psychiatry
165th American Psychiatric Association (APA) Annual Meeting
Refining Goals in the Pharmacological Control of Attention Deficit Hyperactivity Disorder
Philadelphia – Progress is being made in defining the next step in the control of attention deficit hyperactivity disorder (ADHD) when standard regimens fail or are inadequate. At the 2012 American Psychiatric Association (APA) Annual Meeting, positive results have been reported with both a novel therapy and a new delivery system designed to improve control in suboptimal treatment of ADHD. The alternatives are filling a large gap that is now largely bridged by empiric use of unproven psychoactive therapies, particularly atypical antipsychotics. The considerable potential risks of atypical antipsychotics have increased demand for alternatives. The current effort to improve control of ADHD refractory to first-line psychostimulants has major implications for a more rational approach to a disorder which now affects nearly 10% of school-aged children.
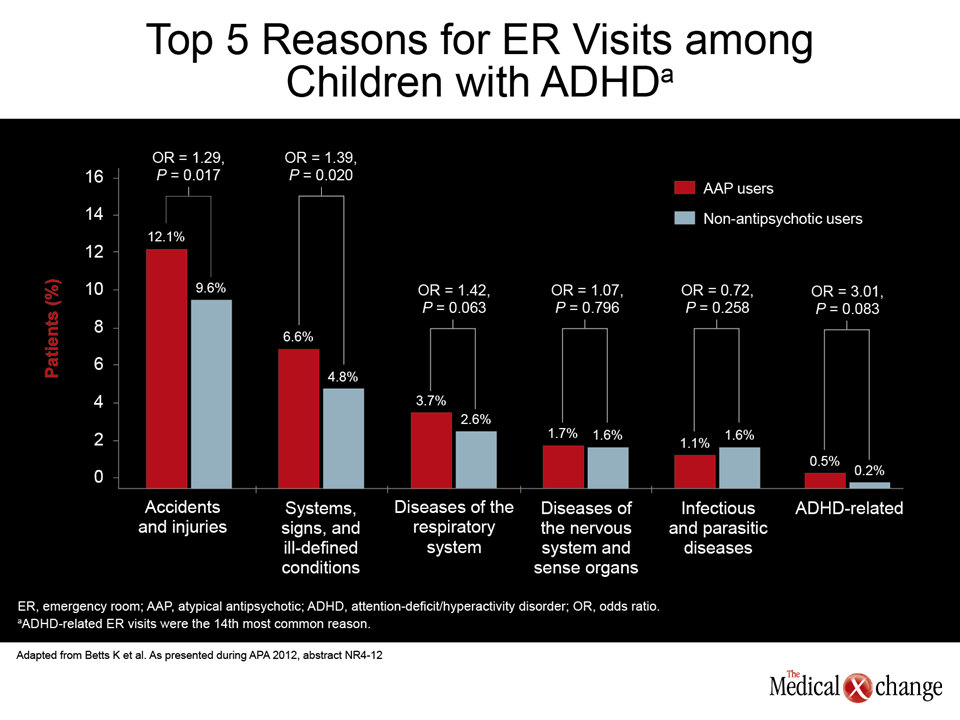
A series of reports delineating the efficacy of new strategies for control of suboptimal treatment of attention deficit hyperactivity disorder (ADHD) were presented at the same session in which data outlined the unintended adverse consequences of off-label use of atypical antipsychotics. Used increasingly, despite limited supportive data for efficacy, some atypical antipsychotics have adverse systemic effects, such as altered glucose metabolism, that have long-term health consequences. In one study presented at this year’s American Psychiatric Association (APA) Annual Meeting, the rate of urgent care and hospitalizations was higher in ADHD children who were exposed to atypical antipsychotics when compared to those who were not.
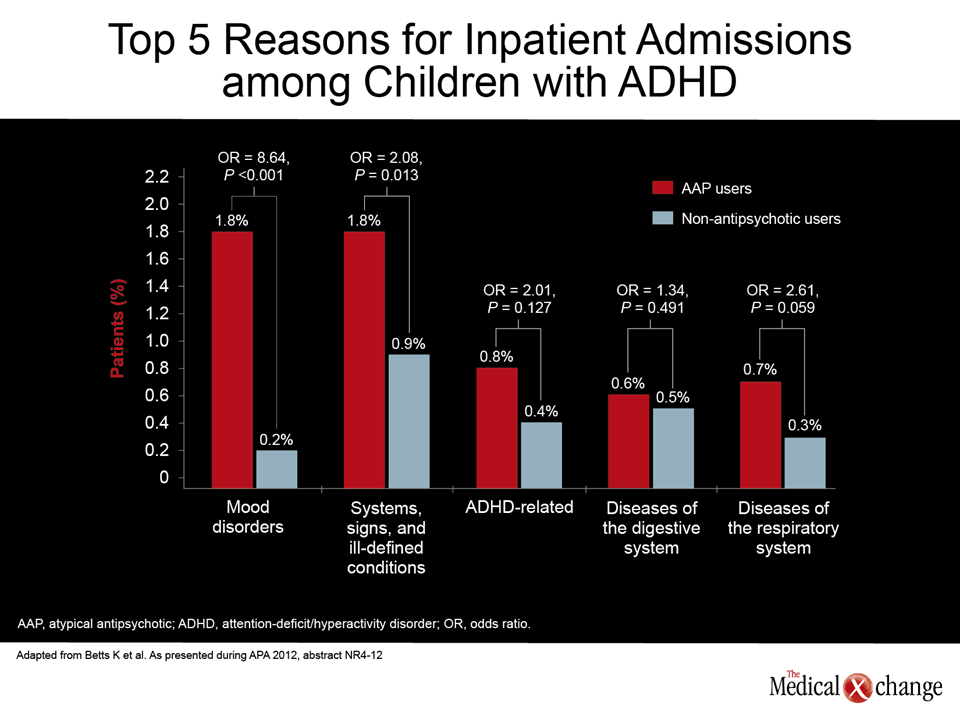
“Emergency room visits occurred at a rate that was more than one third greater [23.8% vs. 18.5%; OR 1.37; P<0.001] while in-patient admissions were more than twice as great [4.5% vs. 1.8%; OR 2.54; P<0.001],” reported the lead author of this study, Dr. Stephen R. Pliszka, University of Texas Health Science Center, San Antonio.
In this study, patients aged 6 to 12 years with an ADHD diagnosis who received at least one stimulant prescription were identified in a large claims database. Patients with a primary diagnosis other than ADHD were excluded. In matched cohorts of 1,857 patients each, the greater rate of emergency room visits and hospitalizations among those receiving atypical antipsychotics compared to those who did not was particularly marked for mood disorder, which was 8.64-fold greater (P<0.001) among those exposed to an atypical antipsychotic. In another study led by Dr. Pliszka, results were similar in adolescents aged 13-17.
Alternative strategies for suboptimally-treated ADHD have emerged. At the APA, data were presented on an extended-release formulation of guanfacine, which is approved by the U.S. Food and Drug Administration (FDA) as a monotherapy and as an adjunctive treatment for children with ADHD. It has now been tested in children with an inadequate response to first-line psychostimulants. The advantages of using agents with supportive safety and efficacy data as well as an indication for treatment are considerable.
A phase III study with guanfacine, a selective alpha-2a adrenergic agonist, in inadequate responders to first-line psychostimulants was published earlier this year (Wilens et al. J Am Acad Child Adolesc Psychiatry 2012;51(1):74-85). In the multicenter, double-blind, placebo-controlled study, 461 patients with a partial but inadequate response to a first-line psychostimulant were randomized to a morning dose of guanfacine, an evening dose of guanfacine, or placebo. All patients remained on their initially prescribed psychostimulant. Relative efficacy was compared with the ADHD Rating Scale IV (ADHD-RS-IV) and Clinical Global Impression (CGI) scales, while safety was also closely monitored.
Both the morning dose plus psychostimulant (P=0.002) and the evening dose plus psychostimulant (P 0<0.001) demonstrated significant improvements in the ADHD-RS-IV measure relative to placebo plus psychostimulant. Both doses also provided significant improvements in CGI measures, including the CGI Improvement (CGI-I) scale, although the difference achieved greater significance for the evening dose (P=0.003) relative to the morning dose (P=0.024). The tolerability of guanfacine on top of a psychostimulant was no different from placebo alone.
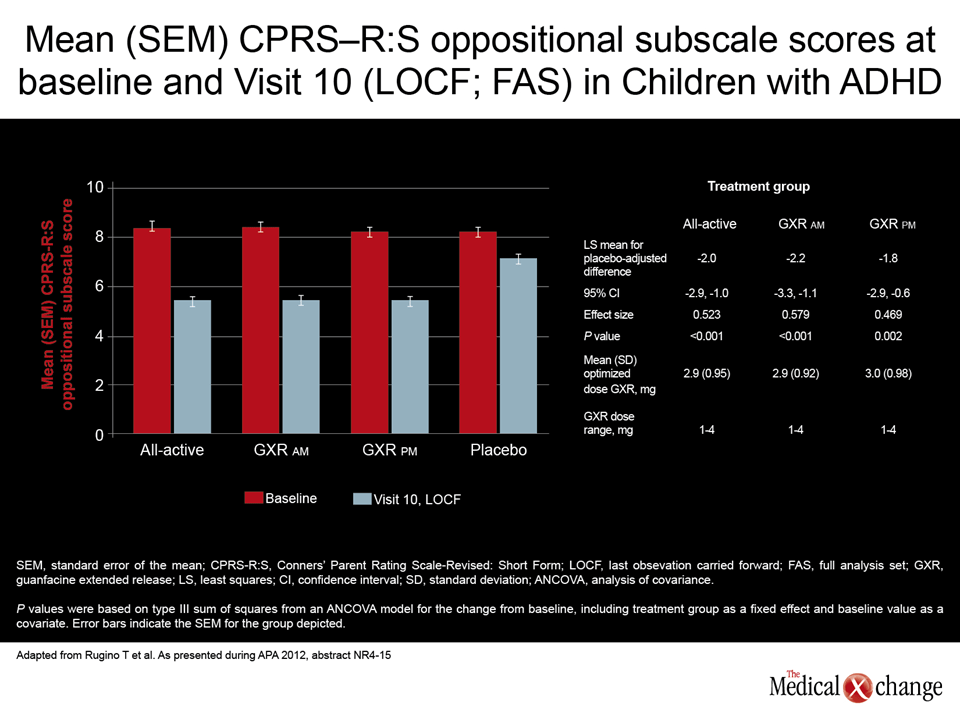
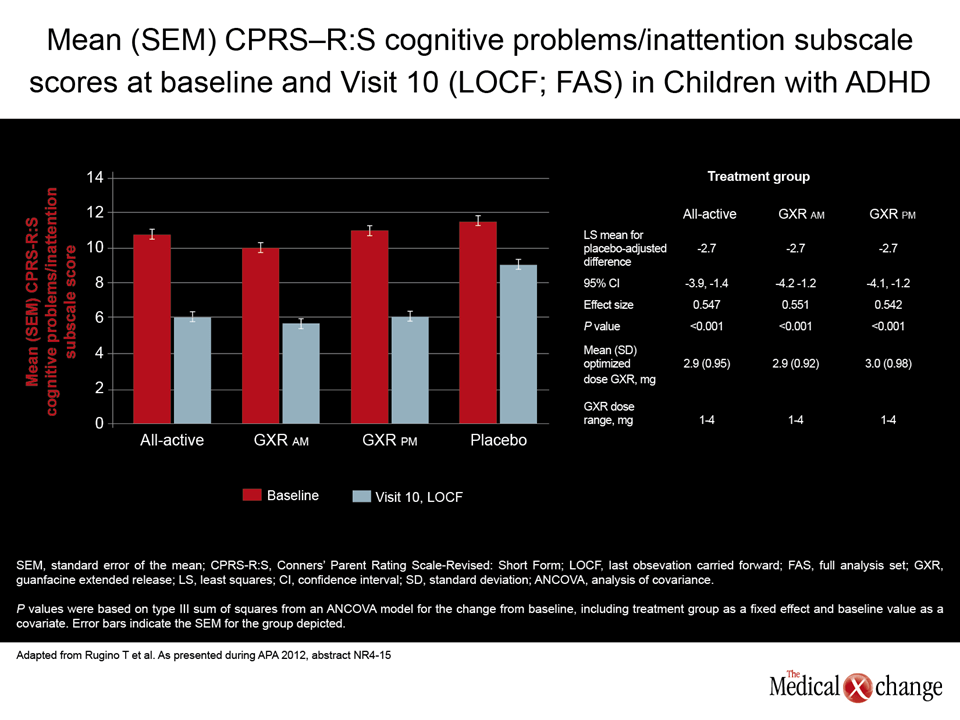
New data presented here reinforced the efficacy of guanfacine as a stand-alone agent in ADHD, providing an explanation why its unique mechanism of action permits it to act as a substitute for psychostimulants or as an add-on therapy. In the phase 3b, double-blind, randomized, multicenter study, 333 children between the ages of 6 and 12 years with ADHD were randomized to extended-release guanfacine in the morning, to extended-release guanfacine in the evening, or to placebo. The primary efficacy endpoint was the ADHD-RS-IV.
“At the final on-treatment assessment at 8 weeks, the changes from baseline in the ADHD-RS-IV scores for the active treatment groups were significantly improved versus placebo with significant [P<0.001] effect sizes,” reported
Dr. Thomas Rugino, Children’s Specialized Hospital, Toms River, New Jersey. “Improvement was seen across a broad range of ADHD-related symptoms and support previously reported observations showing guanfacine treatment-related improvements in ADHD symptoms as measured by the ADHD-RS-IV.”
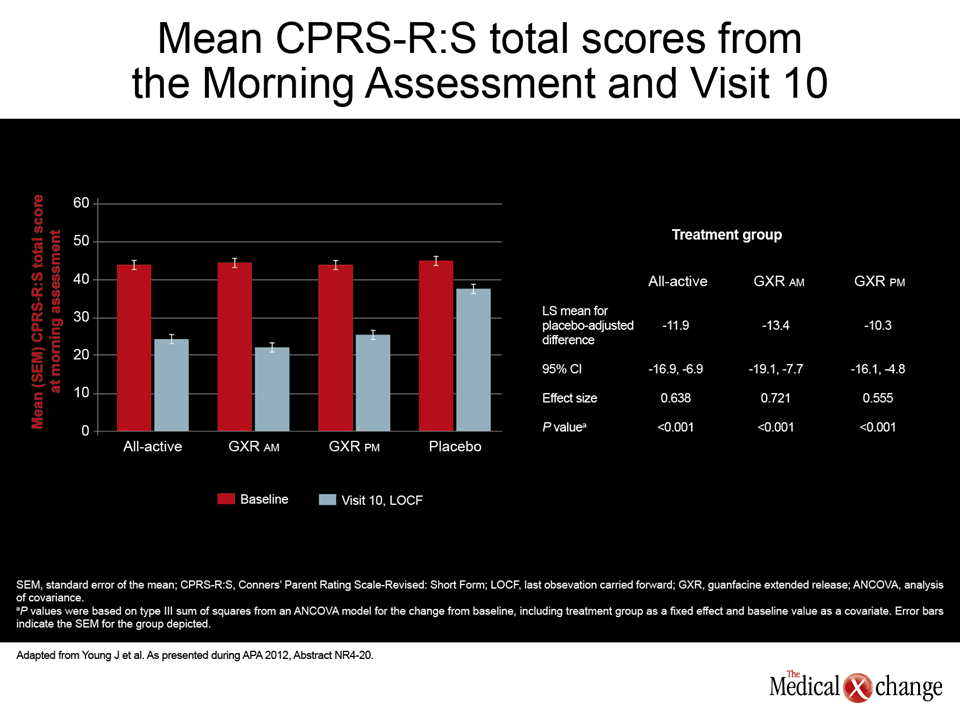
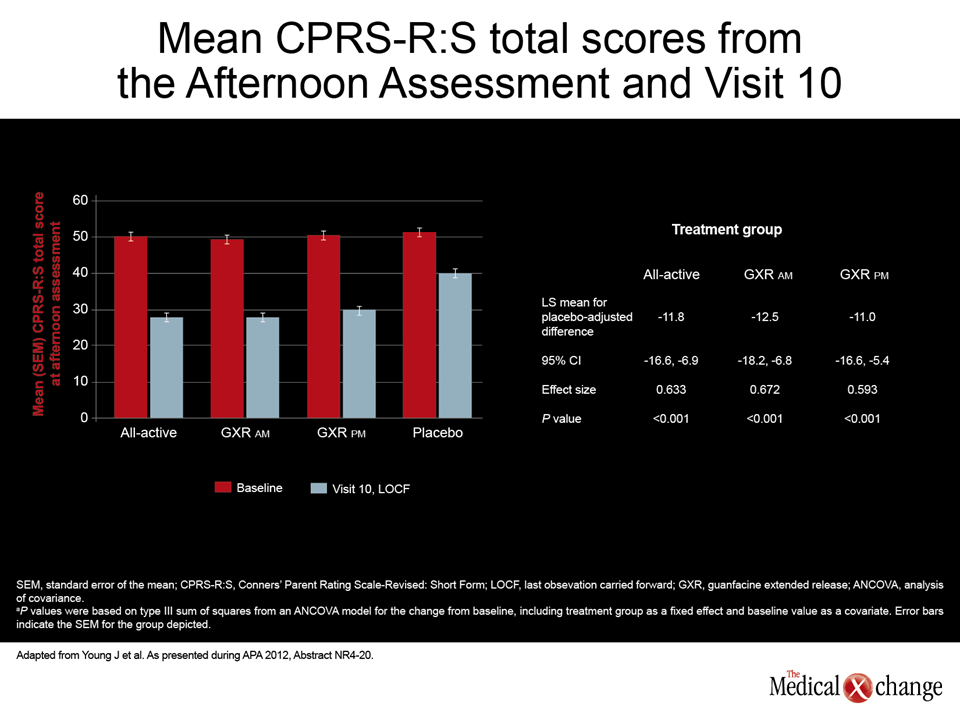
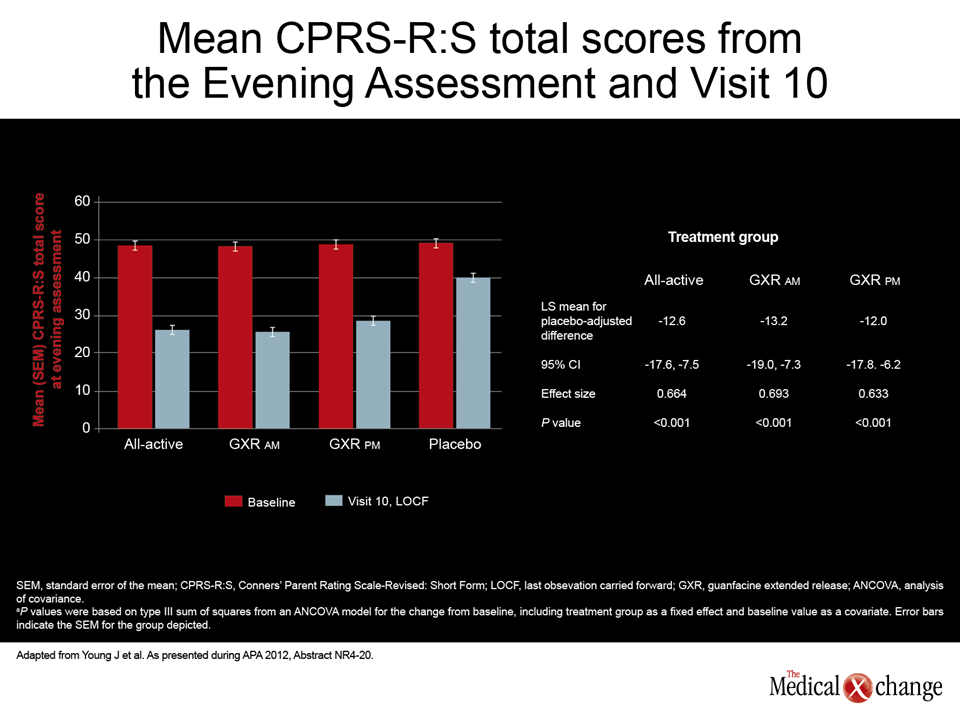
In a substudy that evaluated relative morning, afternoon, and evening symptom control with the morning versus the evening dose of guanfacine, the reductions were remarkably similar. Relative to placebo, the significantly greater reductions in the morning and evening dose groups were similar to each other and to the composite active treatment reduction (Figures 1 (Fig. 1), 2 (Fig. 2) and 3 (Fig. 3)).
Conclusion
There is an urgent need for effective alternatives or adjunctive therapies to first-line psychostimulants. While the use of longer acting formulations has been one approach to improving efficacy, the development of a novel agent with an alternative mechanism of action is an important direction for substitution or augmentation of therapy in ADHD patients inadequately controlled with current licensed options.
Additional Slides
(Figures 4 (Fig. 4), 5 (Fig. 5), 6 (Fig. 6)) and 7 (Fig. 7)).
The methylphenidate transdermal system is currently approved by the U.S. Food and Drug Administration.