cardiology
2012 Scientific Sessions of the American Heart Association (AHA)
Interrelationship of Lipid and Glucose Metabolism Disorders Exemplified in Agents that Favorably Influence Both
Los Angeles – In patients with dyslipidemia and impaired fasting glucose (IFG), newly-presented data demonstrate that adding a bile acid sequestrant into the treatment mix will address both metabolic disorders simultaneously. The results of the randomized placebo-controlled trial, presented at the 2012 AHA, contribute significantly to cardiovascular (CV) risk management because of the frequency with which hyperlipidemia and impaired glucose metabolism co-exist. The growing population of individuals in Canada who require treatment of multiple CV risks, best illustrated by the epidemic of metabolic syndrome that is accompanying rising rates of obesity, has led to complicated risk management schemes that may be simplified by using therapies with multiple favorable effects. In the study, the addition of a bile acid sequestrant was well tolerated and accepted by patients.
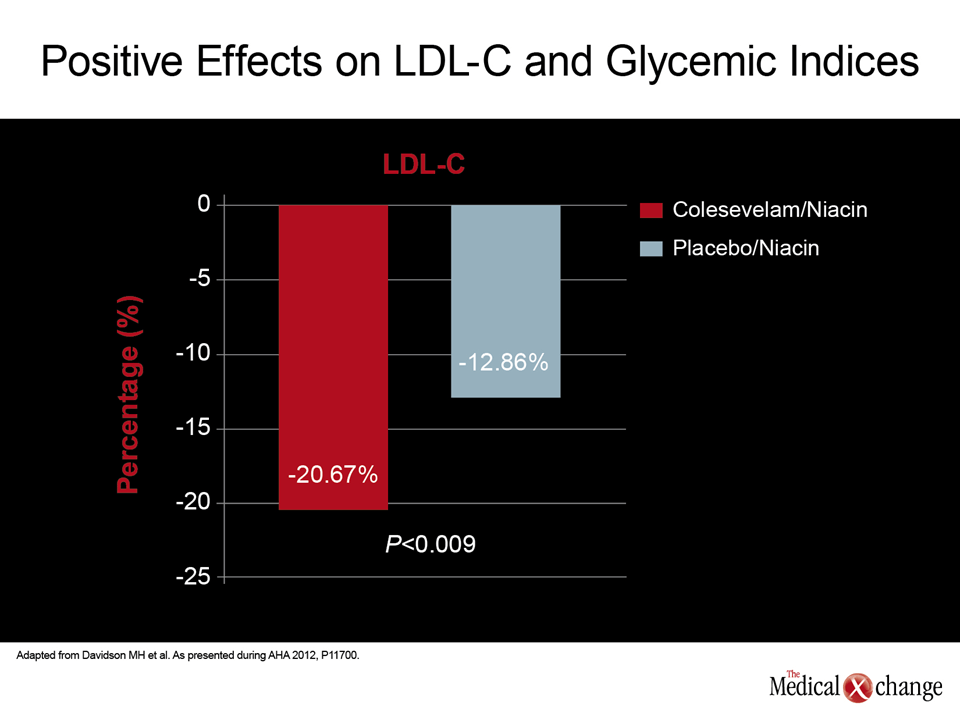
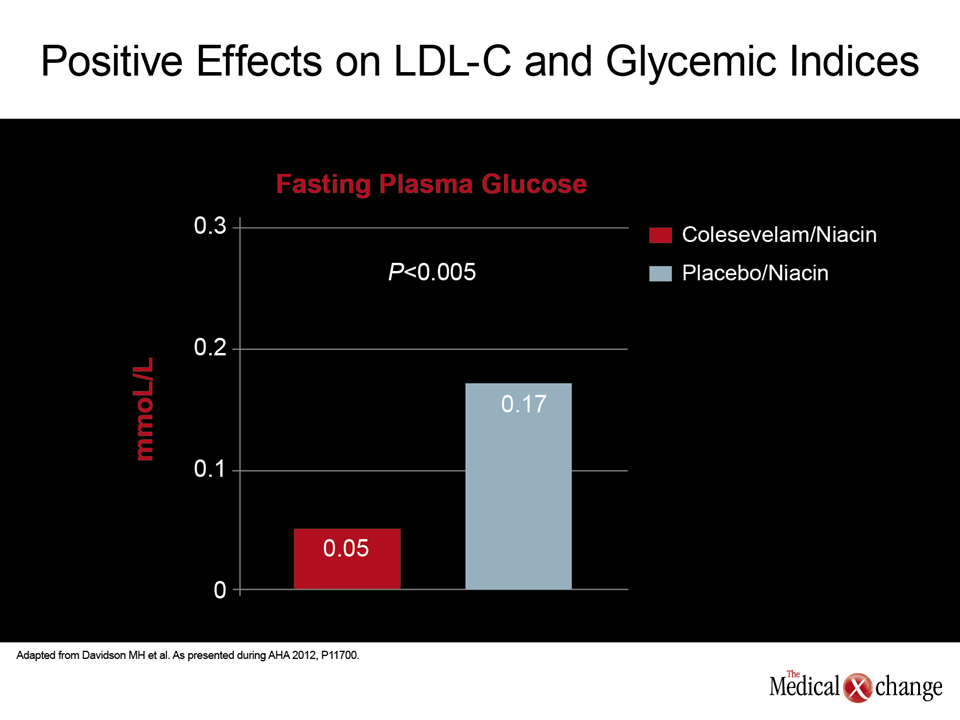
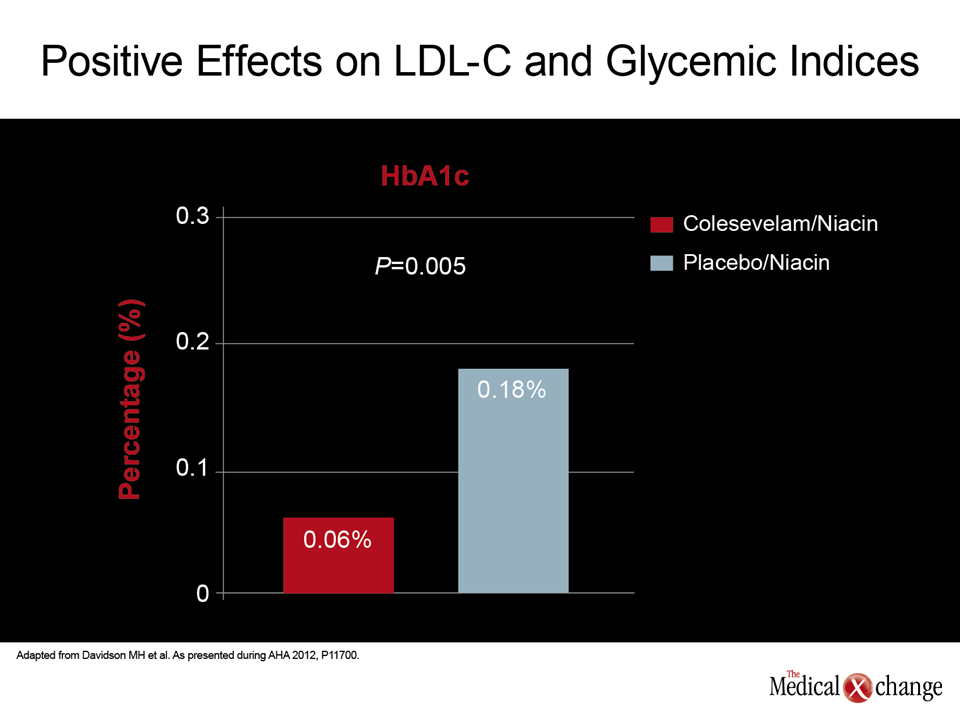
Managing cardiovascular (CV) risk is becoming more challenging because of the complex metabolic disorders generated by rising levels of body weight. Risk factors such as hyperlipidemia, hypertension, and impaired glucose metabolism now typically track together as lifestyle choices have led to less physical activity, higher consumption of fatty foods, and greater visceral fat. The newly-reported efficacy of a bile acid sequestrant in treating both lipid and glucose metabolic disturbances reinforces the interrelationship of these risk factors. According to data from this study, which evaluated the bile acid sequestrant colesevelam, “there were clinically meaningful improvements in both low-density lipoprotein cholesterol (LDL-C), and glucose indices” when this bile acid sequestrant plus niacin was compared to niacin alone, reported the senior author Dr. Michael H. Davidson, Director of Preventive Cardiology, University of Chicago, Illinois. Citing previous studies that have associated colesevelam with significant improvements in glycemic control, including those conducted in patients with type 2 diabetes mellitus (DM2), Dr. Davidson suggested that the study strategy is relevant to routine care of patients with both elevated LDL-C and impaired fasting glucose (IFG), which is a common circumstance. In this study, 140 patients with a non-high-density lipoprotein cholesterol (HDL-C) of 2.5 mmol/L and a fasting plasma glucose (FPG) of at least 2.3 mmol/L were randomized to receive the standard dose of colesevelam (3750 mg/day) with niacin titration or placebo with niacin titration. The titration scheme for niacin was an initial dose of 500 mg/day increased incrementally to a maximum dose of 2000 mg/day as tolerated. All patients also received one enteric-coated aspirin tablet daily. The primary outcome at the end of 12 weeks was change in lipid and glycemic levels. Safety was also monitored. At the end of study, LDL-C fell on average by 20.67% in the arm receiving colesevelam plus niacin versus 12.86% in those patients randomized to niacin plus placebo (P<0.009). While FPG rose on average by 0.17 mmol/L in the group that received niacin with placebo, the average increase was only 0.05 mmol/L in the group that received colesevelam (P<0.005). Similarly, there was only a 0.06% increase in hemoglobin A1c (HbA1c) level for those on colesevelam versus 0.18% (P=0.005) in the group randomized to placebo (Fig. 1) (3 parts).
The take home message from this study is that clinicians “should consider adding colesevelam to niacin therapy if additional LDL-C lowering is indicated – especially if the glucose is elevated.”
“The study demonstrated that adding colesevelam improved the adverse effects of niacin on glucose levels while providing meaningful additivity to LDL-C reduction,” Dr. Davidson reported. The take home message from this study is that clinicians “should consider adding colesevelam to niacin therapy if additional LDL-C lowering is indicated – especially if the glucose is elevated.” Bile acid sequestrants were the first class of lipid-lowering therapy licensed for reducing CV events, a benefit demonstrated in a landmark trial called the Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT) which compared the bile acid sequestrant cholestyramine to placebo. Compared to placebo, the bile acid sequestrant produced an average 20.3% reduction in LDL-C reduction and a 19% reduction in the risk of fatal and non-fatal myocardial infarctions (MI). Cholestyramine was subsequently relegated to adjunctive LDL-C lowering with the introduction of statins. Statins provided greater lipid lowering without the gastrointestinal (GI) side effects associated with cholestyramine.
Tolerability and Safety Profile
Colesevelam, a newer generation bile acid sequestrant which is far better tolerated, has regenerated interest in this class of drugs. There are several reasons driving attention toward colesevelam. One is that a growing segment of patients on statins require adjunctive lipid-lowering therapies because of increasingly rigorous LDL-C targets in current guidelines. Bile acid sequestrants are potent LDL-C lowering agents in individuals intolerant to statins and the only agents other than statins to demonstrate a significant reduction in CV events in controlled trials. In patients who also have IFG or diabetes mellitus, colesevelam has also drawn attention because of its association with clinically-relevant improvements in glucose metabolism. According to Dr. Davidson, the mechanism of benefit appears to be derived from the ability of bile acid sequestrants to stimulate the liver X receptor (LXR) which has a role in glycemic control. In controlled trials, including those conducted in patients with DM2, colesevelam has been associated with meaningful improvements HbA1c and other measures of glucose metabolism when added to any of a broad array of antidiabetic therapies, including sulfonylureas, metformin, and insulin. While other bile acid sequestrants appear to share a favorable effect on glucose metabolism, they have never been as well studied in this context because of the adverse events which had already limited their utility when the favorable effect on glucose metabolism was recognized. Colesevelam, which has been associated with compliance rates of greater than 90% in controlled trials, was well tolerated in the current trial as it has been previously. On the basis of safety analyses that included patient-reported adverse events as well as liver function studies, urinalysis, and blood studies, Dr. Davidson called this agent “generally well tolerated” and specified that the safety profile of colesevelam is “a significant improvement over cholestyramine.” Evaluating glucose metabolism is a routine procedure in CV risk assessment and is particularly important in patients presenting with visceral adiposity or metabolic syndrome. A large proportion of these individuals will demonstrate elevated LDL-C, elevated triglycerides, abnormal HDL-C and IFG. Within the goal of favorably affecting this array of metabolic disturbances, including bringing patients to the LDL-C target, the results of this randomized study are consistent with favorable effects previously reported on LDL-C and IFG. In the context of niacin treatment, which has a negative effect on glucose metabolism, Dr. Davidson considers adjunctive colesevelam to be a viable strategy in routine patient management.
Conclusion
The interrelationship of CV risk factors is encouraging comprehensive treatment strategies that integrate treatment goals rather than addressing each risk individually. This is important because many risk factors, including dyslipidemias and impaired glucose metabolism track together. The efficacy of the bile acid sequestrant colesevelam in producing relatively large reductions in LDL-C with favorable effects on glucose metabolism is relevant to the rising rates of metabolic syndrome in which both of these metabolic abnormalities are common.