Gastroenterology
Digestive Disease Week (DDW) 2013
Adhesion Factor Inhibitors Fundamentally Shift Risk-Benefit of Biologics in IBD
Orlando – Based on phase 3 trial evidence, adhesion factor inhibitors may fundamentally shift the risk-to-benefit ratio of biologics in the treatment of inflammatory bowel disease (IBD). The primary advantage, based on data with an agent likely to advance to regulatory approval, is an ability to confine biologic activity to the gut. Data from the trial program that was presented at this year’s Digestive Disease Week (DDW) demonstrated encouraging clinical remission rates at one year in both ulcerative colitis (UC) and Crohn’s disease (CD). The remission rates suggest that localized inhibition of molecular processes fundamental to inflammation is effective. In addition, rates of infection and other markers of systemic immune suppression were similar to placebo.
Newer Inhibitors offer Promise in Targeting Adhesion Factors
Adhesion factors are an attractive biologic target for autoimmune diseases because they traffic the mediators of an inflammatory response. In inflammatory bowel disease (IBD), the specific value of inhibiting an integrin adhesion factor was initially demonstrated by an agent that was withdrawn because of off-target effects. Newer inhibitors, unlike the agent now withdrawn for use in IBD, have been designed to inhibit adhesion factors that act only in the gut. This was the premise in the development of vedolizumab, a gut-specific, adhesion-factor monoclonal antibody at the most advanced stage of clinical testing. This agent selectively blocks the α4β7MAdCAM-1 complex that mediates leukocyte homing to the intestine, a key step in the inflammatory response.
As explained by Dr. Brian Feagan, University of Western Ontario, London, Ontario, vedolizumab “raises the possibility of gut-specific immune modulation.” Gut-specific activity is a critical distinction between vedolizumab and natalizumab, which was withdrawn for its association with progressive multifocal leukoencephalopathy (PML). Vedolizumab only inhibits α4β7 and requires the presence of the gut-specific MAdCAM-1 complex. Natalizumab inhibits both α4β1 and α4β7. It is not gut-specific but acts systemically, including in the central nervous system (CNS), which is the presumed source of its association with PML.
GEMINI I and II Pooled Data
The clinical data seem to demonstrate this distinction: in the clinical trials program with vedolizumab in ulcerative colitis (UC) and Crohn’s disease (CD), the high rates of clinical remission were characterized by Dr. Feagan as “reminiscent” of those achieved with natalizumab, widely considered the most effective anti-inflammatory biologic yet produced for clinical use. However, “there are no striking differences in serious infection or any infection” when vedolizumab is compared with placebo. With the amount of exposure to vedolizumab in clinical trials to date, several cases of PML would have been expected.
Safety Analysis
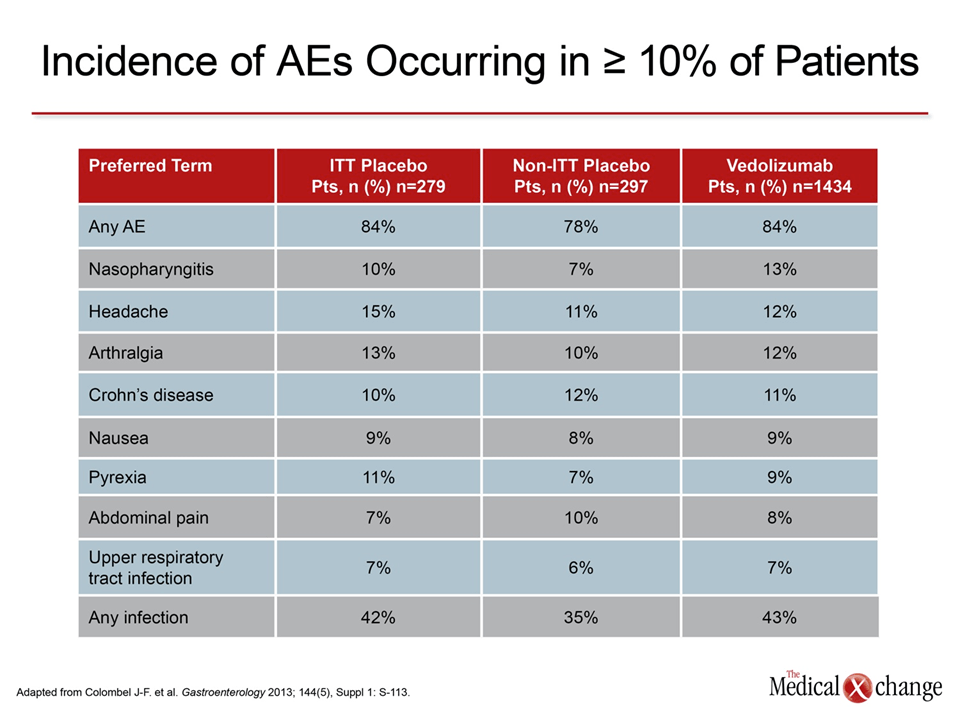
In a new integrated safety analysis of vedolizumab from the phase 3 trials in UC and CD presented at Digestive Disease Week (DDW) 2013, the rate of infections was 42% and 43% for placebo and vedolizumab respectively, on an intention-to-treat (ITT) basis. In an extended breakdown of adverse events (AEs), no AE was significantly more common on vedolizumab relative to placebo (Table 1). While serious AEs occurred more frequently on vedolizumab relative to placebo (19% vs. 15%) on an ITT analysis, rates were numerically although non-significantly lower after adjusting for exposure.
With more than 1400 patients exposed to vedolizumab in the phase 3 trials, “we have not so far seen a safety signal” regarding the types of risks, particularly infection, which has been observed with TNF inhibitors and other biologics, reported Dr. Jean-Frédéric Colombel, who is affiliated with the Centre Hospitalier Universitaire (CHU) de Lille, France, and is a visiting professor at the Mount Sinai School of Medicine, New York City, New York.
Efficacy Data: Sustained Healing Rates are Promising
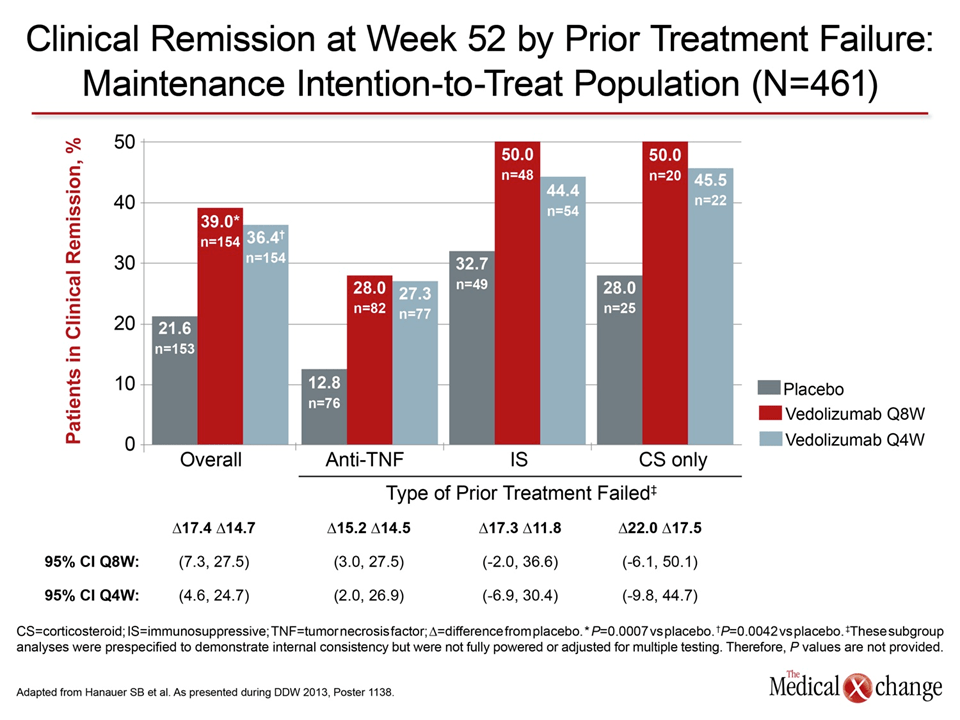
The promise of a more favorable benefit-to-risk ratio is supported by data updated at this year’s meeting. While acute healing rates with vedolizumab relative to placebo have been on the order of other biologics, the sustained healing rates in CD at 1 year are particularly encouraging. In a phase 3 subanalysis of CD patients who previously failed TNF inhibitor therapy, Dr. Stephen Hanauer, University of Chicago, Illinois, reported that clinical remission rates at 52 weeks were 39% overall on an ITT basis on an every-8-week schedule. Remission rates climbed to greater than 50% in patients who had not previously failed a biologic (Fig. 1).
Other agents expanding biologic targets controlling the characteristic inflammatory processes of autoimmune diseases are in development. In his review, Dr. Feagan cited new phase II data with etrolizumab, which is an antibody to the β7 epitope. Inhibitors of CCR9 and the sphingosine-1-phosphate receptor are in earlier stages of clinical development. The promise of these agents is a level of activity similar or greater to that provided by TNF inhibitors with a more favorable AE profile, including a reduced risk of infection and cancer.
Conclusion
In the treatment of IBD, biologics with activity localized to the gut may reduce systemic changes in immunologic modifier function, circumventing risks of infection. While TNF inhibitors have provided unprecedented activity for IBD as well as other autoimmune diseases, the quest for more focused therapies is accelerating. Advances have the potential to radically alter the benefit-to-risk ratio of these therapies.