Rheumatology
2011 ACR/ARHP Annual Scientific Meeting
New Preliminary ACR Guidelines Released for Management of Gout
Chicago – Gout is becoming more common in our aging population and its links to other age-related and life-threatening conditions are increasingly evident. Based on a thorough review of current evidence, new recommendations for gout management, issued at this year’s meeting in preliminary form by the American College of Rheumatology (ACR), offer guidance to rheumatologists and general healthcare providers on the treatment of acute attacks, management of chronic tophaceous gouty arthropathy, and on prophylaxis with lifestyle measures, anti-inflammatory agents and medications that lower serum urate levels.
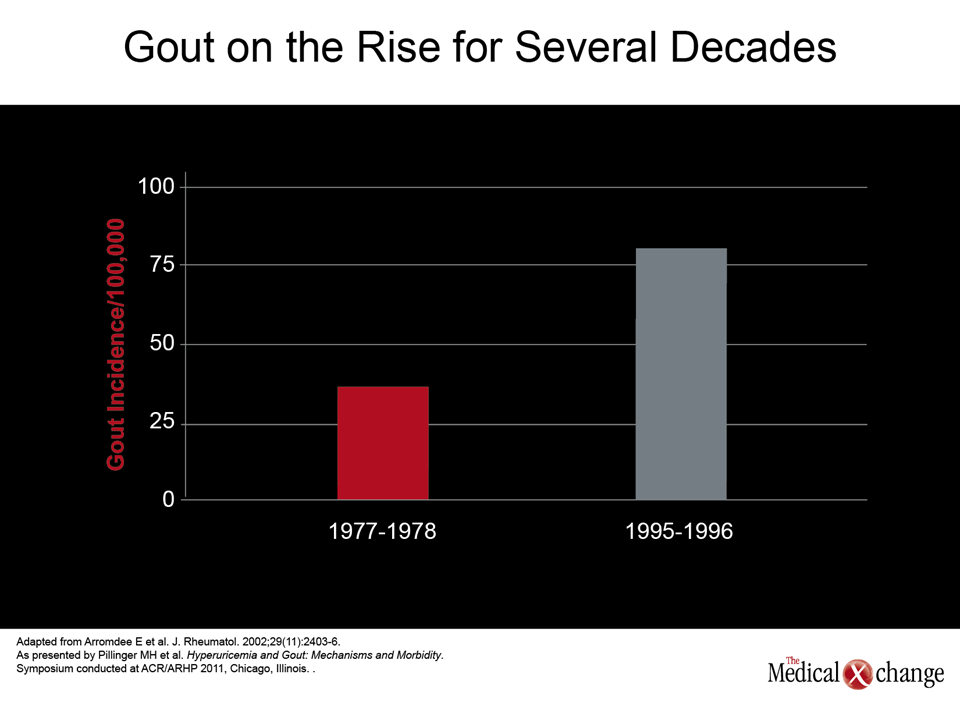
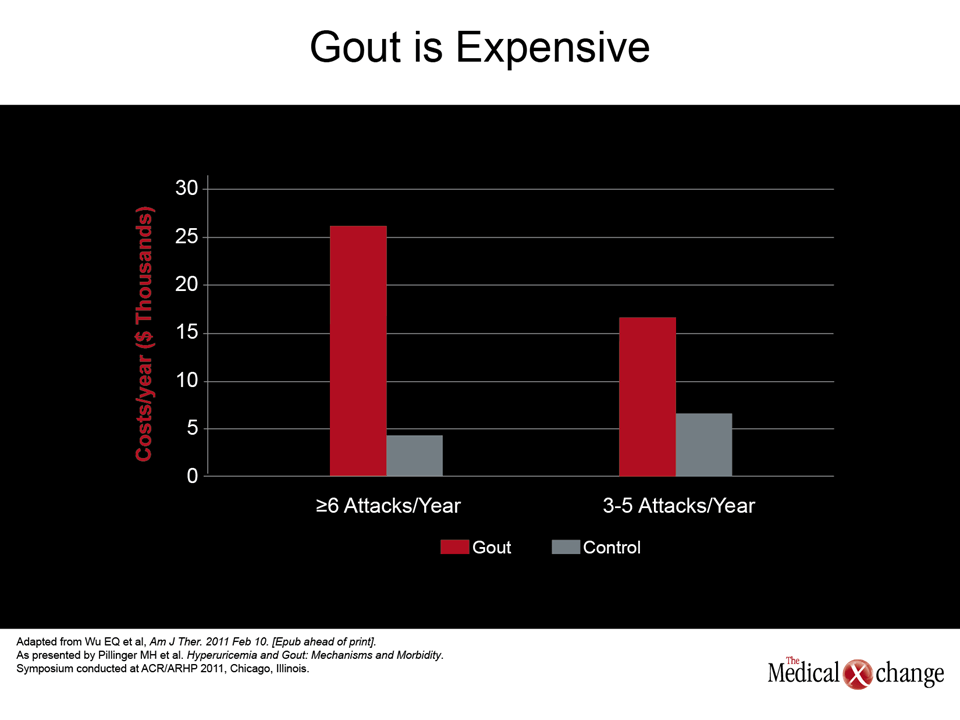
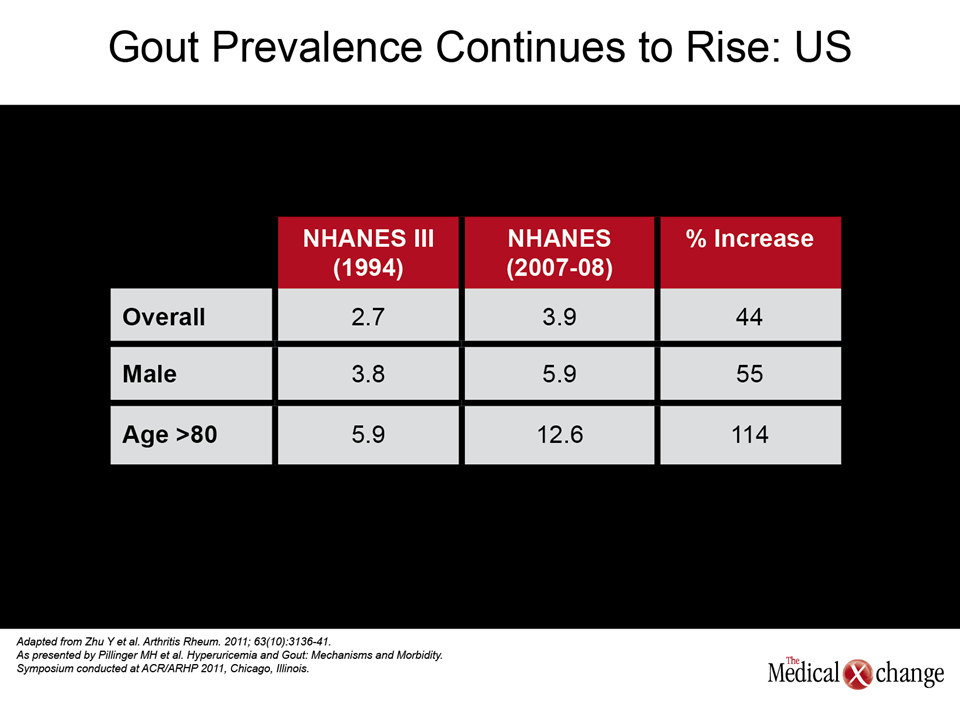
The incidence and prevalence of gout have been increasing steadily over the last two decades in North America as have costs associated with its management. Likely explanations for this evolution in epidemiology include the aging and increasing obesity of the North American population (Fig. 1). Gout often occurs in patients with other age- and lifestyle-related conditions, including the metabolic syndrome, coronary artery disease, hypertension, diabetes and kidney disease. In a recent Canadian study, the 5-year incidence of gout among approximately 20,000 elderly individuals was 4.4%; over the study period, the extra health care costs for each gout patient compared with controls amounted to about $8000 (Hanly JG et al. J Rheumatol 2009;36(4):822-30). In the United States, there has been a 44% rise in gout prevalence overall since 1994; the prevalence in patients aged >80 has increased by 114% (Zhu Y et al, Arthritis Rheum 2011;63(10):3136-41).
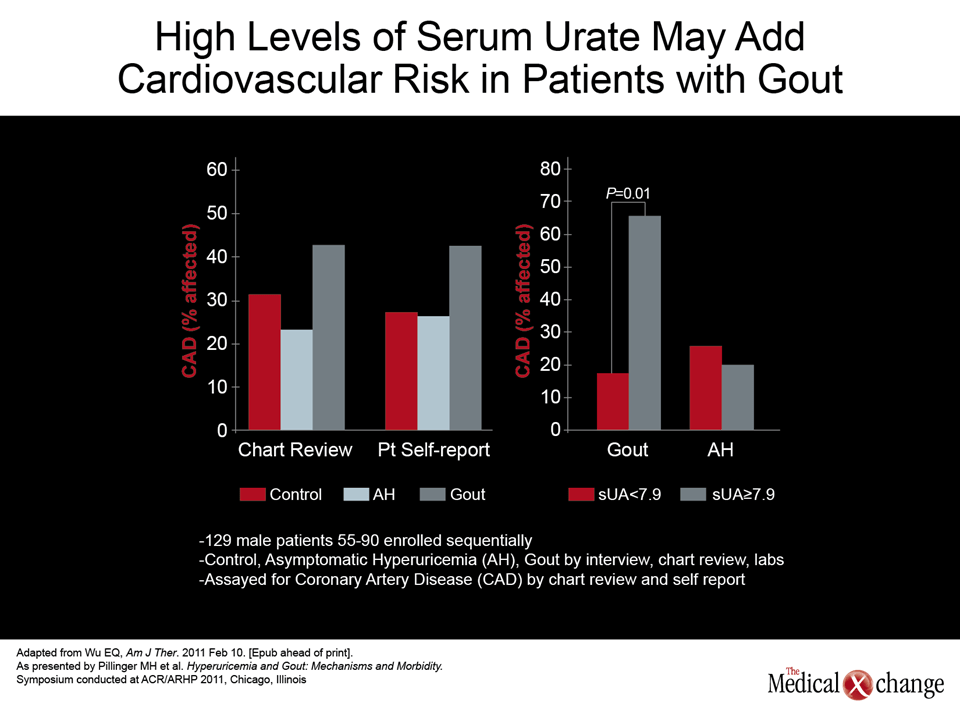
Appropriate management of gout is important not only because of its negative impact on patients’ quality of life, but because hyperuricemia has been linked to the development of cardiovascular disease and events.
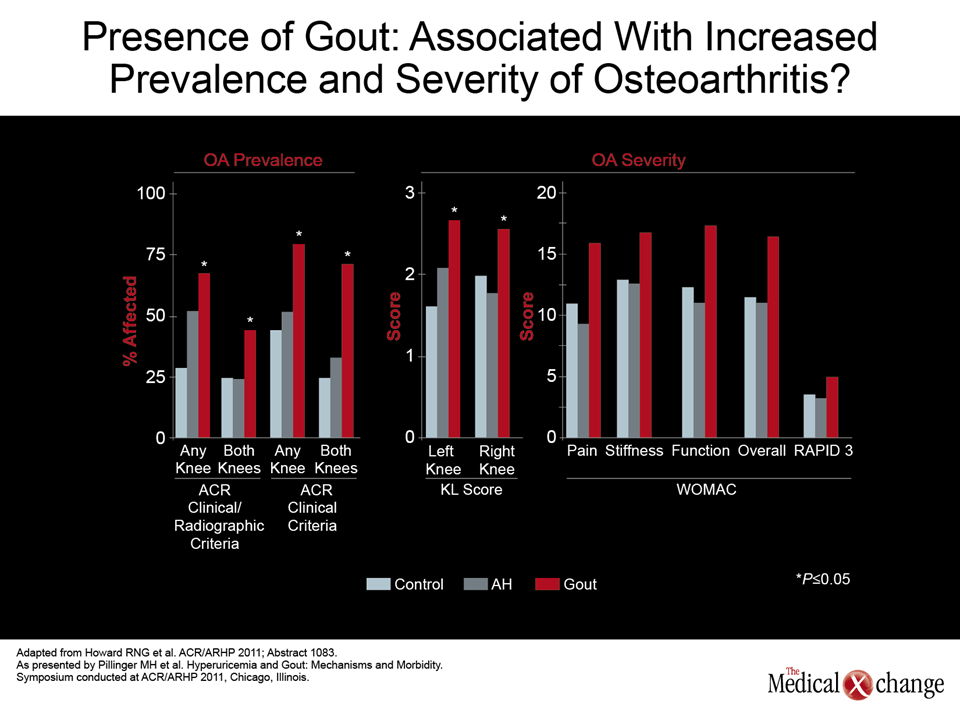
Appropriate management of gout is important not only because of its negative impact on patients’ quality of life, but because hyperuricemia has been linked to the development of cardiovascular disease and events. Gout is also associated with increased severity of osteoarthritis, according to studies presented this year’s ACR/ARHP meeting.
Treatment Principles
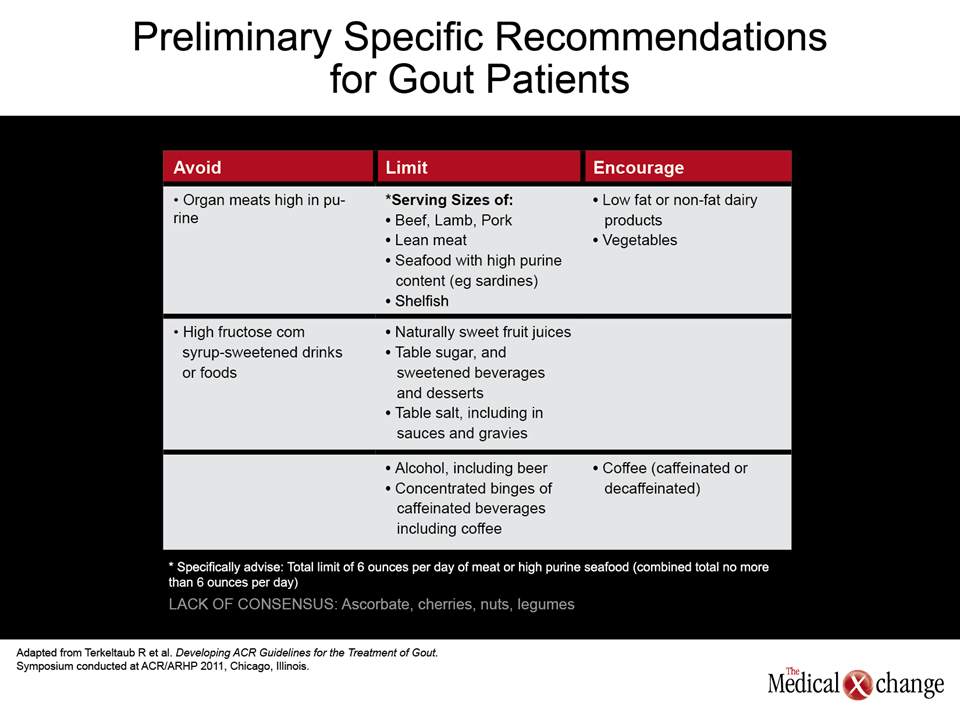
According to new recommendations by the American College of Rheumatology, patients with gout should be evaluated for symptom severity and tophus burden, hyperuricemia and possible contributing factors, and comorbidities. Treatment of an acute gout attack should be initiated within 24 hours of onset. Patients should be educated about lifestyle measures to prevent further attacks, which may include weight loss, maintaining a healthy diet (e.g., limiting alcohol and foods high in purines and high-fructose corn syrup), smoking cessation, appropriate hydration, and regular exercise (Fig. 2). Patients with gout should also be given instructions for initiating treatment at home when an attack occurs.
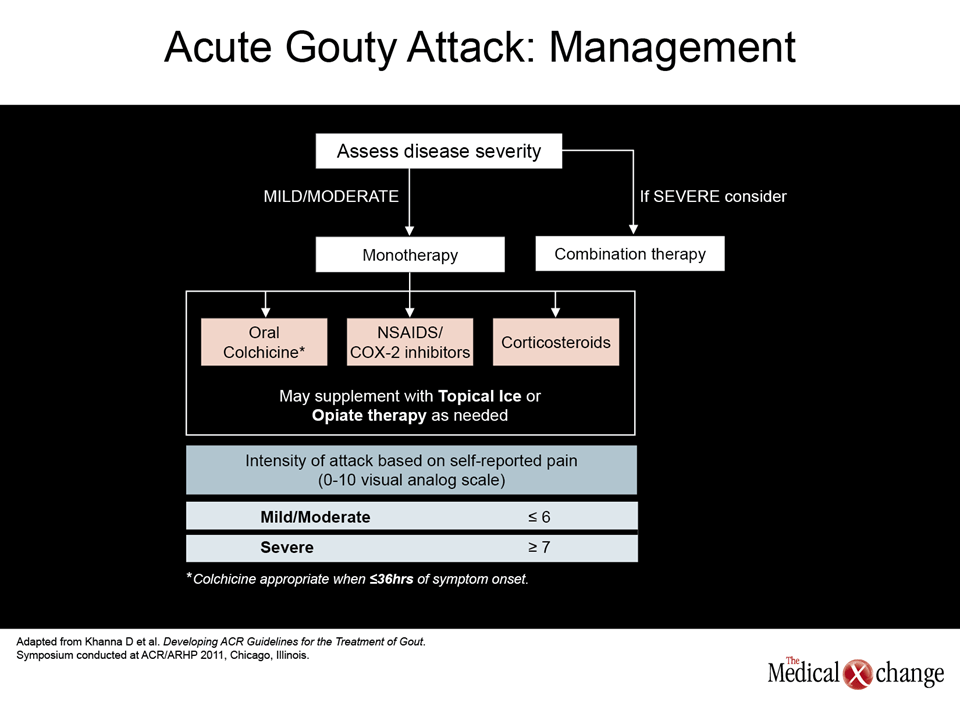
Acute Attacks
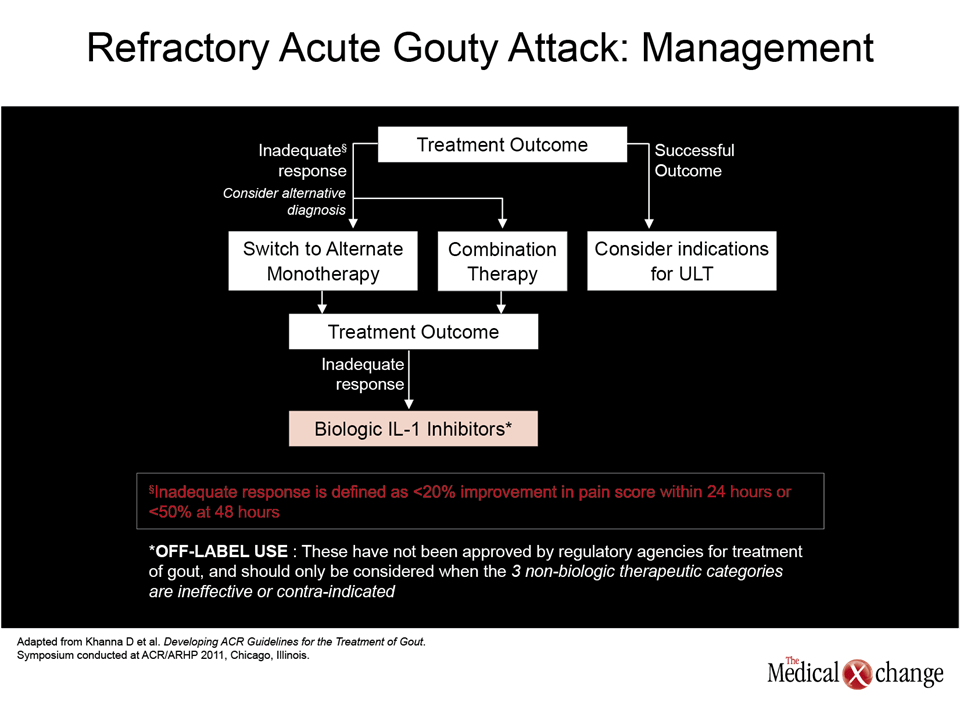
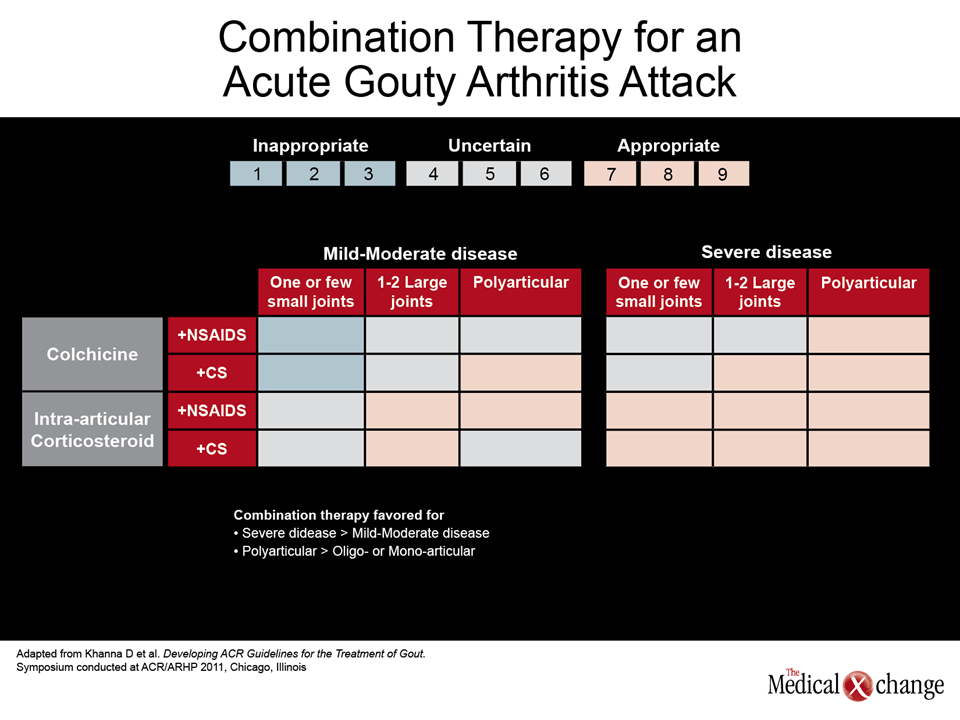
Mild to moderate acute gout – in which the patient’s pain is <6 on a visual analog scale – can typically be treated with oral colchicine (within 36 hours of symptom onset), a non-steroidal anti-inflammatory drug (NSAID), or a corticosteroid. More severe attacks, extensive disease, or initial nonresponse to monotherapy (e.g., <20% improvement in pain within 24 hours or <50% improvement after 48 hours) should prompt consideration of combination therapy. ACR recommendations now in development indicate that biologic interleukin-1 inhibitors are an emerging but as yet unapproved option for patients with an inadequate response to the more common therapies. Pain may be further alleviated with topical ice or opiates, as needed.
Chronic Gout
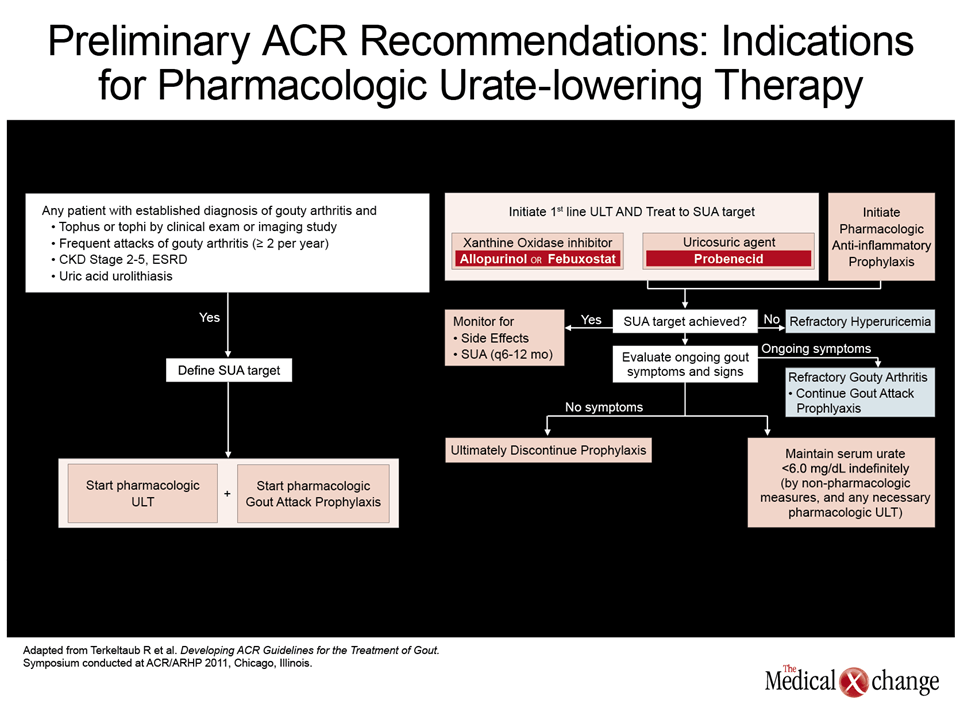
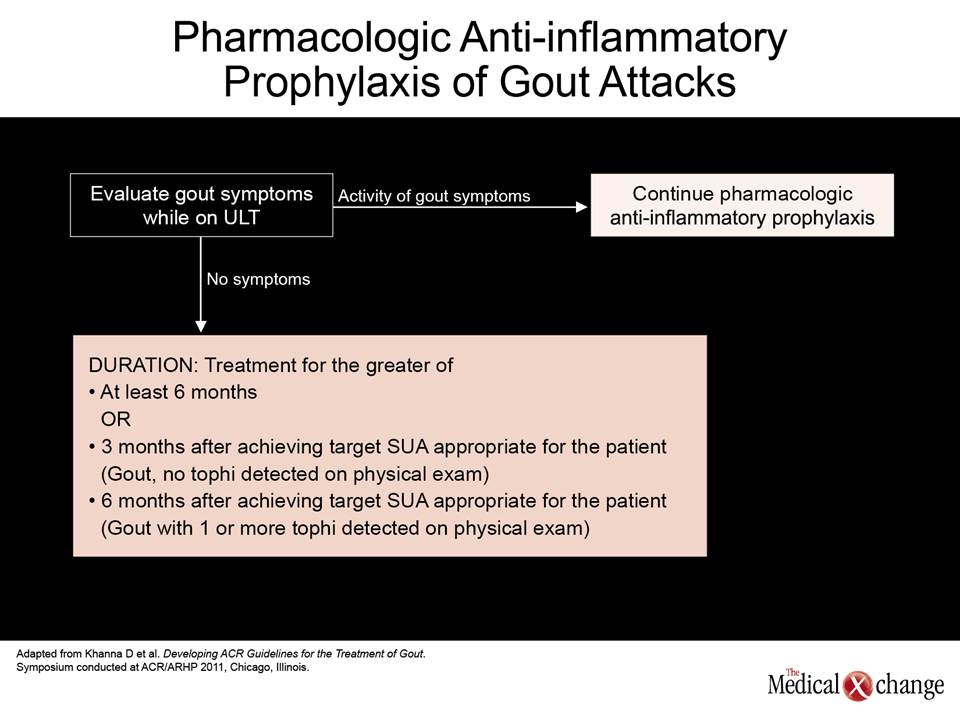
Managing gout over the long term shouldinclude anti-inflammatory agents and urate-lowering therapy (ULT). The diagnosis of gout should be confirmed before ULT is initiated. Along with clinical evaluation and synovial fluid analysis, the use of high resolution ultrasound is recommended for detection of urate crystal deposition or findings suggestive of tophi. Patients with gout and one or more tophi or who have experienced at least two acute gout attacks in one year may benefit from pharmacologic ULT. Other indications include chronic kidney disease and uric acid urolithiasis. As shown in (Fig. 3), first-line ULT for all gout patients is a xanthine oxidase inhibitor (XOI), and includes either allopurinol or febuxostat. ULT should be given at least until the desired serum uric acid (SUA) concentration is achieved and maintained. The usual target is <6 mg/dL (<360 μm/L). Upward dose titration of the XOI or a change of medication may be needed if the SUA target is not met with initial therapy. Probenecid is an alternative if either XOI fails, and is the first choice among uricosuric agents. The combination of an XOI and uricosuric is acceptable if the SUA is not adequately decreased with monotherapy. The agent pegloticase is another option for patients with severe gout whose condition is refractory to or who are intolerant of other ULTs. The SUA should be monitored and maintained at or below the prescribed target. Continued pharmacologic therapy is recommended for those with ongoing symptoms or refractory gouty arthritis. Low-dose anti-inflammatory prophylaxis should be started before or at the same time as ULT. Recommended regimens are colchicine once or twice daily, an NSAID plus a proton pump inhibitor, prednisone or prednisolone. Anti-inflammatory prophylaxis typically continues for at least six months, or three to six months after the patient has achieved the prescribed SUA. (The shorter duration is recommended only for patients without tophi.)
Conclusion
The new preliminary ACR recommendations offer guidance for management of gout, according to severity and persistence of symptoms. After acute management, anti-inflammatory drugs and medications to ensure maintenance of the target SUA may be required for prophylaxis. The detailed recommendations will be published shortly in a peer-reviewed journal.
Additional Slides
Figures: (Fig. 4), (Fig. 5), (Fig. 6), (Fig. 7), (Fig. 8), (Fig.9), (Fig. 10), (Fig. 11) and (Fig. 12).