Multiple Sclerosis
28th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS)
Safety Data for Established and Newer Disease-Modifying Therapies in Multiple Sclerosis: Key Data from ECTRIMS
Lyon – New data confirm the importance of periodically recalculating the risk-to-benefit ratio of disease-modifying therapies (DMTs) for multiple sclerosis (MS). For the newer oral and injectable agents, the ultimate safety will not be fully understood until the risk of late adverse effects from altered immune function or unexpected organ toxicities can be fully quantified over lengthy follow-up. For the established injectable DMTs, data now being collected in populations not well represented in the registration trials, such as adolescents and pregnant women, are providing a broader perspective on where these treatments fit. Safety data relevant to both types of risk calculations were presented at the 2012 ECTRIMS.
An accurate calculation of the benefit-to-risk ratio of newer therapies, including oral agents, is dependent on a large database of safety data collected over several years, according to Dr. Xavier Montalban, Director, Multiple Sclerosis Center of Catalonia, Barcelona, Spain. Referring to fingolimod, the only oral therapy approved so far for use in Canada, and teriflunomide, which is now available in the United States, Dr. Montalban reiterated a common perspective that “the new therapies will have both known and unforeseen complications” that cannot be fully appreciated until the long-term data are available.
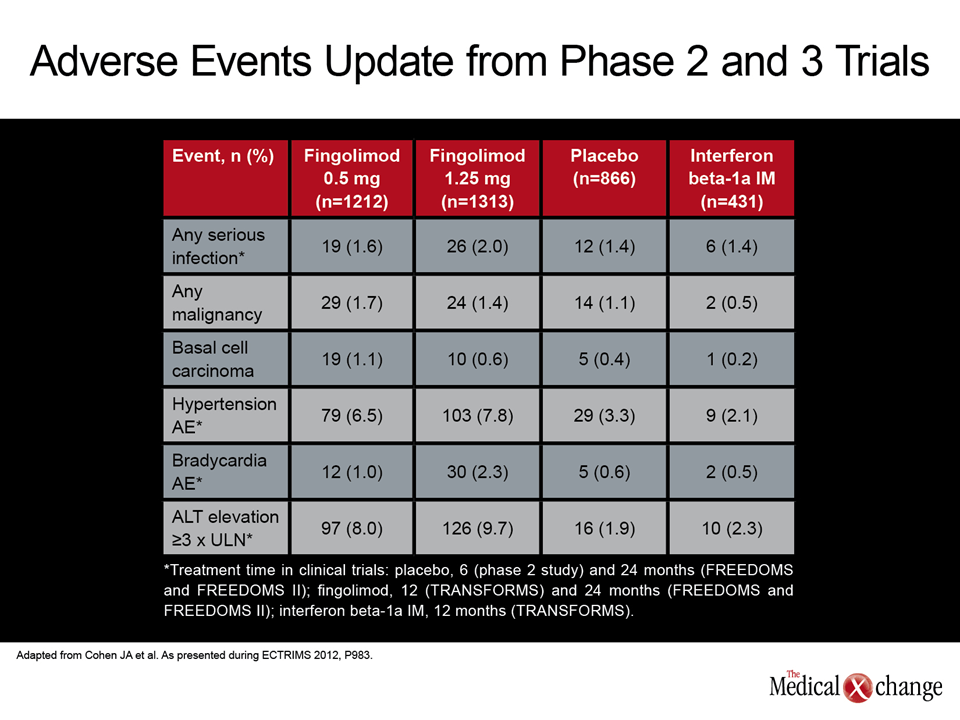
Fingolimod safety data updated at ECTRIMS provide an example. In a presentation by Dr. Jeffrey A. Cohen, Cleveland Clinic Foundation, that collated all the safety data collected in phase 2 and phase 3 studies, as well as extensions, an initial signal of increased risk of basal cell carcinoma reported previously has faded but the degree of increased risk of hypertension and liver enzyme elevations is now better described. In regard to altered immune function, no signal has been observed for risk of serious infections or malignancy in any form (Table 1).
Different Mechanisms of Action in Newer Agents
The types of risks associated with other newer agents are likely to differ because of different mechanisms of action. This is exemplified in the new phase III data with teriflunomide. Presented at this year’s ECTRIMS by Dr. Ludwig Kappos, University of Basel, Switzerland, the protection against relapse was on the order of that associated with other disease-modifying therapies (DMTs), but the side effect profile of this oral agent was relatively unique. While it is difficult to interpret the higher discontinuation rate on teriflunomide than fingolimod when drawn from different data sets (8.3% on the highest dose of fingolimod in the Cohen presentation and 15.6% on the highest dose of teriflunomide in the Kappos data), several side effects not associated with fingolimod, such as alopecia and diarrhea, occurred at a higher rate on teriflunomide relative to placebo.
Safety data presented at ECTRIMS for the broad array of other agents in development, such as the oral drug BG-12 and the injectable monoclonal antibodies alemtuzumab and daclizumab, associate each with a unique acute safety profile. Specifically, alemtuzumab has been associated with an increased risk of thyroid dysfunction and immune thrombocytopenic purpura (ITP), while daclizumab, in newly-presented data from an extension of the phase II SELECT study, called SELECTION, has been linked to serious infections, serious skin reactions and autoimmune complications, including one death from autoimmune hepatitis. These findings reinforce the principle that each immune-modulating therapy has the potential to pose very different long-term risks. Again, due to unknown long-term safety, the benefit-to-risk ratio of these newer other options cannot be fully understood until longer follow-up is available.
Established Agents Offer Perspective in Special Populations
In contrast, more than a decade of clinical use with the established injectable agents permits a relatively precise understanding of benefits in the context of risk. Due to the large experience with these drugs, safety data is now accumulating in special populations, such as pregnant women, pediatric patients, and patients with co-morbidities. In data presented at ECTRIMS from the Avonex Pregnancy Exposure Registry, which has follow-up data on 311 prospectively enrolled women treated with this IFNβ-1a agent, the spontaneous abortion rate of 10.5% was slightly lower than the expected rate of 15%, while the 5.6% rate of birth defects and the types of birth defects also provided no signals for concern.
In a study led by Dr. Aaron E. Miller, Mount Sinai School of Medicine, New York City, of 44 women contemplating pregnancy, 28 opted to remain on therapy. Of the 34 completed pregnancies in these women, 28 were full term with normal children. There were three spontaneous abortions, one ectopic pregnancy, and two pregnancies terminated for Trisomy 21 fetuses not considered related to glatiramer acetate (GA). Overall, the results support the safety of GA in pregnancy even though the authors emphasized that a larger data pool is needed.
In children and adolescents with MS, a safety analysis of the use of IFNβ-1a drawn from the REPLAY study, which involves a retrospective analysis of safety and efficacy from this agent as captured in medical records, was also reassuring. Presented by Dr. Angelo Ghezzi, Ospedale di Gallarate, Italy, the study evaluated adverse events overall and adverse events stratified by age below 12 years and ages 12 to 18 years in 307 patients receiving adult doses. Overall, while there were serious adverse events considered to be related to IFNβ-1a, such as injection-site injuries and abnormal liver function tests, the incidence was comparable to that reported in adults, and there were no significant differences between those less than 12 years of age and those older.
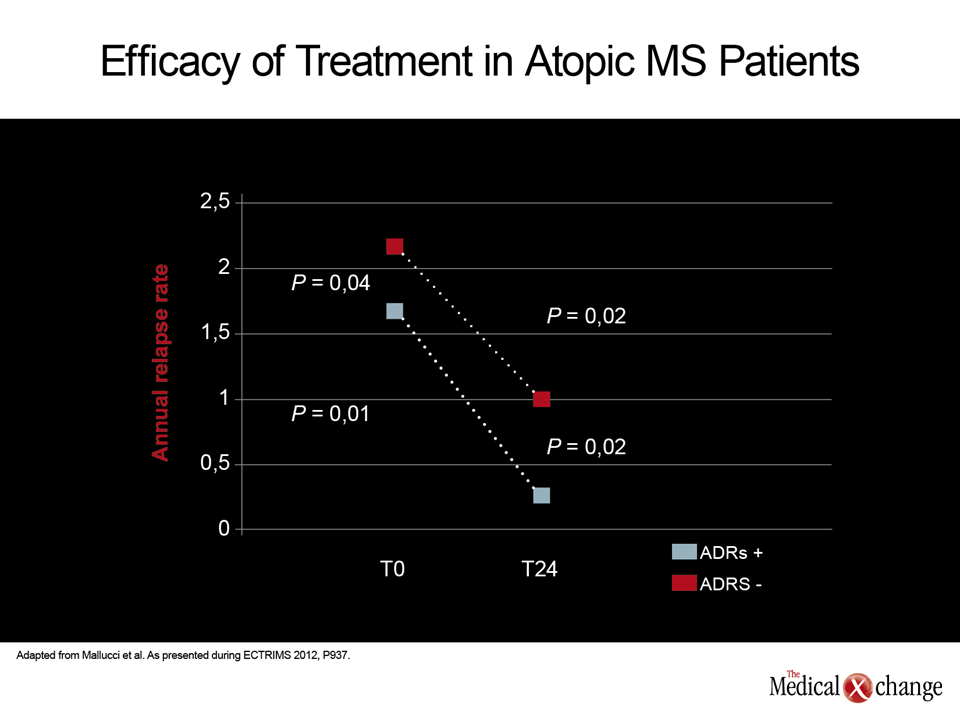
In the administration of immune-modulating therapies for MS, one concern has been exacerbating other immune-related disorders, but an intriguing study suggests that the mechanism of GA, which is believed to promote a shift from a Th1 to a Th2 response, may actually be of benefit when MS patients have an allergic respiratory disease (ARD). In a prospective, multicenter study that followed 27 patients with ARD and 28 patients without ARD who were initiated on GA, both groups achieved a significant reduction in the annualized relapse rate, but the benefit was significantly greater in those with ARD (Fig. 1). According to Dr. Roberto Bergamaschi, Neurological Institute C. Mondino, Pavia, Italy, this relative protection is not only potentially relevant to treatment of atopic patients but provides support for one of the purported mechanisms of GA.