Diabetes
American Diabetes Association (ADA) 72nd Annual Scientific Sessions
Glucose Profiles and Cardiovascular Outcomes Improved by Newer Bile Acid Sequestrant in Type 2 Diabetes
Philadelphia – Among two studies in type 2 diabetes mellitus (T2DM) on patients receiving a bile acid sequestrant (BAS), presented at this year’s American Diabetes Association (ADA) 72nd Annual Scientific Sessions, one demonstrated benefits in both prandial and glucose profiles while the other showed improved cardiovascular outcomes in patients with high medication adherence.
Diabetes, metabolic syndrome and obesity are each independently associated with increases in cardiovascular events. Separate research presented at this year’s ADA meeting looked into the effect of colesevelam on diurnal glucose patterns, and into its effects on cardiovascular outcomes.
In addition to its lipid-lowering properties, the bile acid sequestrant (BAS) colesevelam is known to lower blood glucose as measured by HbA1c. But because HbA1c is a “gross” measure, said the author of the first study, Dr. Roger Mazze, Clinical Professor, University of Minnesota Medical School and Chief Academic Officer, International Diabetes Center (IDC), MN, questions about how colesevelam lowers glucose, how quickly it does so and whether or not it lowers overnight or postprandial glucose have remained unanswered. The advent of continuous glucose monitoring (CGM), however, now allows aspects of these questions to be addressed.
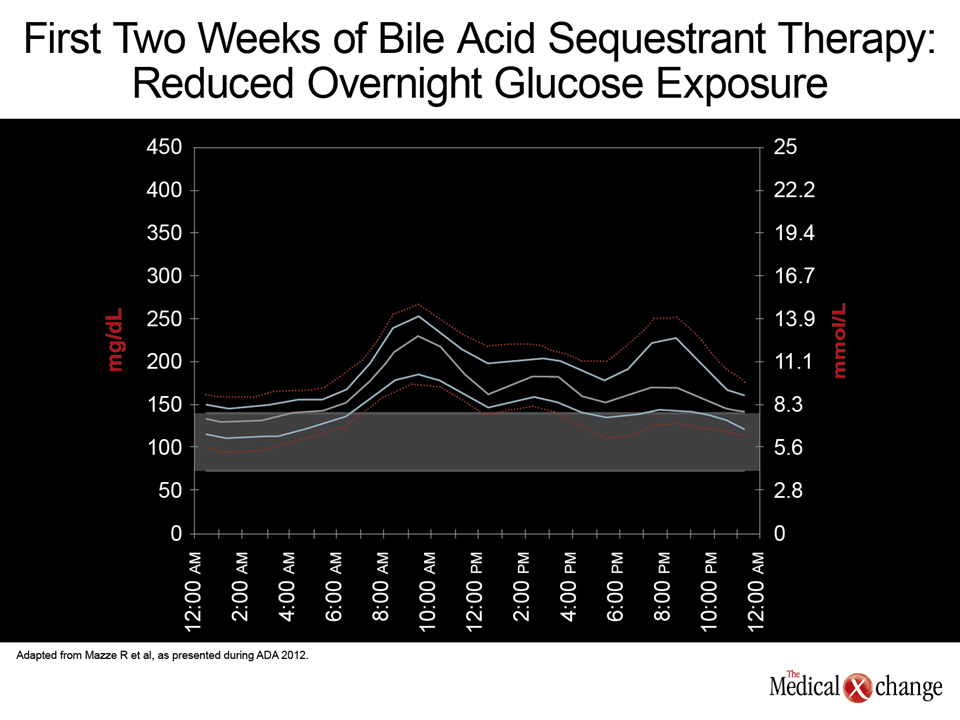
In a prospective, 12-week cross-over, double-blind, placebo-controlled study, Dr. Mazze and colleagues used CGM and ambulatory glucose profile (AGP) analysis to determine to what degree colesevelam restores normal diurnal glucose patterns in 21 type 2 diabetes patients treated with metformin, sulfonylurea, or a combination of the two. After two weeks of baseline monitoring, patients received colesevelam or placebo for 12 weeks before crossing over for another 12 weeks.
Dr. Mazze and the IDC in Minneapolis, MN developed the software that generates an AGP in the form of a visual report for the clinician that provides a comprehensive view of the patient’s changing glucose levels over the period during which the CGM device is worn. That report allows clinicians to see patterns and adjust therapy accordingly.
In one example from this study, a 47-year old female with normal glucose tolerance was compared to an age- and sex-matched patient with type 2 diabetes; both were treated with metformin for 28 days. The AGP for the diabetic patient showed a persistent post-prandial rise in mean blood glucose, with an 80% excess in glucose exposure compared with the reference normal case. It also showed threefold greater glucose variability (interquartile range) than the normal case. Glucose variability has been shown to increase risks and severity of coronary artery disease.
The study analysis showed a significant difference in HbA1c levels (-0.6%) between the end of the placebo periods and the end of the colesevelam periods (P<0.0001). During the same period, LDL cholesterol decreased significantly in the colesevelam group (-21.4 mg/dL, P=0.0007).
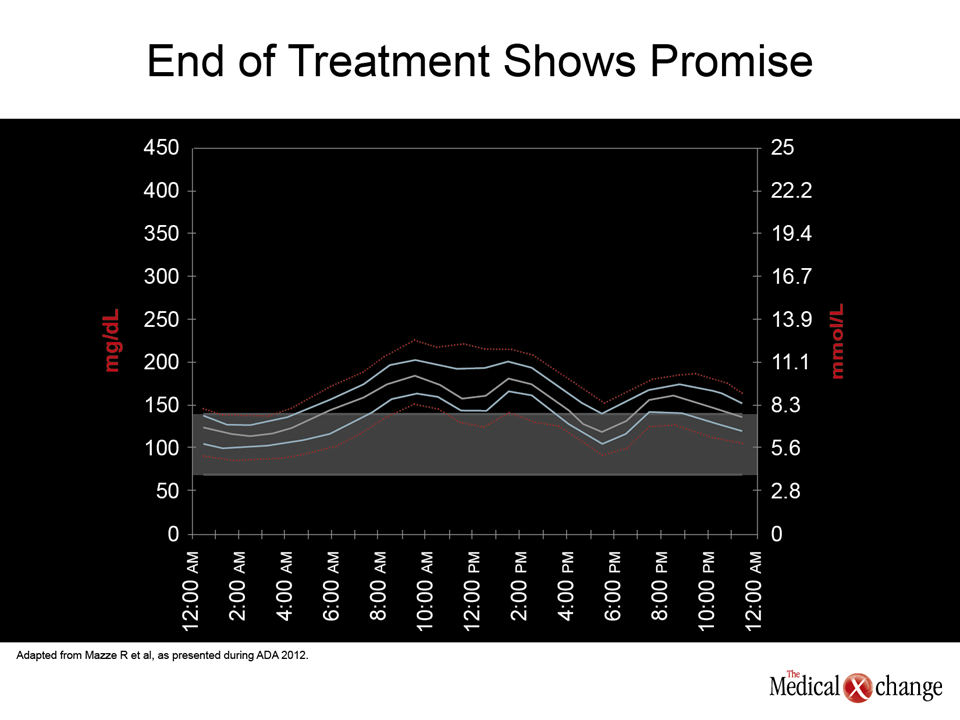
Figures 1A (Fig. 1A) & 1B (Fig. 1B) show a representative patient at the start and end of colesevelam treatment, with the latter revealing a narrowing of the profile towards normal and a dampening of the postprandial rise in glucose. Hypoglycemia was not reported, and weight remained the same.
“It is a very good drug for this population because unlike statins, it does not raise glucose. Depending on glucose levels when you start, you may not have to use other glucose-lowering medications. You are lowering glucose variability, which is very important—and you are lowering lipids at the same time,” Dr. Mazze said. Compliance with medications over the half-year study was excellent despite the relatively high colesevelam dose (6 pills), Dr. Mazze commented.
The significance of this favorable adherence to colesevelam therapy was underscored by Dr. Xin Ye, Director, Health Economics and Outcomes Research, Daiichi Sankyo, who noted that medication adherence is a challenge in chronic disease management, and non-adherence may lead to patients not receiving the full advantages of medications.
Dr. Ye presented an analysis of one of the largest US claims databases, the MarketScan® Commercial Claims and Encounters and Medicare Supplemental Databases, which includes more than 20 million individuals annually with approximately 100 payers. The aim was to examine the association between adherence to colesevelam and the risk of major cardiovascular events (acute myocardial infarction [AMI] and stroke) in type 2 diabetes mellitus (T2DM) patients.
Subjects (mean age ~60 years) were stratified according to colesevelam adherence levels, with high adherence defined as a medication possession ratio (MPR) during a designated 1-year period of ≥0.8 (n=2405), medium adherence as 0.5≤ MPR <0.8 (n=1930), and low adherence as MPR <0.5 (n=7845). The study outcome was time to first hospitalization with a primary diagnosis of AMI or stroke.
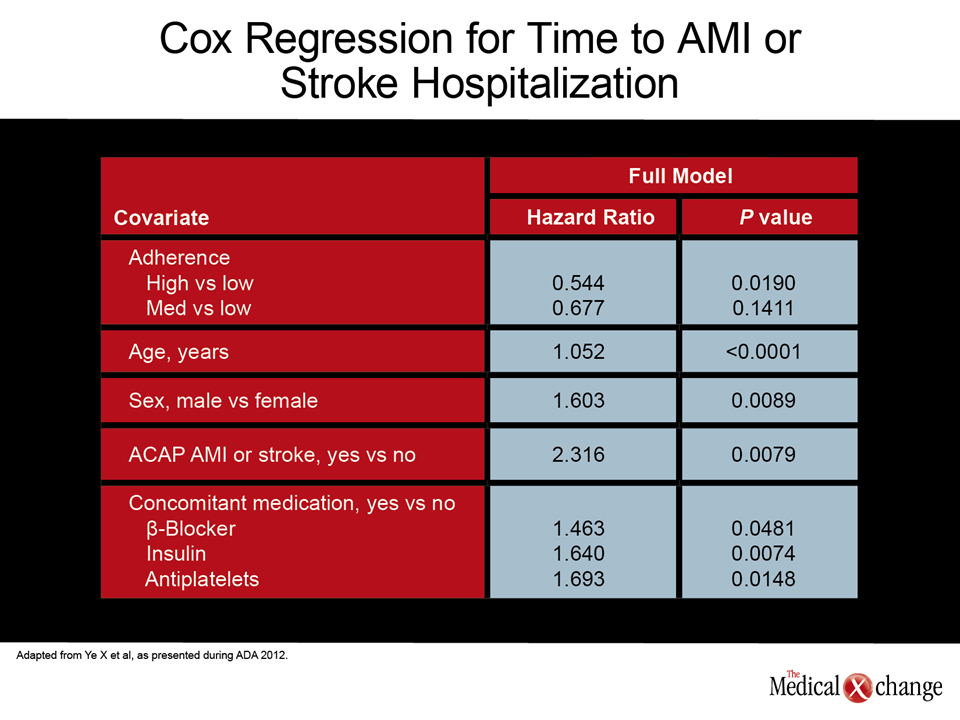
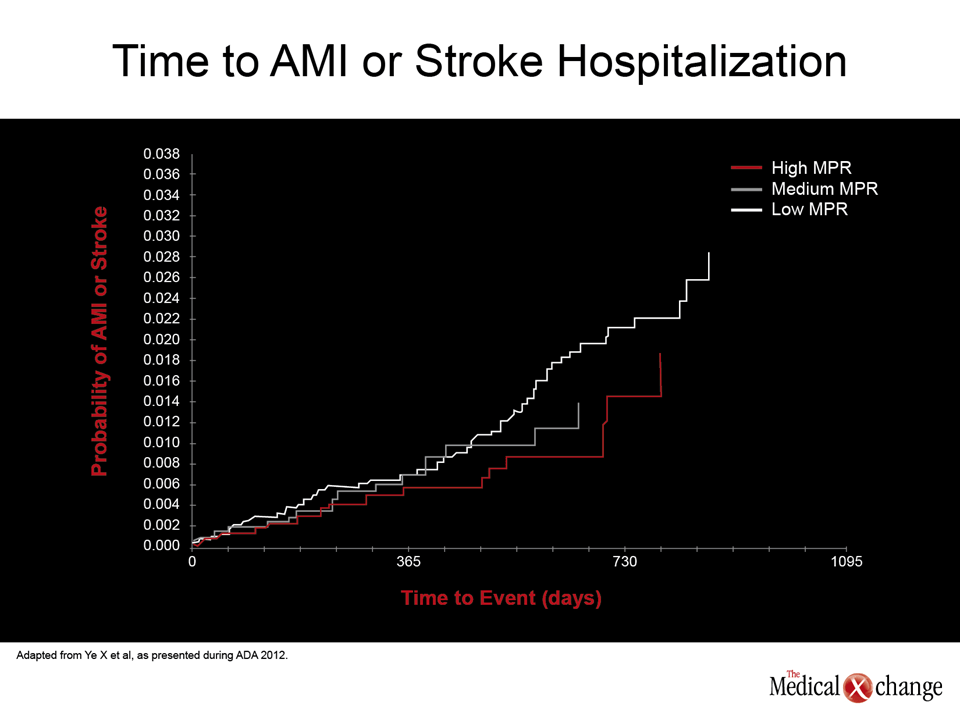
After adjusting for baseline characteristics, Dr. Ye found that patients with higher colesevelam adherence as compared to low colesevelam adherence had nearly a 46% lower risk of hospitalizations for AMI or stroke (HR=0.544, P=0.0190) (Fig. 2). There were reductions in AMI and stroke risk for medium versus low adherence, but they were not statistically significant (HR=0.6776, P=0.1411). “You see a very nice response curve,” Dr. Ye commented (Fig. 3).
Other factors conferring significantly higher AMI or stroke hospitalization risk were older age, male sex, and concomitant beta-blocker, insulin or antiplatelet medication. Dr. Ye concluded, “This finding suggests that interventions to improve adherence to colesevelam in the patients with suboptimal adherence may have long-term cardiovascular benefits.”
Session moderator Craig D. Williams, PharmD, Clinical Associate Professor of Pharmacy Practice, College of Pharmacy Oregon State University and Oregon Health & Science University, asked, “There have been a number of trials showing that compliance is a surrogate for healthy lifestyle behavior – and often good compliance to placebo in the cardiac literature is more important than poor compliance to the active drug. Would you speculate on how much of this benefit is coming from the drug itself versus its being a marker for healthy lifestyle behavior among these patients?” Dr. Ye, after pointing out that the database does not allow assessment of lifestyle factors, responded, “Because of the nice dose response, I think there is a significant drug effect.”
Conclusion
Dr. Ye’s analysis showing reduced AMI and stroke in patients with high adherence to colesevelam therapy suggests that the improved glucose profiles demonstrated with colesevelam in Dr. Mazze’s study can lead to clinically meaningful benefits.