Neurology
Alzheimer’s Association International Conference 2012 (AAIC)
Latest Alzheimer’s Disease Diagnostic Criteria and Guidelines Show Importance of New Screening Tools to Detect Key Biomarkers
Vancouver – In 2011, The US National Institute on Aging (NIA) together with the Alzheimer’s Association (AA) established new Alzheimer’s disease (AD) spectrum diagnostic guidelines. The new classifications of the disease include a preclinical phase and illness in patients with mild cognitive impairment (MCI). They reflect a movement within the field of AD research to detect and treat the disease even before a person demonstrates outward symptoms. Consequently, the development of screening tools that will enable clinicians to detect key biomarkers for AD, specifically the presence of amyloid biomarkers and the Apolipoprotein E4 (APOE-e4) allele, as early indicators of cognitive decline, is yielding extremely promising results, and contributing to the validation of these new guidelines.
During this year’s Alzheimer’s Association International Conference (AAIC) a key theme emerged, that of screening for early detection in presymptomatic and healthy adults and in people with mild cognitive impairment (MCI). This research focus is supported by the recent reclassification of Alzheimer’s disease (AD) as a spectrum disease to include a preclinical phase, which is based on the presence of abnormal beta amyloid biomarkers.
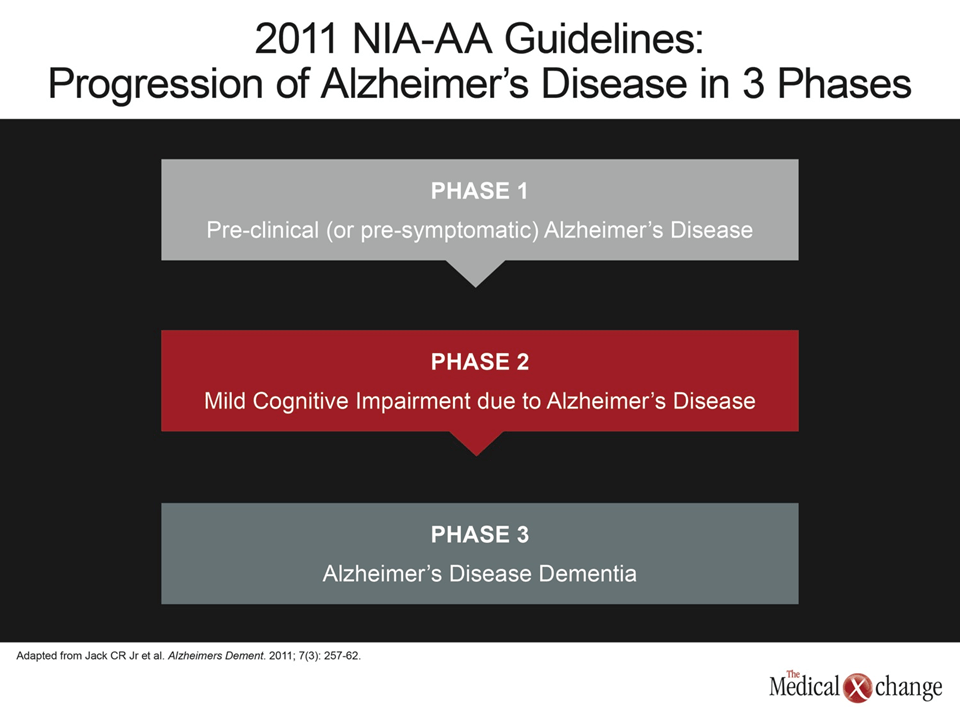
In April 2011, the US National Institute on Aging (NIA), together with the Alzheimer’s Association (AA), published new criteria and guidelines for the diagnosis of AD. These guidelines separate the progression of Alzheimer’s into three phases, namely: (1) preclinical (presymptomatic), (2) MCI due to AD, and (3) AD dementia (Fig. 1).
The first and second phases of the proposed guidelines are described by the NIA as research criteria in need of validation, and evidence of significant progress in this direction was abundant at the conference, with a specific focus on imaging for detection of beta amyloid biomarkers and neurodegeneration, and cognitive testing.
Validating Preclinical AD: The Relationship between AD and Neurocognitive Decline
Researchers at the Mayo Clinic presented compelling supportive data for the NIA-AA preclinical diagnostic criteria from a study of 443 participants enrolled in the larger Mayo Clinic Study of Aging (MCSA).
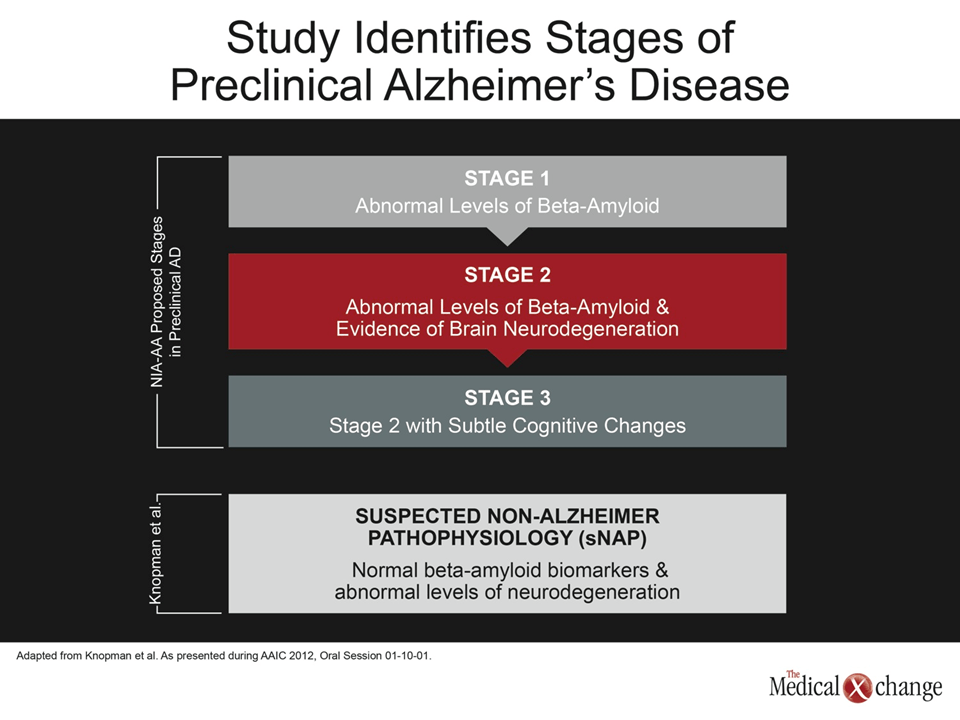
The three stages of preclinical AD defined in the NIA-AA guidelines are abnormal levels of beta-amyloid (stage 1); abnormal levels of beta-amyloid and evidence of brain neurodegeneration (stage 2); and stage 2 with subtle cognitive changes (stage 3) (Fig. 2). The Mayo Clinic investigators stratified participants into these stages, in addition to a suspected non-Alzheimer pathophysiology (sNAP) group, consisting of people with normal beta-amyloid biomarkers but abnormal levels of neurodegeneration. Participants were evaluated for biomarkers using MRI scans, 18-Fluorodeoxyglucose (FDG) PET scans, and amyloid imaging using C11 Pittsburgh Compound B (PiB) PET Scans. The investigators compared the differences in outcomes in cognitively normal people, according to their biomarker profile.
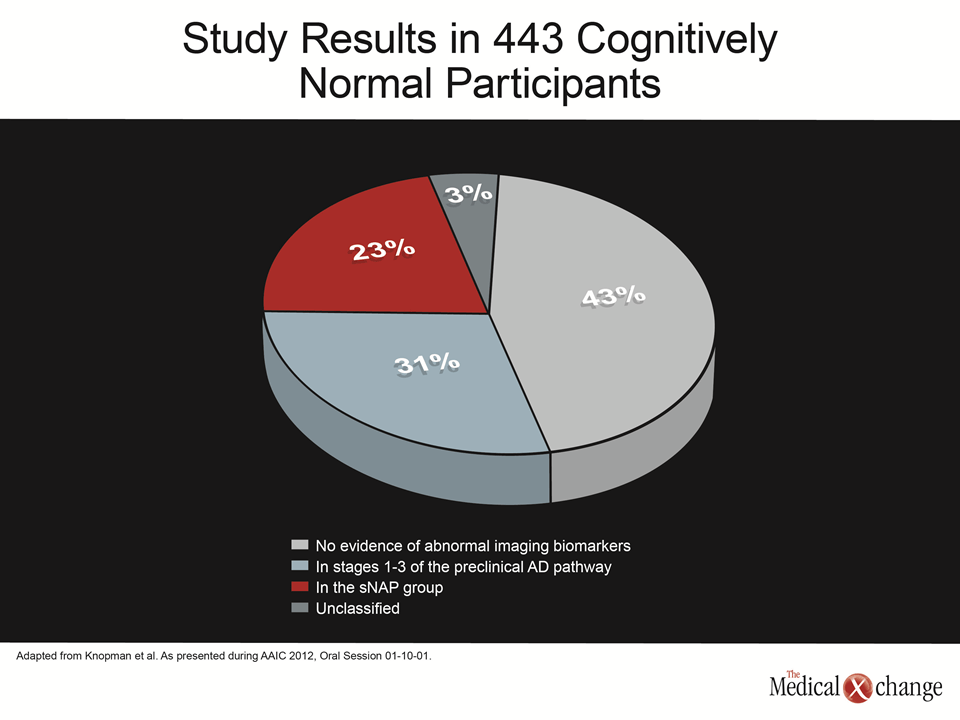
The data showed that of the 443 cognitively normal participants, 189 (43%) had no evidence of abnormal imaging biomarkers, while 137 (31%) fell into stages 1-3 of the preclinical AD pathway, 102 (23%) were in the sNAP group and 15 (3%) were unclassified (Fig. 3).
Not surprisingly, those in preclinical AD pathway stages 1-3 were significantly more likely to progress to cognitive impairment than the biomarker negative group (P<0.001). In contrast, the sNAP group showed no evidence of higher levels of white matter hyperintensity, or cortical or subcortical infarcts compared with preclinical AD stage 1-2 participants. Additionally, the AD preclinical stage 2-3 groups were more likely to progress than the sNAP group (P=0.04). On further investigation, the researchers found that the sNAP and AD preclinical stages 2-3 groups were similar except for one factor – the sNAP group had a lower proportion of Apolipoprotein E4 (APOE-e4) carriers.
“Abnormal beta-amyloid imaging with neurodegeneration carried a higher risk for cognitive decline than neurodegeneration alone,” noted Dr. David Knopman, Department of Neurology, Mayo Alzheimer’s Disease Research Center (ADRC), Rochester, MN, and lead study investigator. These results provide evidence that the NIA-AA preclinical AD criteria identify a group of cognitively normal persons at risk for cognitive decline, he said.
Cognitive Testing
Further compelling data showing the association between beta-amyloid burden and cognitive impairment in normal older adults were presented by Yen Ying Lim, PhD student, University of Melbourne, Australia. The results showed that healthy older adults who had increased beta-amyloid in their brains demonstrated a decline in memory over 18 months, despite being completely normal on conventional neuropsychological assessment. “These results suggest that monitoring for changes in individual memory on the basis of repeated assessment will be useful for identifying very early AD,” said Ms. Lim.
The prospective study used APOE-e4 genotyping and PET neuroimaging for baseline detection of cerebral beta-amyloid load using PiB in 141 participants in the Australian Imaging, Biomarkers and Lifestyle (AIBL) study. The participants completed the CogState Brief Battery, and extensive neuropsychological, medical and lifestyle assessments at baseline and 18 months.
Linear mixed model analyses, adjusting for baseline performance levels, indicated a significant worsening in cognitive function from baseline in healthy older adults with abnormal levels of PiB at 18 months. When the model included APOE-e4 status the results remained the same. However, in the visual memory task with healthy older APOE-e4 carriers, the performance was worse compared with non-carriers. The data suggest that an elevated beta-amyloid load is associated with faster cognitive decline, particularly in measures of visual and verbal memory.
A second study using the CogState Brief Battery in another subset of AIBL participantsshowed that in healthy people with the APOE-e4 allele, memory abilities are associated with the level of beta-amyloid in the brain.
The study evaluated relationships between cerebral beta-amyloid burden, episodic memory, attention and psychomotor function and clinical ratings in 144 healthy older adults, 30 older adults with MCI and 20 adults with AD who had undergone amyloid neuroimaging using PiB and APOE-e4 genotyping.
The results showed that within each clinical classification there was an association between cerebral beta-amyloid burden and episodic memory in the MCI group, and similar but weaker relationships in the healthy older adults. In healthy older APOE-e4 carriers, relationships between cerebral beta-amyloid and episodic memory were stronger compared with non-carriers. No relationships were evident in the AD group.
“The finding of a relationship between brain amyloid levels and memory suggests that very subtle changes in memory are associated with radiological markers of AD pathology; collected from brain scanning, only in people who are already at some increased risk of disease,” said lead author of the study, Dr. Paul Maruff, Professor, Mental Health Research Institute of Victoria, University of Melbourne, Australia.
“These findings point the way to a protocol for the early identification of AD by combining objective assessment of memory, using a system like the CogState system, a marker of an individual’s genetic risk for AD, determined from blood and brain scanning with a compound that can detect amyloid in the brain,” he said. “The CogState brief battery is highly sensitive to changes in the brain that are related to AD even in people who are completely healthy.”
MCI Criteria applied AD Spectrum Diagnosis
The proposed NIA-AA diagnostic guidelines for MCI due to AD involve three levels of certainty; uninformative, intermediate, and highest. These are ordered according to the availability of biomarkers, and are in the process of being validated in the general population. To that end, Dr. Ronald Petersen, MCSA principal investigator and Director of the Mayo ADRC, Rochester, MN, and colleagues evaluated these criteria in 156 participants (mean age 82 years) in the MCSA who were diagnosed with MCI. Participants underwent 3T MRI, FDG PET and PiB PET scans at diagnosis of MCI. Notably, imaging was done without knowledge of the clinical diagnosis. Participants were subsequently classified as normal or abnormal on indices of amyloid deposition by PiB PET and neurodegeneration using MRI hippocampal volume and FDG PET.
The results showed that 12% had evidence of the presence of amyloid on PiB scans but no other signs of neurodegeneration. However, 55% had evidence of both amyloid deposition on PiB, and either atrophy on MRI or on FDG PET indicative of hypometabolism, or both. Not surprisingly, the frequency of APOE-e4 carrier status was highly correlated with the presence of beta-amyloid.
“These results indicate that the new diagnostic criteria for MCI due to Alzheimer’s work quite well,” said Dr. Petersen. “Sixty-seven percent of the participants had evidence for either amyloid deposition or amyloid plus a marker for neurodegeneration. As such, two thirds of the participants were thought to be highly likely to develop the dementia due to Alzheimer’s.”
Decline Observed in AD is Gradual: Sub-study Results
In addition to being able to detect those likely to progress to Alzheimer’s dementia, determining the rate at which the disease progresses and factors that may influence that progression over the short-term—3 to 6 months—would inform clinical trials for new treatment modalities in preclinical and MCI populations. Data from the AIBL-Rate of Change Sub-Study (ROCS) showed that it is possible to monitor memory and other aspects of thinking such as attention and working memory in people who are healthy, who have mild cognitive impairment and in those with AD.
The study evaluated 205 participants from AIBL consisting of 64 healthy older adults; 51 adults with subjective memory impairment (SMI); 48 adults with MCI; and 42 adults with AD. Each participant underwent a 20-minute CogState computerized battery on a monthly basis for 3 months. The battery included measures of verbal learning, processing speed, attention, visual episodic memory, visual recognition learning, working memory, and verbal episodic memory.
Dr. Maruff further noted: “as expected, performance on the very brief battery was different between the groups, with the AD group showing a large impairment on the tests of memory and attention and the MCI group showing moderate levels of impairment the memory test.
However, even when given these same tests multiple times over very short time intervals, for example four times over three months, performance did not change in any of the groups. Furthermore, the measures of stability were equivalent between the healthy, mild cognitive impairment and AD groups.
These data suggest that as an instrument for measuring cognitive status in the clinic, the CogState Brief Battery can be applied repeatedly without loss of sensitivity and that this application is appropriate for use in healthy people and in people who have dementia. Thus clinicians will not need to use different assessment tools for the different patient groups.”
Conclusion
The results presented here are promising, and will expand the clinical tools available for the detection and treatment of AD. As is evident in cardiovascular disease, the importance of early identification of high-risk individuals cannot be understated, and will provide the opportunity for early and possible preventative interventions for AD, thereby improving the quality of life for the person, their families and health care providers alike.