gastroenterology
American College of Gastroenterology (ACG) 2011
Improving PPI Therapy: Current Obstacles and Opportunities
Washington, DC – For gastroesophageal reflux disease (GERD), relative acid control is the only meaningful variable for effective therapy. This concept has been blurred by studies that do not distinguish between the sources of upper gastrointestinal (GI) symptoms. Although it is true that pain or discomfort resembling GERD can be caused by other disorders, such as dysmotility, hypersensitivity, or functional diseases that may be driven by abnormal neurotransmitter signaling, the symptoms that stem from reflux of gastric contents into the lower esophagus are acid related in the vast majority of cases. New studies with strategies designed to increase the duration of acid control over each 24-hour dosing period repeat a message that has been restated by every advance which produced an improvement in acid control over the last several decades.
Treatments to Increase Duration of Acid Control
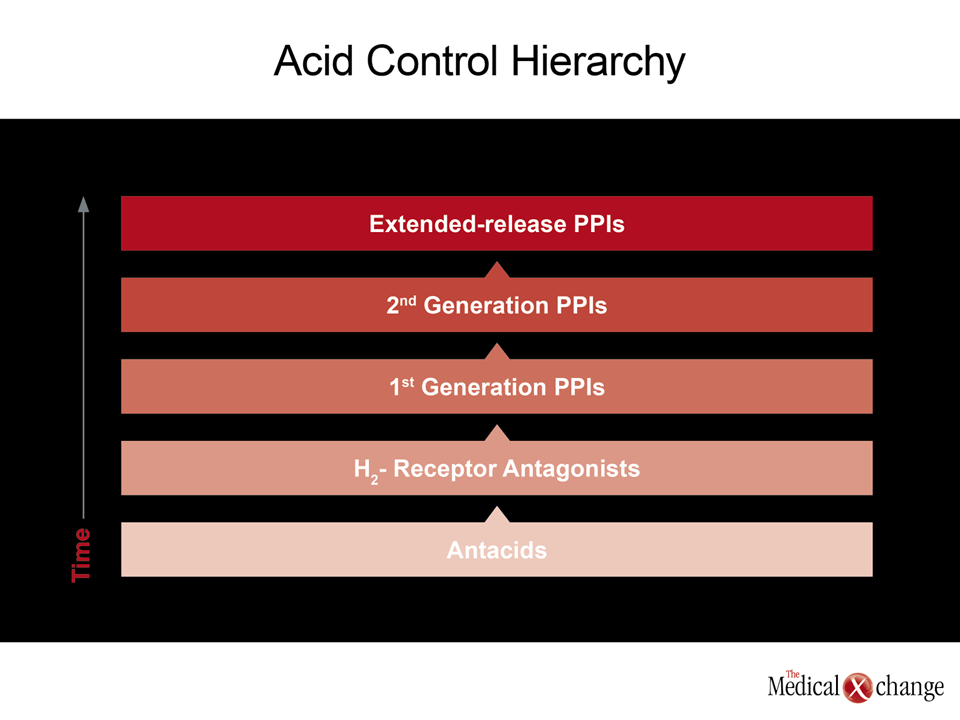
New data at the ACG 2011 meeting have reinforced an old message; control of gastroesophageal reflux disease (GERD) improves each time there is greater and longer duration of acid control over any dosing period. This concept was perhaps first demonstrated when H2-receptor antagonists provided greatly improved and sustained acid control relative to antacids, again when proton pump inhibitors (PPIs) did the same relative to H2-receptor antagonists, again when second-generation PPIs produced more durable acid suppression relative to first-generation PPIs, and most recently when a delayed-release PPI provided more sustained acid control relative to the most potent second-generation agents. Acid control is the common variable.
Based on the importance of acid control, “patients with GERD are commonly prescribed twice-daily PPIs when symptom relief is not adequate on once-daily therapy,” explained Dr. Ronnie Fass, University of Arizona Health Sciences Center, Tucson. Leading a study with the newest delayed-release PPI designed to improve acid control with a single once-daily dose, Dr. Fass cautioned that “the problem with the twice-daily PPI strategy is that it is expensive and most patients prefer not to take two separate doses.”
Changing the formulation of a PPI to improve the duration of effect is an important advance.
Creating better delivery systems of PPIs has been an inevitable next step in the evolution of acid control because it is difficult to improve on the mechanism of PPIs, which block the final common pathway of acid production in gastric parietal cells. While PPIs bind irreversibly to the proton pump, the half-life of PPIs is short so that new subsequent pumps are not blocked. Changing the formulation of a PPI to improve the duration of effect is an important advance.
Maintaining an Extended Relief of Symptoms
Among studies with dexlansoprazole, the first licensed PPI to employ a delayed-release technology to prolong the availability of active drug, a direct comparison confirmed superior acid control to esomeprazole, which has previously demonstrated superior acid control relative to older PPIs (Kukulka M et al. Clin Exp Gastroenterol. 2011;4:213-20). A new study presented at the ACG by Dr. Fass has provided evidence that this advantage is clinically relevant.
In this study, 178 patients being maintained on twice-daily PPI therapy in order to control symptoms of GERD were screened over a six-week period during which they had to maintain a diary of symptoms. At the end of this period, they replaced their PPI with a once-daily morning dose of 30 mg of dexlansoprazole with a matched placebo given for the evening dose. Over the six-weeks on the once-daily therapy, patients continued to maintain a diary of their symptoms.
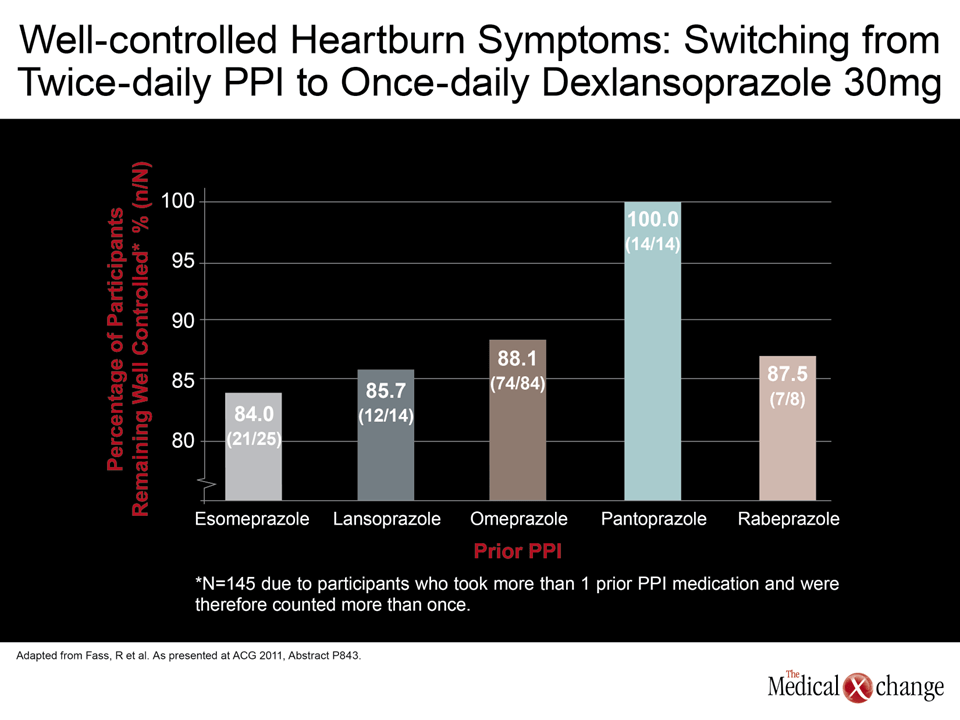
According to patient records, symptoms remained well controlled in 88% of the participants after switching from twice-daily PPI to once-daily dexlansoprazole. When stratified by specific PPI, the persistence of control on once-daily therapy ranged from 84% in those previously managed with esomeprazole to 100% in those previously managed with pantoprazole (Fig. 1). The clinical significance of this relative control was reinforced by standardized quality of life measurements taken at baseline and at the end of the study.
“The majority of GERD participants who required twice-daily PPI to fully control their heartburn were able to step down to once-daily dexlansoprazole without loss of heartburn symptom control,” Dr. Fass concluded from these results. “Baseline levels of GERD-related symptom severity and health-related QOL appear to have been maintained in participants who documented continued heartburn relief in their daily diaries.”
Consistent with PPIs in general, significant adverse events were uncommon and few of those that did occur were thought to be drug related. Based on drug costs, Dr. Fass estimated that the savings from successfully stepping down to once-daily dexlansoprazole from twice-daily PPI therapy even over the six-week study period would be measured in tens of thousands of U.S. dollars.
Impact of Daily Average Pill Consumption
The differences in the relative efficacy of acid control among PPIs in regard to daily average consumption was reflected in a separate medical claims database analysis of 185,506 GERD patients. Of this population, 33.3% were taking omeprazole, 30.2% were taking pantoprazole, 19.6% were taking rabeprazole, 9.6% were taking esomeprazole, and the remainder were taking lansoprazole or dexlansoprazole. Most of those on omeprazole were taking a generic formulation, while the overall proportion of patients on a branded PPI was 56.5%.
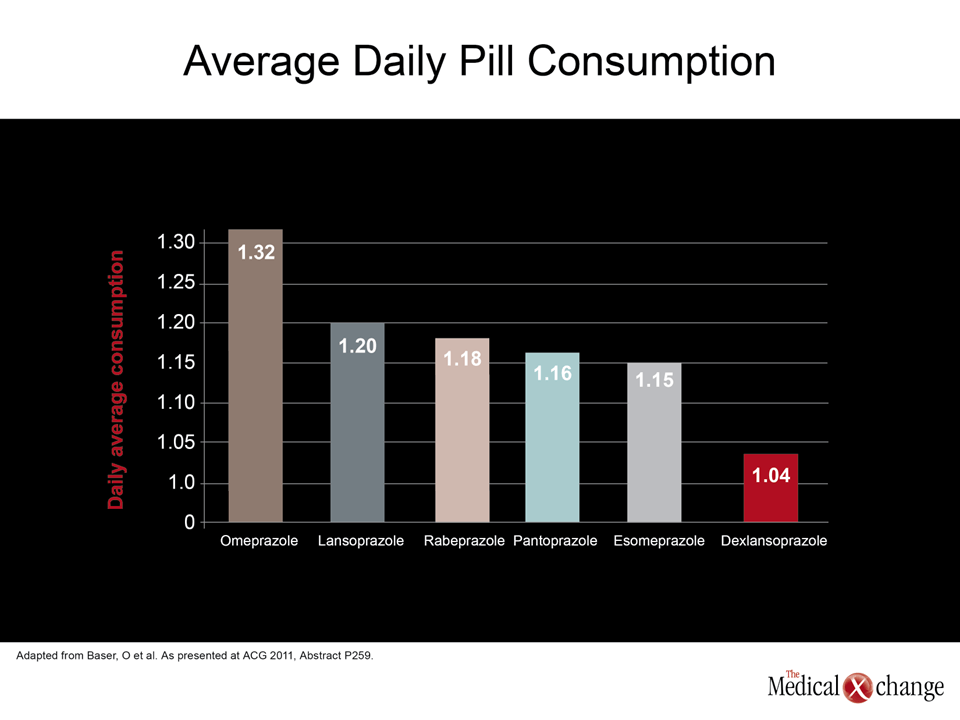
When compared for daily average consumption (DACON), the lowest rate was dexlansoprazole (1.04 pills per day) followed by esomeprazole (1.15 pills per day). The highest DACON was among omeprazole users at 1.32 pills per day (Fig. 2). These findings are consistent with the acid-lowering potency of these agents in several comparative trials. According to the senior author of this study, Dr. Onur Baser, University of Michigan, Ann Arbor, these findings are potentially important to clinical decisions designed to improve symptom control and lower cost.
“The potential impact of reduced DACON on patient adherence, length of treatment, and total and GERD-related healthcare resource utilization and costs requires further evaluation,” Dr. Baser maintained.
Conclusion
In patients with GERD, the therapy providing the greatest suppression of acid over each dosing period will provide the greatest symptom relief. This is a message that has been repeated with each advance that has provided an incremental improvement in acid control over the last several decades. The development of a controlled-release PPI has provided the latest demonstration of this relationship. Importantly, new data suggest that once-daily therapy with the dexlansoprazole extended-release formulation provides a degree of symptom control comparable to twice-daily regimens with other PPIs.
Additional Slide
Figure 3 (Fig. 3).