) plus lamivudine (3TC) and to tenofovir (TDF) plus emtricitabine (FTC). By far the most commonly used NRTI backbones, ABC/3TC and TDF/FTC have different strengths and weaknesses, particularly in regard to risk of co-morbidities.
Case Study 1: Type 2 Diabetes Mellitus & High Blood Pressure
In the particular debate in which Dr. Maggi participated, the case study was of a patient with type 2 diabetes mellitus and high blood pressure. These co-morbidities increase CV risk as well as risk of renal impairment. His opponent in the debate, Dr. Stefan Mauss, Center for HIV and Hepatogastroenterology, Duesseldorf, Germany, advocated use of TDF/FTC over ABC/3TC, citing data that ABC increases CV risk. In a diabetic, CV risk is even more important than renal toxicity according to Dr. Mauss. While he acknowledged that TDF increases risk of renal toxicity, “this can be monitored easily.”
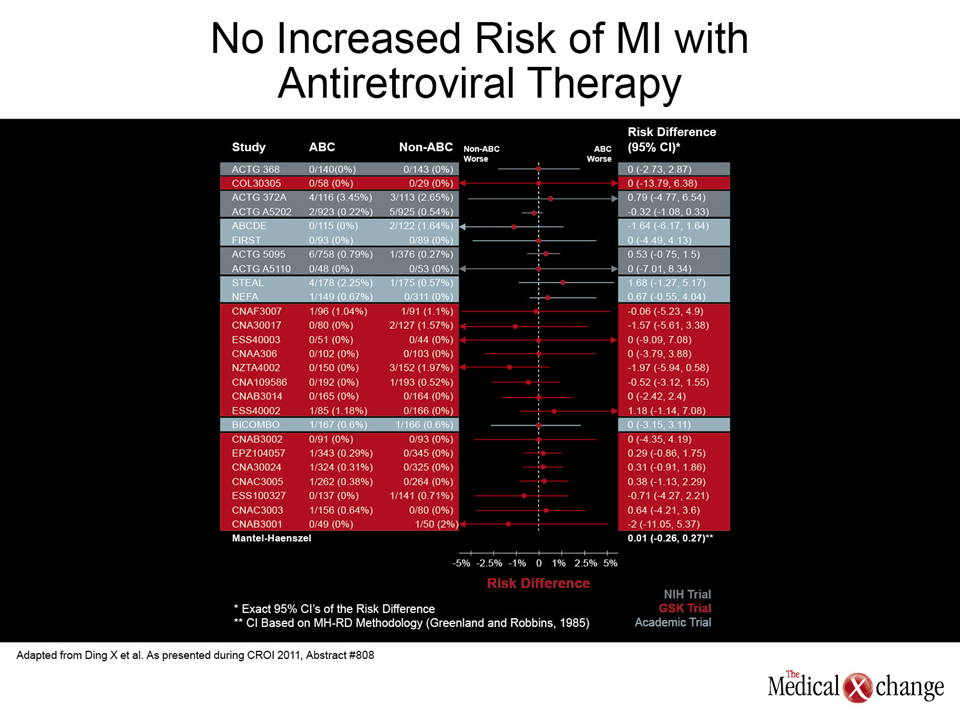
The premise that ABC may increase CV risk was introduced by data from the D:A:D cohort (D:A:D Study Group, Lancet 2008;371:1417-26). While several subsequent studies designed to test this association have also associated ABC with an increased CV risk, many have not. According to Dr. Maggi, who reviewed these data, the most recent analysis from the U.S. Food and Drug Administration is perhaps the most authoritative. Presented at the 2011 Conference on Antiretroviruses and Opportunistic Infections (CROI) (Ding X, et al. Abstract 808) the FDA found no association in an extensive analysis of the available data. Moreover, Dr. Maggi pointed out that there is as yet no plausible mechanism to explain a link between ABC and increased CV risk.
Case Study 2: High Viral Counts and Effective Treatment Options
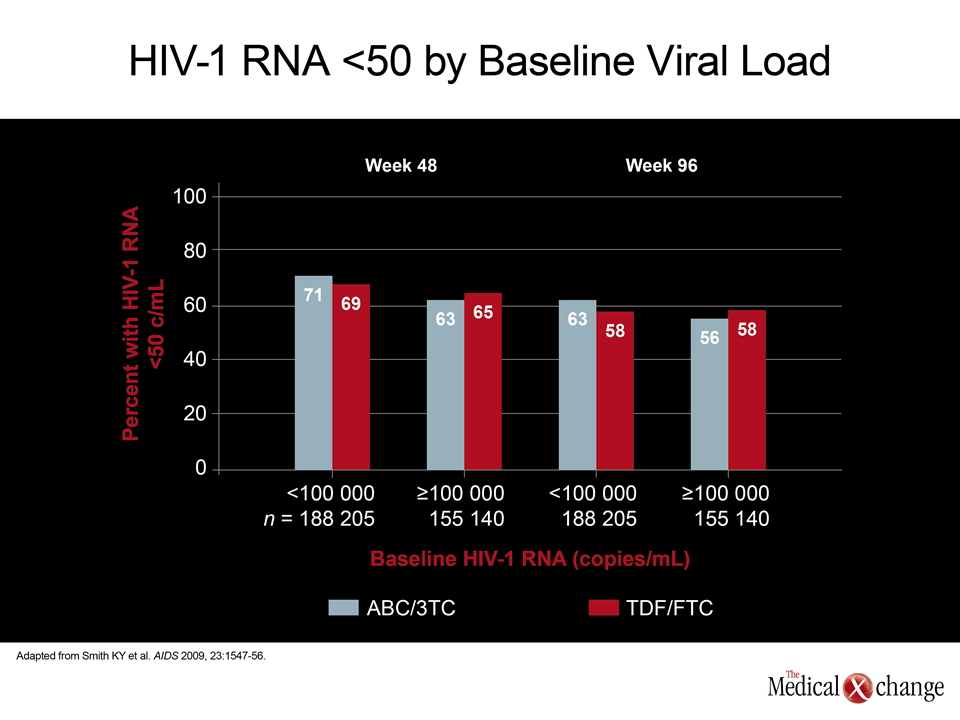
In this first case, both sides accepted the premise that relative efficacy of NRTI backbones are similar, but a potential for a difference in the relative efficacy of the NRTI pairs was the focus of a second case study which involved a treatment-naive patient of Black race with a baseline viral load of >150,000 HIV RNA copies/mL. Dr. Daniel Podzamczer, Coordinator of the AIDS Unit, Hospital Universitario de Bellvitge, Barcelona, Spain, maintained that high viral counts favour TDF/FTC. He cited the ACTG 5202 study (Sax PE, et al. N Engl J Med 2009;361:2230-40), which found ABC/FTC inferior in patients with high viral loads.
His opponent Dr. Alain Lafeuillade, Chief, Department of Infectious Diseases, General Hospital, Toulon, France, noted that the inferiority of ABC/3TC in the ACTG 5202 trial was based on highly atypical endpoints. One definition of failure was any episode of viremia ≥1000 HIV RNA copies/mL during the first 16 to 24 weeks of the study.
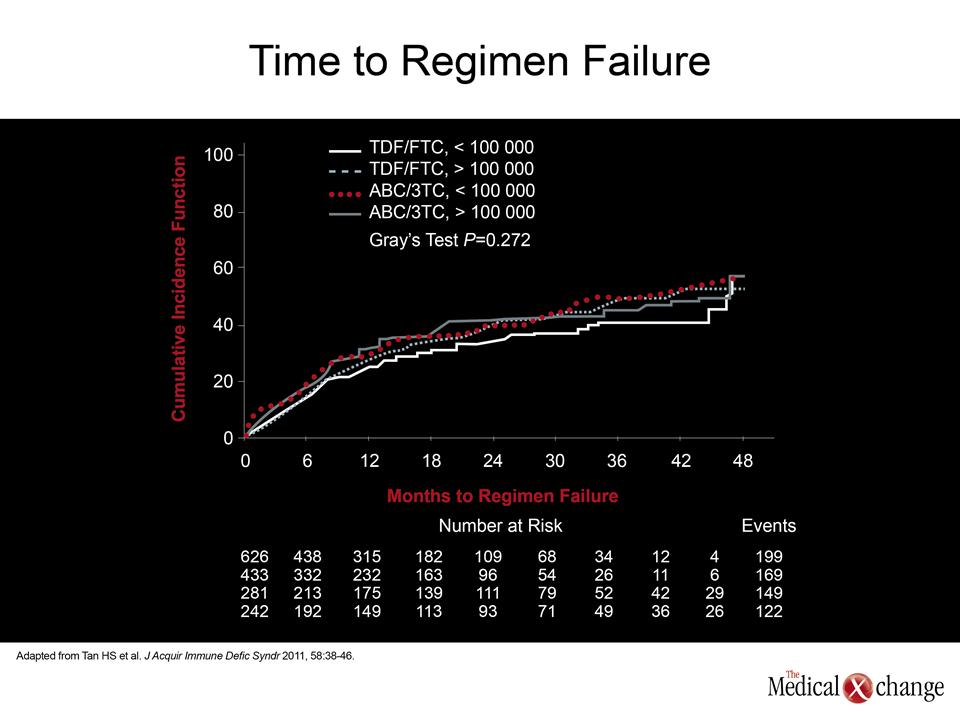
“The accepted endpoint is the proportion of patients with viremia level below 50 HIV RNA copies/mL, and on this endpoint there was no difference between the NRTI combinations in the ACTG 5202 trial,” Dr. Lafeuillade reported. In addition, he suggested that this study should not be cited out of context with the larger body of evidence, including the multicentre HEAT study (Smith KY, et al. AIDS 2009;23:1547-56) (Fig. 1) and the Canadian CANOC study (Tan HS, et al. J Acquir Immune Defic Syndr 2011;58:38-46) (Fig. 2) that found ABC/3TC just as effective in patients with high viral loads. In this Black patient, Dr. Lafeuillade supported ABC/3TC as a more reasonable first choice because of the increased risk of renal toxicity in this racial group.
Case Study 3: Effect on Patient with Osteoporosis
In comparing the relative merits of ABC/3TC and TDF/FTC in a third case, a 50-year-old postmenopausal woman with several risk factors for osteoporosis, including a low body weight, Dr. Pablo Tebas, Director, Adult AIDS Clinical Trials Unit, University of Pennsylvania, Philadelphia, emphasized that bone mineral density (BMD) loss is an important emerging issue because HIV is, by itself, a risk factor for osteoporosis. He supported the use of ABC/3TC over TDF/FTC in this patient because of evidence that TDF accelerates bone loss.
“We have two pairs of NRTIs that can be used in many circumstances, and the truth is we can choose either of them in the vast majority of patients.”
From his perspective, Dr. Manuel Battegay, Chief, Division of Infectious Diseases, University Hospital, Basel, Switzerland, was not convinced that TDF increases risk relative to clinically significant osteoporosis. In particular, he emphasized that no controlled evidence associates TDF with increased fracture risk. Although TDF would not be expected to have any advantage over ABC for attenuating risk for osteoporosis, he prefers this agent for other considerations, such as the efficiency of once-daily regimens when it is combined with efavirenz (EFV).
The moderator of the session, Dr. Santiago Moreno, Professor of Infectious Diseases, Hospital Ramon y Cajal, Madrid, Spain, indicated that there were no winners in these debates. Rather, “we have two pairs of NRTIs that can be used in many circumstances, and the truth is we can choose either of them in the vast majority of patients.”
Conclusion
The extensive attention devoted to non-infectious complications of HIV in the new EACS guidelines underscore the importance these risks have assumed in HIV management. In many centers, including an increasing number in Canada, the average age of patients with HIV is climbing above 50 years. The new EACS guidelines caution that this is an evolving area with specific recommendations regarding use of antiretrovirals likely to change with additional studies.