Gastroenterology
Digestive Disease Week (DDW) 2013
Optimization of PPI Therapy in GERD: Need for Acid Control Over Each 24-hour Period
Orlando – A back-to-basics emphasis on the importance of acid control in gastroesophageal reflux disease (GERD) resurfaced at the 2013 Digestive Disease Week (DDW). In patients with upper gastrointestinal (GI) complaints who do not respond to proton pump inhibitors (PPIs), there are now a number of diagnostic studies to consider, but these studies are employed after first optimizing PPI regimens, according to several experts placing newer tests into context. While not all upper GI symptoms represent GERD, the optimization of PPI therapy, a concept related to the duration of acid control over each 24-hour period, is the most appropriate first step to rule out acid-related disease.
Upper gastrointestinal (GI) symptoms have numerous etiologies and can be heterogeneous in presentation, but the reflux of acid into the esophagus remains the most common source of these complaints. Algorithms that rely on impedance testing and pH monitoring have been developed to guide therapy in patients who do not respond to proton pump inhibitors (PPI) therapy, but several experts, including Dr. David Armstrong, Division of Gastroenterology, McMaster University, Hamilton, Ontario, emphasized that PPIs should first be optimized before moving to more complex and costly diagnostic studies.
Gastroesophageal reflux disease (GERD) is “a symptomatic diagnosis aided by empirical [PPI] therapy over at least 16 weeks with a step up,” explained Dr. Armstrong. He was joined by other experts, including Dr. Michael Vaezi, PhD, Division of Gastroenterology, Vanderbilt University, Nashville, Tennessee, who indicated that additional diagnostic tests can be helpful but should be reserved for those whose symptoms are not adequately controlled after “optimizing” PPIs.
The principle of optimized PPI therapy is durable acid control over the period in which acid pumps are being formed in the gastric parietal cell. These are meal-stimulated. First-generation PPIs have a half-life of 3 to 4 hours. If taken in the morning, these inhibit pumps triggered by the morning meal. Although sufficient in some, optimization of PPI therapy requires a longer duration of acid control to prevent rising gastric acidity as subsequent meals trigger new acid pump production.
Bioavailability
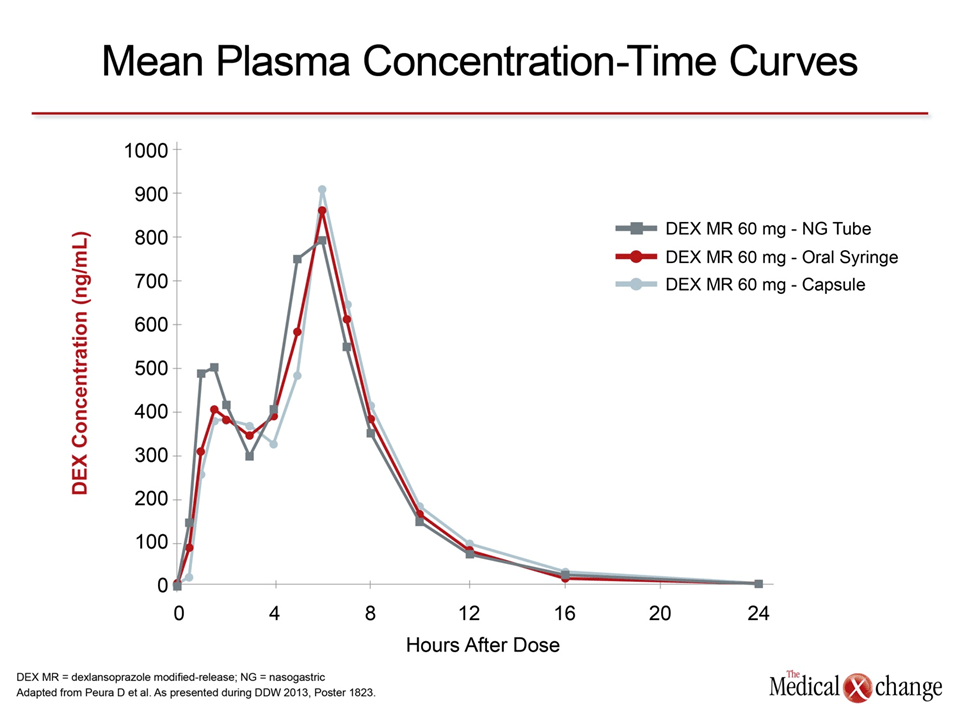
Twice-daily PPI therapy is an option to increase the duration of acid control, but it is also possible to preserve the advantages of once-daily PPI with the dexlansoprazole modified-release (MR). The pharmacokinetics of this agent has been described previously, but the peak plasma concentration curves were recreated at this year’s Digestive Disease Week (DDW) in a study of alternative delivery strategies for those unable or unwilling to take the capsule. The study showed that an aqueous solution created by mixing granules from the capsule with water provide the same sustained plasma concentrations regardless of route to the stomach.
In the crossover study, the pharmacokinetics of dexlansoprazole were measured sequentially in volunteers taking the capsule, the aqueous solution by oral syringe, and the aqueous solution by nasogastric (NG) tube or by an oral syringe. The two-peak plasma concentration times established previously with the capsule and seen again in this study were recreated with either method of delivering the aqueous solution. In all cases, serum concentrations remained at therapeutic levels for approximately 10 hours (Fig. 1).
NERD Patients and Relief from Dyspepsia
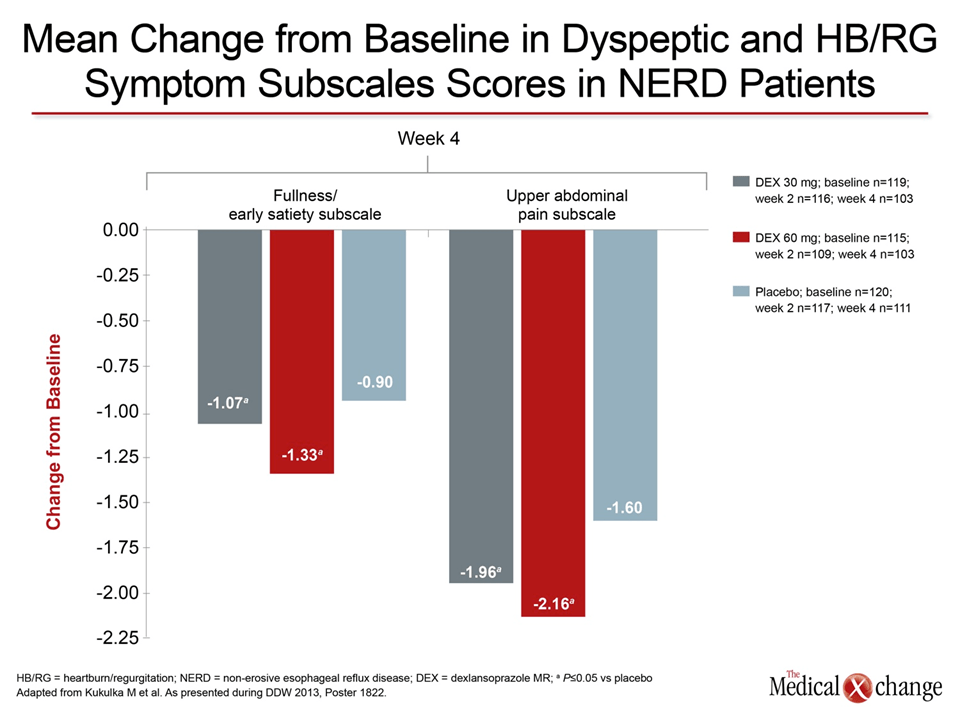
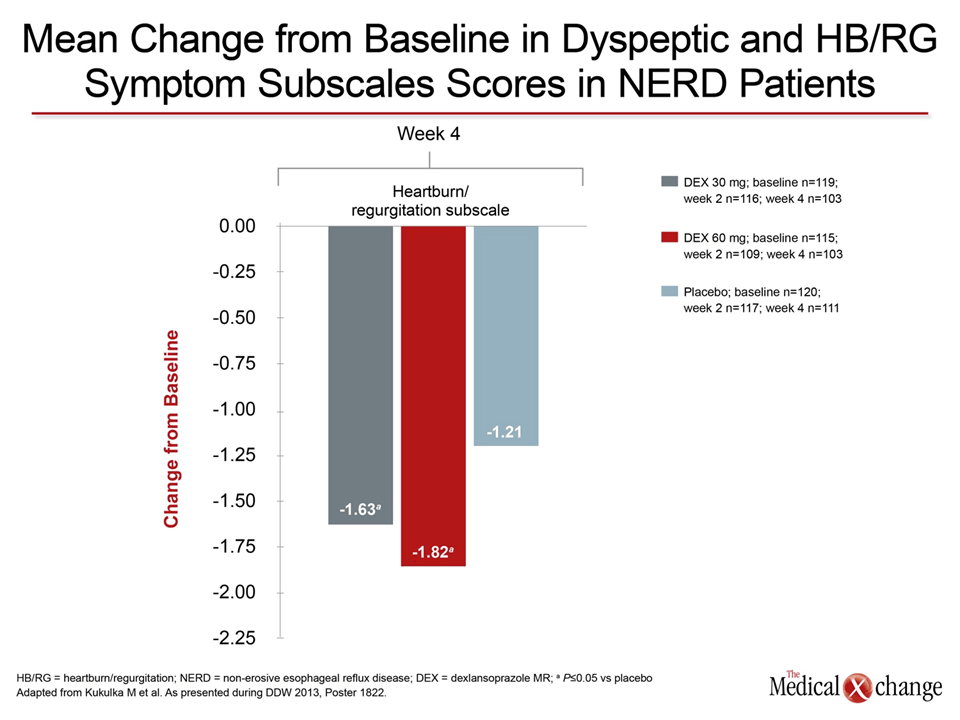
“A longer suppression of gastric acid production predictably translates into less opportunity for acid-related symptoms. It is a simple premise.”
“A longer suppression of gastric acid production predictably translates into less opportunity for acid-related symptoms. It is a simple premise,” reported Dr. David Peura, University of Virginia, Charlottesville. Dr. Peura evaluated dexlansoprazole in a subset of patients that had both non-erosive GERD (NERD) and dyspepsia. Demonstrating the principle of optimizing PPI therapy, the study showed that both GERD and dyspeptic symptoms were significantly reduced on dexlansoprazole relative to placebo in dose-dependent fashion (Fig. 2).
Asked why acid control would influence symptoms of dyspepsia, Dr. Peura explained that a reduction in gastric acidity could exert a favorable effect on gastric volume, thereby exerting a direct effect on sensations of pain or satiety. He suggested that the long duration of action of dexlansoprazole could be just as relevant to amelioration of dyspepsia as for GERD.
A similar comment about the consistency of acid suppression was made by the author of a study that evaluated PPIs in GERD patients with chronic cough. In this 134-patient study, PPI therapy was associated with improvement in chronic cough in 61.7% of the patients, but the author, Dr. Ji Huyn Lim, Bundang Hospital, Seoul National University, Korea, stressed that cough and other extraesophageal symptoms required more consistent acid suppression over a longer period than control of esophageal symptoms.
Conclusion
Optimized PPI therapy is a critical step in a treatment algorithm that addresses upper GI symptoms consistent with GERD. Optimization signifies persistent blockade of the acid pumps stimulated with each meal. This requires twice-daily dosing of conventional PPIs or a sustained release PPI. While not all upper GI symptoms are GERD, optimal acid control is the most critical feature to GERD control.