Respirology
American Thoracic Society (ATS) 2012 International Conference
Treating the Airways in COPD: Controlling the Dyspnea that Hinders Rehabilitation and Quality of Life
San Francisco – Control of dyspnea, as part of a comprehensive management scheme in individuals with chronic obstructive pulmonary disease (COPD) has implications for prolonged survival. New data presented at the American Thoracic Society (ATS) 2012 International Conference has associated increased exercise capacity with a highly significant reduction in the risk of death over a follow-up exceeding 10 years. As a key factor in the ability to pursue exercise-related improvements in survival, control of dyspnea is among critical components in a management plan that serves as a paradigm shift designed to move from simple control of symptoms to protection against exacerbations and better long-term outcomes. Recent improvements in therapeutic options appear to be highly effective against dyspnea, which by increasing inspiratory capacity can be an important factor in attenuating the functional decline that increases the likelihood of exacerbations. This has provided the platform for redirecting the therapeutic goals in COPD from symptom control to improved survival. As an early domino in the cascade of events leading to exacerbations and end-stage disease, dyspnea is an important although not isolated target in the effort to improve COPD control.
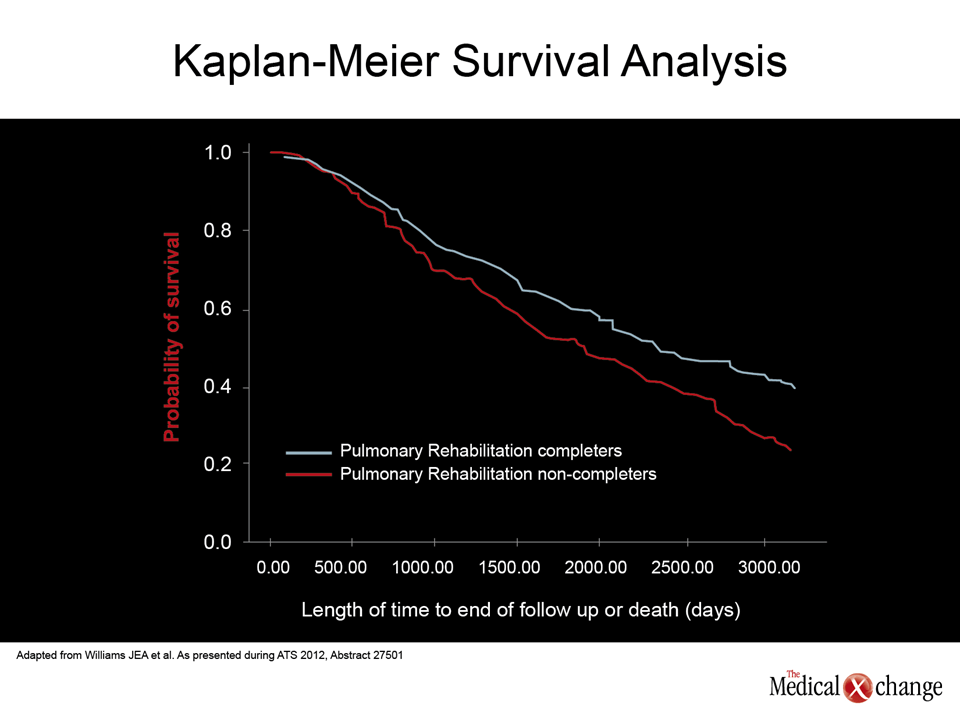
The seven chronic obstructive pulmonary disease (COPD) treatment goals listed in the influential Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report are not just interrelated but inseparable. Such goals as preventing and treating exacerbations and improving exercise tolerance are fundamental to the seventh and ultimate goal of reducing mortality. Successful interventions that halt or slow the progression of COPD depend on control of dyspnea, a key manifestation of the disease. “COPD is a progressive disease characterized by persistent airflow limitation with chronic and progressive dyspnea,” reported Dr. Stephen I. Rennard, Larson Professor of Medicine, University of Nebraska Medical Center, Omaha. While dyspnea is a “characteristic strongly associated with reduced health-related quality of life,” it is also a pivotal symptom for loss of functional capacity that sets the stage for exacerbations and advancing COPD. The evidence that pulmonary rehabilitation has a mortality benefit was generated by an observational study in which completion of a rehabilitation program predicted survival. When completers were compared to non-completers in a series of 1615 patients, survival curves separated after about two years and continued to widen over the full 10 years of follow-up. After 10 years, the absolute survival advantage was approximately 15% (40% vs. 25%; P<0.001) with a relative survival advantage of more than 50% (Fig. 1).
For patients who are enabled, exercise “may literally be a matter of life and death.”
For patients who are enabled, exercise “may literally be a matter of life and death,” reported the senior author of this study, Dr. Johanna Williams, Department of Respiratory Medicine, University Hospitals of Leicester, UK. She indicated that these data intensify the effort to control exercise-limiting symptoms in order to permit rehabilitation.
Treatment Options to Control Dyspnea
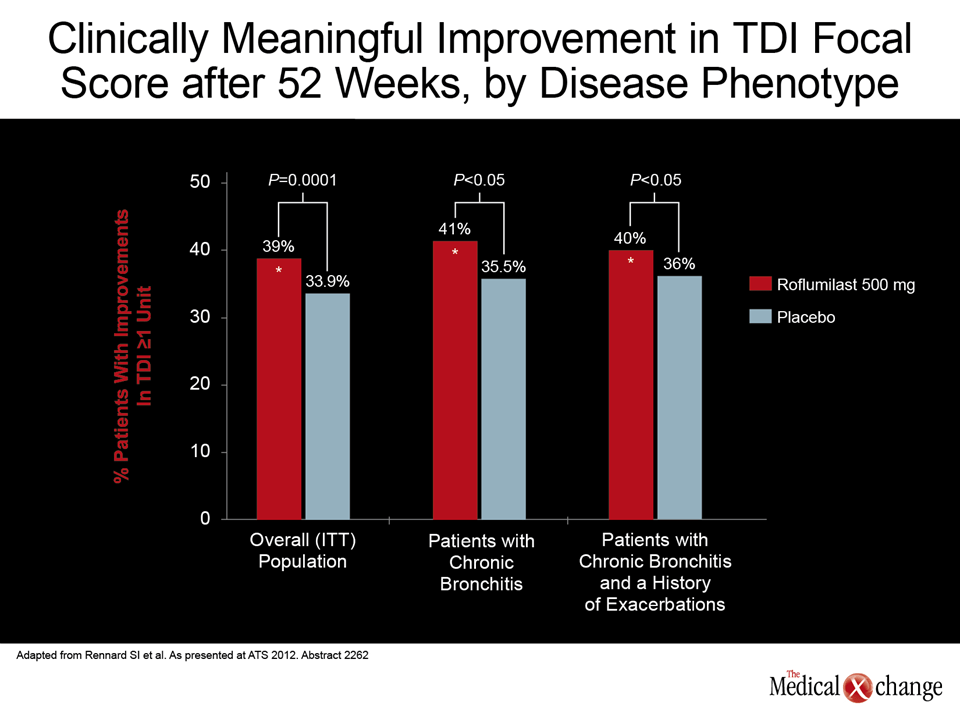
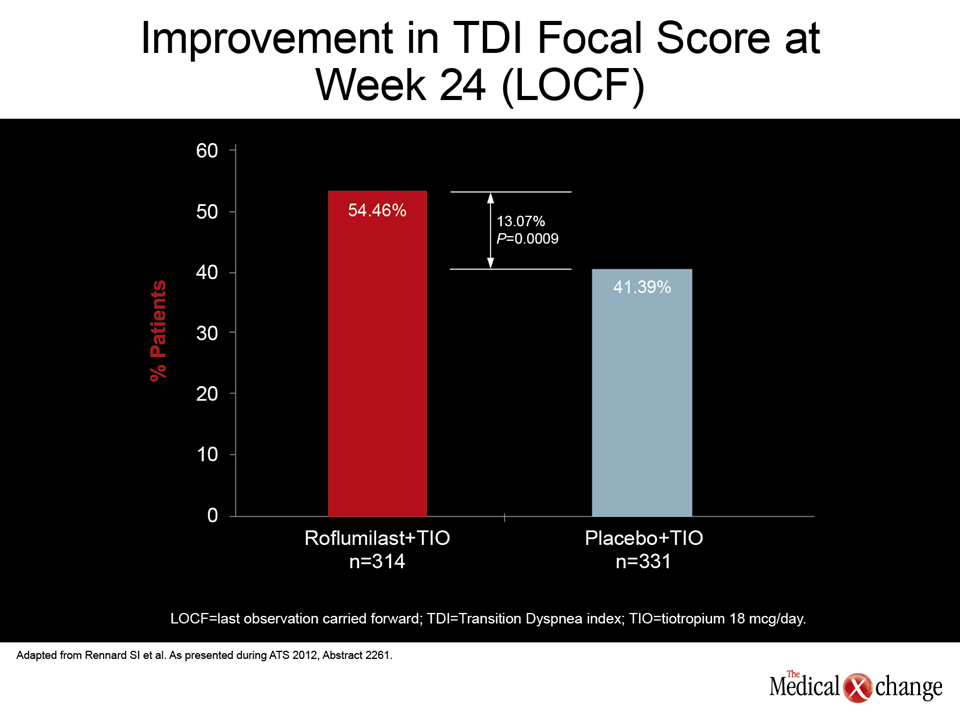
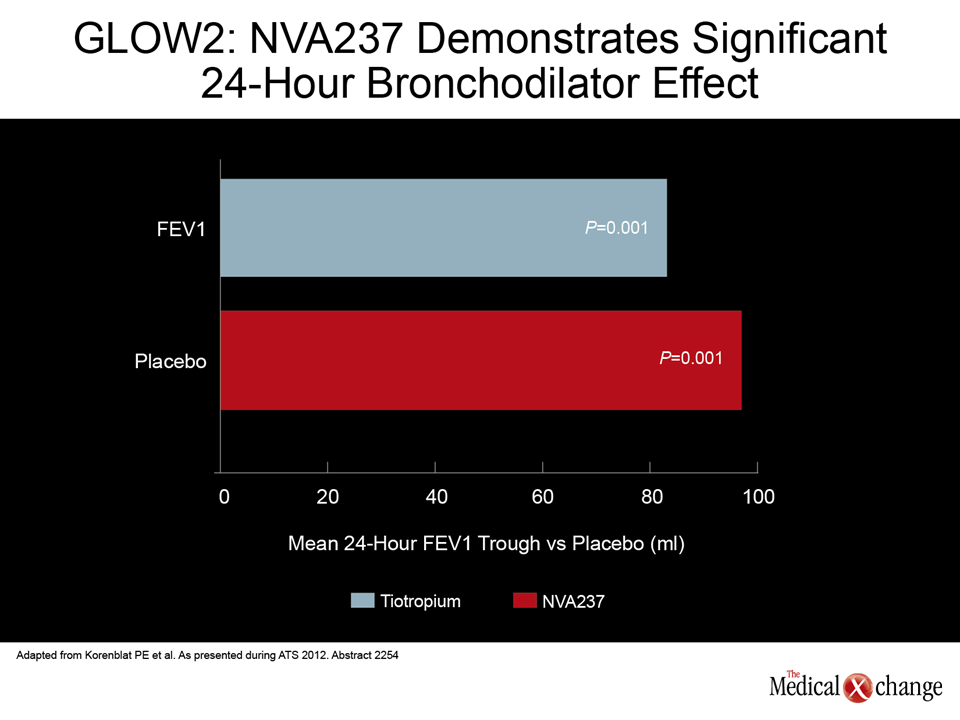
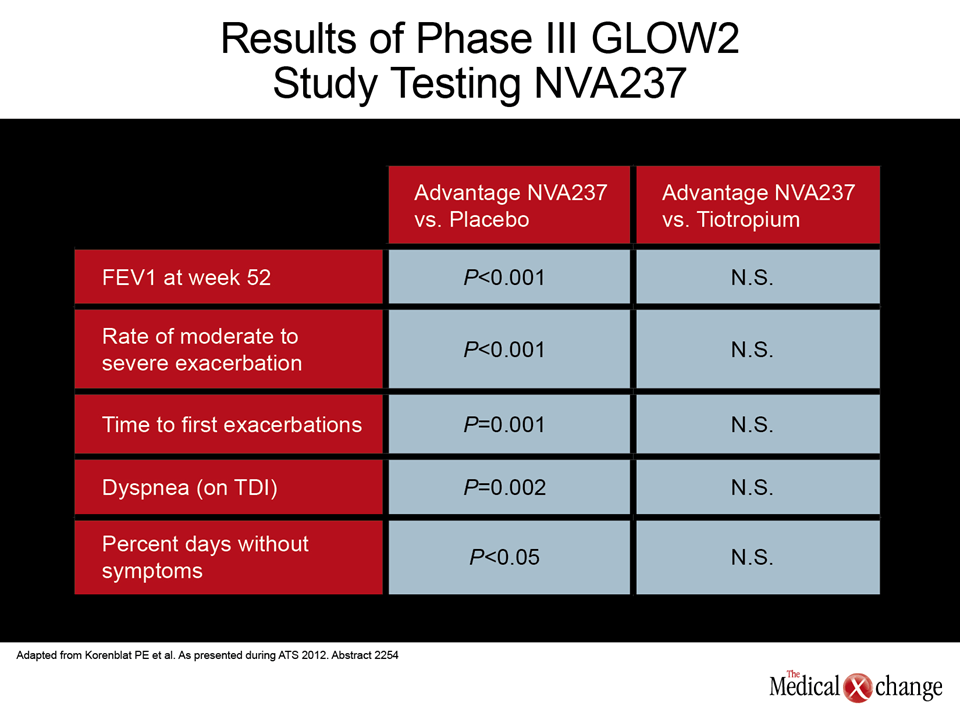
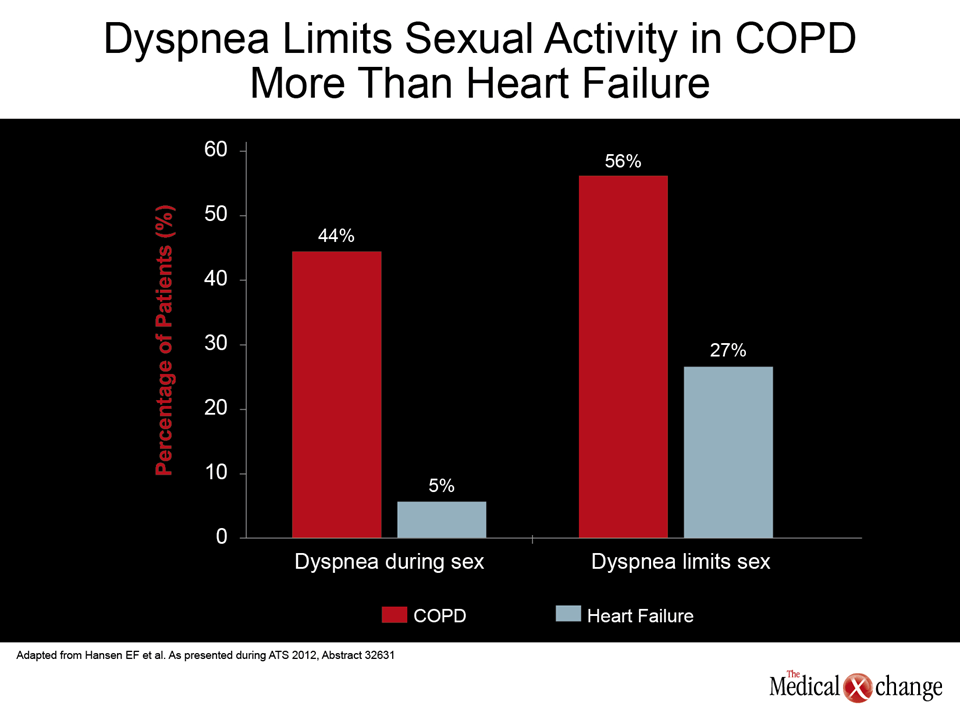
The options for control of dyspnea, the key exercise-limiting COPD symptom, are improving. In the past, bronchodilators for COPD have been drawn from the beta agonist, anticholinergic and methylxanthine drug classes, but new strategies include phosphodiesterase-4 (PDE4) inhibition and agents that combine mechanisms, such as PDE4 inhibition with long-acting beta2 adrenoceptor agonism (LABA). Some of the newer agents have demonstrated both a bronchodilator effect and an anti-inflammatory effect. In measuring COPD treatment efficacy, the traditional endpoint has been exacerbations, because these can be life-threatening and often lead to hospitalization. The growing interest in effect on dyspnea is based on the greater interest in preventing disease progression by allowing patients to optimize physical function. For example, one of the newest medications, roflumilast, was approved for the treatment of COPD in Canada and the United States on the basis of a series of phase III multicenter, placebo-controlled trials showing highly-significant reductions in the risk of exacerbations. At the 2012 ATS meeting, Dr. Rennard pooled data from these studies to demonstrate benefit on dyspnea. On the basis of the relatively rigorous criterion of at least a one unit change in the Transition Dyspnea Index (TDI), the proportion of patients with a clinically-meaningful reduction in dyspnea increased by more than 15% (P=0.0001) on roflumilast, a PDE4 inhibitor, relative to placebo (Fig. 2). “The results were similar for patients with chronic bronchitis or those with chronic bronchitis and a history of exacerbations,” reported Dr. Rennard, whose data include intention-to-treat (ITT) analyses on 5777 randomized patients. The activity of this and other newer agents against dyspnea is drawing attention because of the implications for outcome. More aggressive control of dyspnea is also driving combination studies based on the potential advantage of employing two agents with different mechanisms of action. Such a trial, also presented by Dr. Rennard, tested roflumilast plus tiotropium, an anti-muscarinic agent, in patients with inadequate response to tiotropium alone. After a four-week run-in with tiotropium plus placebo, the patients were randomized to remain on placebo or switch to 500 mcg once daily (QD) roflumilast. Using the same TDI definition as in the pooled analysis, “significantly more patients on roflumilast and tiotropium achieved a clinically-meaningful improvement in dyspnea compared to those on tiotropium and placebo,” Dr. Rennard reported. In this 24-week study of 728 patients, the absolute advantage was 13.07% (54.46% vs. 41.39%; P=0.0009), representing more than a 30% relative gain (Fig. 3). Also important, only 6.69% of those on the combination with roflumilast versus 15.41% on tiotropium plus placebo (P=0.004) had a clinically-meaningful deterioration in TDI score. Combining mechanisms in COPD is attractive. While tiotropium achieves bronchodilation by blocking muscarinic receptors, the gradual improvement in lung function produced by roflumilast is achieved by PDE4 inhibition. In addition, roflumilast appears to exert some direct anti-inflammatory effects, according to new data presented by Dr. Javier Milara, Health Institute Carlos III, Valencia, Spain. This is relevant to dyspnea and exacerbations because of the role that inflammation plays in promoting sputum production, susceptibility to infection, and symptom intensification. In studies conducted in neutrophils cultured from COPD patients, roflumilast was associated with inhibition of interleukin-8 (IL-8) and matrix metallopeptidase-9 (MMP-9) secretion. The same effect was less robust with dexamethasone. “The anti-inflammatory efficacy of glucocorticoids is impaired under oxidative stress conditions, which often occur in COPD. It is perhaps clinically important that we could document an anti-inflammatory effect with roflumilast in neutrophils from both COPD patients and healthy controls,” Dr. Milara reported. Although roflumilast appears to exert some of its control on COPD through direct effects on cAMP in pneumocytes and other lung cells, the anti-inflammatory effect is believed to be the mechanism behind the 17% per year reduction in the exacerbation rate observed in the phase III trials (Lancet 2009;374:685-94). Developing an array of agents that may be used additively or synergistically to control exacerbations and dyspnea in COPD has important implications for outcome, which has drawn attention to new options in clinical testing. Phase III results were presented with NVA237, which is also known as glycopyrronium bromide (GP). In the study, called GLOW2, 1066 COPD patients were randomized to 50 mcg NVA237, placebo, or 18 mcg tiotropium and followed for 52 weeks. On the primary endpoint of significant improvement in lung function as measured with forced expiratory volume in 1 second (FEV1), a significant advantage for NVA237 was observed over placebo at day 1, week 26, and week 52. The advantage of NVA237 on this endpoint was numerically, although not significantly, superior to tiotropium (Fig. 4). “In addition to the improvement in the lung function endpoint, there was a consistent benefit relative to placebo across all of the key indicators of improved COPD control,” reported Dr. Phillip E. Korenblat, Professor, Division of Allergy and Immunology, Washington University School of Medicine, St. Louis, MO. In addition to a significant reduction in the rate of exacerbations (P=0.001) and a significant improvement in quality of life scores (P<0.001), these indicators included a reduction in dyspnea as measured with TDI (P=0.002) (Table 1). NVA237 was also associated with a prolongation of the time to first exacerbation (P=0.001), a reduction in the use of rescue medication (P=0.039), and the percentage of days without symptoms (P<0.05) relative to placebo. Again, although some effects were numerically superior to tiotropium, none were statistically superior. The rate of serious adverse events on NVA237 was actually lower (12.6%) than either placebo (15.4%) or tiotropium (15.0%), although this outcome primarily demonstrates that this bronchodilator, like others, is well tolerated. Although at an earlier stage of development, GS-5759, a bi-functional PDE4 inhibitor and LABA, is also attractive because of dual bronchodilator mechanisms of action and the potential to exert an anti-inflammatory effect. In a study specifically designed to evaluate its anti-inflammatory activity, human peripheral blood mononuclear cells (PBMCs) and neutrophils were stimulated for cytokine release in the absence and presence of this agent, roflumilast, another PDE4 inhibitor known as GSK-256066, and dexamethasone. The 50% inhibitory concentrations (IC50) were consistently superior with this dual mechanism agent than the comparators. “We believe our results demonstrate that GS-5759 has potent anti-inflammatory activity in human PBMCs and neutrophils that is achieved through a combination of both its PDE4 inhibitor effect and its effects on the beta-2 adrenoceptor,” researchers reported here. In the series of studies summarized by researcher Stacey L. Tannheimer, PhD, and others, it was also shown that GS-5759 augments the anti-inflammatory activity of dexamethasone when the two agents were employed together in the experimental model. Agents that can favorably influence the underlying pathophysiology of COPD, which is driven by inflammation, are critical in a transition that will take management from symptom control to disease control. In COPD patients, a comprehensive management strategy is needed because the limitations imposed by the disease, often exacerbated by other co-morbidities, conspire to render patients less active, which in turn contributes to declining exercise capacity. The psychological burden of dyspnea is not the least important adverse influence on disease progression. “Dyspnea at exertion can limit daily activities and increase the risk of poor well-being, social isolation, and depression,” reported Dr. Ejvind Frausing Hansen, Chief Physician, Hvidovre Hospital, Denmark. Providing data demonstrating the effect of dyspnea on sexual activity, Dr. Hansen maintained that control of this symptom is fundamental not only to improve quality of life but for maintaining levels of activity that contribute to health maintenance. In the study presented by Dr. Hansen, 61 patients, of which 39 had COPD and 22 had heart failure, were administered a questionnaire designed to elicit information about troublesome dyspnea during sexual activity. While only 5% of heart failure patients reported dyspnea as a problem during this activity, the rate was 44% (P=0.001) among those with COPD. Of those who reported dyspnea during sex, 56% of COPD patients, versus 27% of heart failure patients (P=0.04), described it as a limiting factor. A higher proportion of COPD patients than heart failure patients described their sexual life as inadequate (38% vs. 32%), but the difference was not significant (Fig. 5). “An adequate sexual life is also important for elderly people and is an important aspect of a sense of wellbeing,” Dr. Hansen commented. He suggested that control of dyspnea to improve sexual function deserves more attention but is part of a comprehensive approach to sustain participation of COPD patients in a full array of activities that define an adequate quality of life.
Conclusion
Treating the symptoms of COPD is important for preserving quality of life in this progressive condition, but there is increasing attention to the relevance of symptom control to preservation of pulmonary function and exercise levels. The limitation on activity imposed by COPD symptoms can create a vicious cycle of declining exercise capacity that increases the risk of exacerbations and accelerates functional impairment. Agents that can control dyspnea have the potential to improve functional capacity to slow or prevent the decline in physical wellbeing that underlies greater vulnerability to exacerbations, hospitalizations, and death. Use of agents that improve dyspnea through bronchodilation, anti-inflammatory effects, or other actions may improve outcomes at the same time that it preserves quality of life.