gastroenterology
American College of Gastroenterology (ACG) 2011
Preventing Relapses of Inflammatory Bowel Disease Often More Convenience-Dependent than Efficacy-Dependent
Washington, DC – In patients taking oral medications for inflammatory bowel disease (IBD), non-adherence has been remarkably high when considering the serious risks of a significant flare. For the clinician attempting to protect patients from the complications of IBD, strategies to maximize adherence are essential. It is perhaps ironic that adherence is a smaller issue in patients who require scheduled infusions of a biologic after failing to adhere to oral agents and thus advancing to more severe disease involvement. Studies evaluating adherence strategies typically focus on mesalamine, the first-line therapy for IBD which provides the most favorable ratio of benefit-to-risk. Efficacy rates for acute and maintenance therapy with mesalamine are high with the most potent once-daily formulations, but recognizing the obstacles to adherence will largely define treatment success.
Non-adherence in Maintenance Therapy
A variety of factors conspire to make non-adherence to prescribed medications uncommonly high in inflammatory bowel disease (IBD). Of these, the intermittent periods of quiescence may be one of the most important. The absence of symptoms can make adherence seem less urgent or even create doubts that a medication is still needed. Yet, maintenance therapy after healing is essential for preventing recurrent flares in both Crohn’s disease (CD) and ulcerative colitis (UC). In patients who are candidates for mesalamine, once-daily treatment with a potent delayed-release formulation can keep up to 90% in long-term remission.
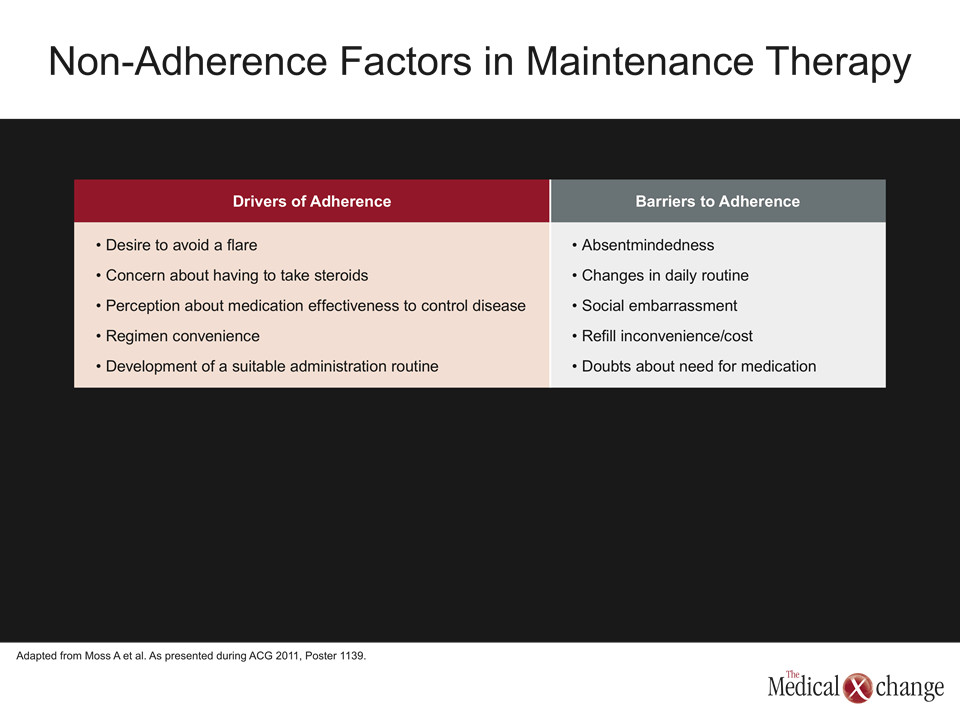
“Non-adherence with maintenance therapy is a widespread problem in patients with IBD. The reasons, which have been mostly determined from demographic profiles and other indirect sources, are not well defined, but efforts to improve adherence should be a priority in clinical care,” reported Dr. Alan C. Moss, Center for Inflammatory Bowel Disease, Beth Israel Deaconess Medical Center, Boston. Dr. Moss made these remarks in the context of a study he presented at the 2011 ACG that was designed to better isolate factors that increase the likelihood of non-adherence. Drawn from 255 detailed response codes from 27 one-hour interviews in IBD patients, five themes were identified by Dr. Moss that he believes can be targets of initiatives to improve adherence.
There is a paradox that is created when excellent control of symptoms create a sense of false security that treatment is no longer needed.
Of these five themes, doubt about the need for medication is among the most troublesome. The other four themes included social embarrassment about taking pills, the inconvenience and cost of refills, absentmindedness, and changes in daily routine that derail efforts to take the medication on schedule. While these are common obstacles to essentially all medications, the clinical trials with mesalamine demonstrate that after acute healing is achieved, there is a rapid attrition to relapse when long-acting formulations are not offered in adequate doses. The data from Dr. Moss indicate a paradox in that excellent and prolonged control of symptoms create the greatest risk of a false security that treatment is no longer needed (Table 1).
“For patients to avoid a repeat of the disease flare that put them on medication, they must understand that adherence is essential not only for well-being but for avoiding complications,” Dr. Moss said.
Ulcerative Colitis – Phase III Trial
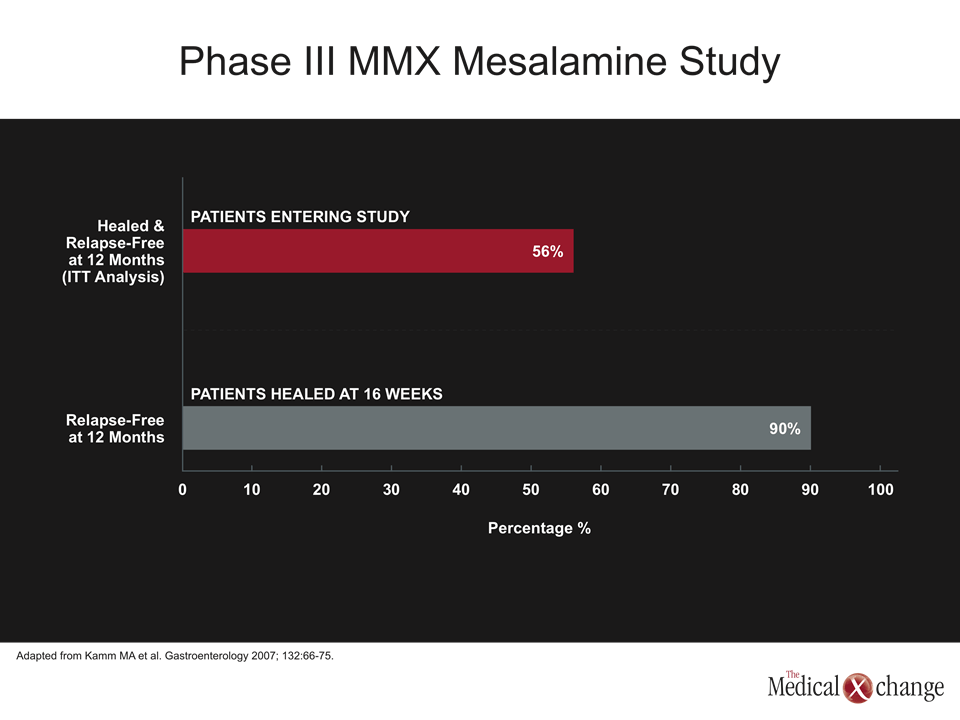
While mesalamine was once thought to offer relatively modest efficacy, large multinational trials have now shown that the majority of patients with a mild to moderate acute flare of UC can expect to achieve healing and then remain relapsed over a long term. One of the most rigorous studies ever conducted was published four years ago (Kamm MA et al. Gastroenterology 2007;132:66-75). In that landmark phase III trial, 221 patients with acute UC were initiated on the multi-matrix system (MMX) formulation of mesalamine (Mezavant®). Thirty-five percent were healed at eight weeks and 60.9% were healed at 16 weeks. Of those healed, 90% remained relapse free over 12 months, but 56.6% of those who entered the study also met this rigorous endpoint (Fig. 1).
The concept of healing as a predictor of long-term remission is being widely adopted.
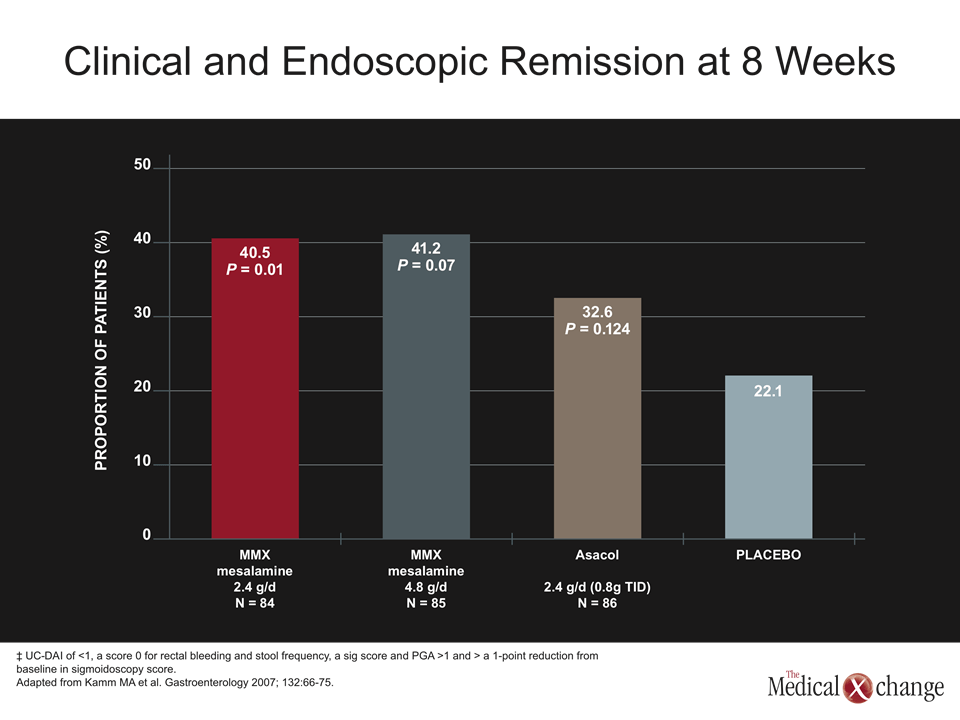
It is notable that this was achieved with once-daily therapy at a dose of either 2.4 or 4.8 mg, both of which were well tolerated. There is a large literature to support the notion that once-daily pills lead to better adherence than pills that require two or more daily doses, but the efficacy of mesalamine is also linked to drug delivery. As most of the anti-inflammatory benefit of these drugs is derived from a topical effect on the mucosa as the drugs descend the lower gastrointestinal tract, the formulation is likely to be critical. Strategies for increasing the amount of drug delivered to the colon not only include the MMX technology but other delayed-release strategies such as an ethyl-cellulose coating (Pentasa®), and granulated sachets (Salofalk®). These are not likely to be interchangeable. Indeed, in the acute phase of the phase III study, the proportion of patients who achieved healing at eight weeks in an arm receiving Asacol®, unlike those receiving MMX mesalamine, was not significantly higher than placebo (Fig. 2).
In the past, a variety of definitions were employed in clinical trials for an endpoint of “complete response.” In particular, mild friability of the mucosa was considered permissible as an isolated finding in the setting of symptom control. However, the concept of healing as a predictor of long-term remission is being widely adopted. At the 2011 ACG, the goal of a workshop sponsored by the U.S. Food and Drug Administration (FDA) was to determine the feasibility of this endpoint as a definition of efficacy. Among expert panelists, including Dr. Brian Feagan, University of Western Ontario, London, and Jean-Frederic Colombel, Mount Sinai School of Medicine, New York City (a co-author of the MMX mesalamine phase III trial) there was strong support for the notion that healing does predict remission and is a valid goal.
Conclusion
The problem of non-adherence in IBD is complex and may be partially driven by periods of disease quiescence when patients either forget to take medication or decide that medication is no longer needed. Mesalamine is effective both for healing and maintenance of therapy, which may be relevant to adherence because it is generally better tolerated than other options and can be taken in once-daily doses with the most effective current formulations. There is increasing evidence that the key variable for long-term remission is healing at the time of acute treatment, but educating patients about the importance of chronic treatment is essential.