ADHD
4th World Congress on ADHD
Drug Combinations Frequently Employed to Control ADHD in Children and Adolescents
Milan – According to a large Canadian survey designed to capture real-world clinical practice, one in five children appear to require two or more psychotropic drugs to control symptoms of attention deficit hyperactivity disorder (ADHD). While the survey found that the rates of combination therapy were higher in children with a diagnosed psychiatric comorbidity, the rates remained substantial even in those without an established mental health or neurologic comorbidity. The most common psychotropic drugs used in combination with a stimulant were alpha-2 receptor agonists, antipsychotic agents, and antidepressants. Most adjunctive therapies were used out of labeling. The survey suggests more data is needed to guide second- and third-line ADHD therapies when stimulants are not sufficient.
One in five children and adolescents in Canada receiving a long-acting stimulant for attention deficit hyperactivity disorder (ADHD) is receiving at least one other psychoactive drug to control symptoms, if data collected in Quebec is representative. The data derived from actual clinical practice over a 12-month period was collected from the Régie de l’assurance maladie du Québec (RAMQ), which is the province-wide health plan database. It includes approximately 3.3 million patients covered for medical service and prescription drug use.
One in five children and adolescents in Canada receiving a long-acting stimulant for ADHD is receiving at least one other psychoactive drug to control symptoms.
“The data suggests we need more treatment options in patients with ADHD. Although the gold standard, long-acting stimulants are effective in the majority of children, the data from this survey is consistent with other evidence that 20% to 30% of children with ADHD do not achieve adequate control on stimulants alone,” reported the first author of the study, Dr. Leila Ben-Amor, Ste. Justine Hospital, University of Montreal. “For many, I think it is not a question of no response, but not enough response to stimulants, which is why they receive additional therapy.”
Data from children aged 6 to 17 with a diagnosis of ADHD participating in the RAMQ plan was included for this study if they had received at least a 30-day supply of stimulants during a 12-month period of eligibility. Children were defined as having received combination therapy if at least a 30-day supply of a psychoactive therapy was prescribed over the same period that the children received a stimulant. Comorbid mental health and neurologic diagnoses were noted.
Of the more than 13,000 children in the RAMQ database with a diagnosis of ADHD during the period of eligibility, 9,431 met all the predefined inclusion criteria. Of these, 2227 (24%) also had a diagnosis of an additional mental health or neurologic disorder and were considered to have comorbid pathology. The average age in the study population was 11.3 years, and 27.7% were female.
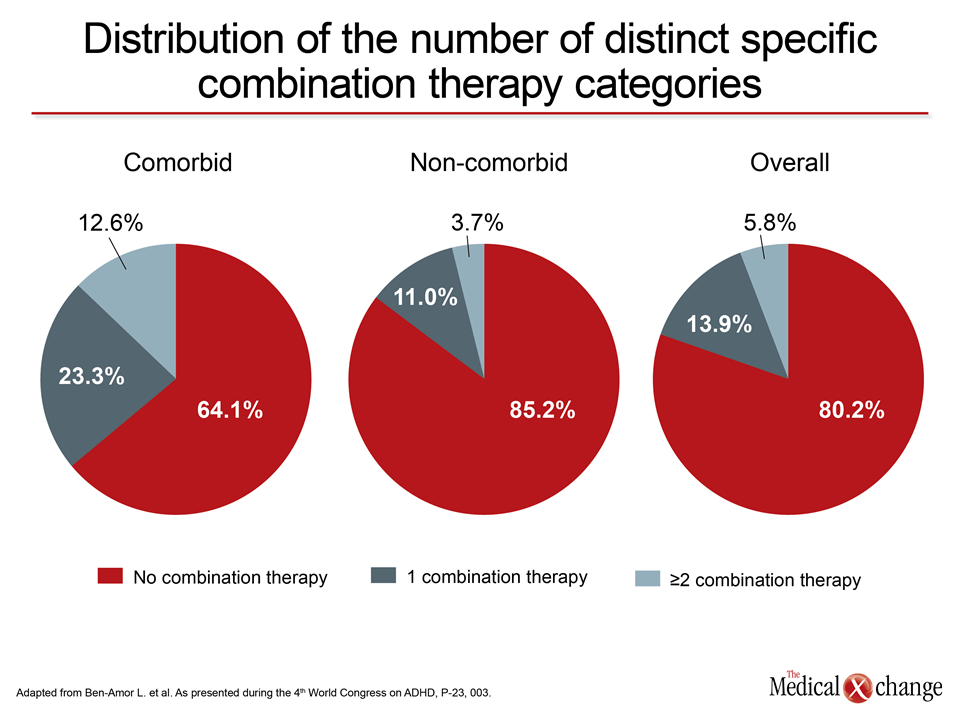
Overall, 19.8% of the ADHD patients in the database used a stimulant with another psychoactive agent. The proportion climbed from 14.8% in the group without comorbidity to 35.9% in the comorbid group. The proportion on two or more psychoactive drugs rose from 3.7% in the group with ADHD alone to 12.6% in the comorbid group. (Fig. 1).
In those with comorbid conditions, it is possible that some or all of the combination agents were prescribed to control the comorbidity rather than ADHD symptoms. However, the types of therapies combined with stimulants were similar in those with or without comorbidity. All drugs added to the first-line, long-acting therapies would have been used off label if prescribed to control ADHD, even though some of those used have been identified as third-line choices in the Canadian ADHD Resource Alliance (CADDRA) guidelines.
CADDRA Guidelines: First-line Agents in Uncomplicated ADHD
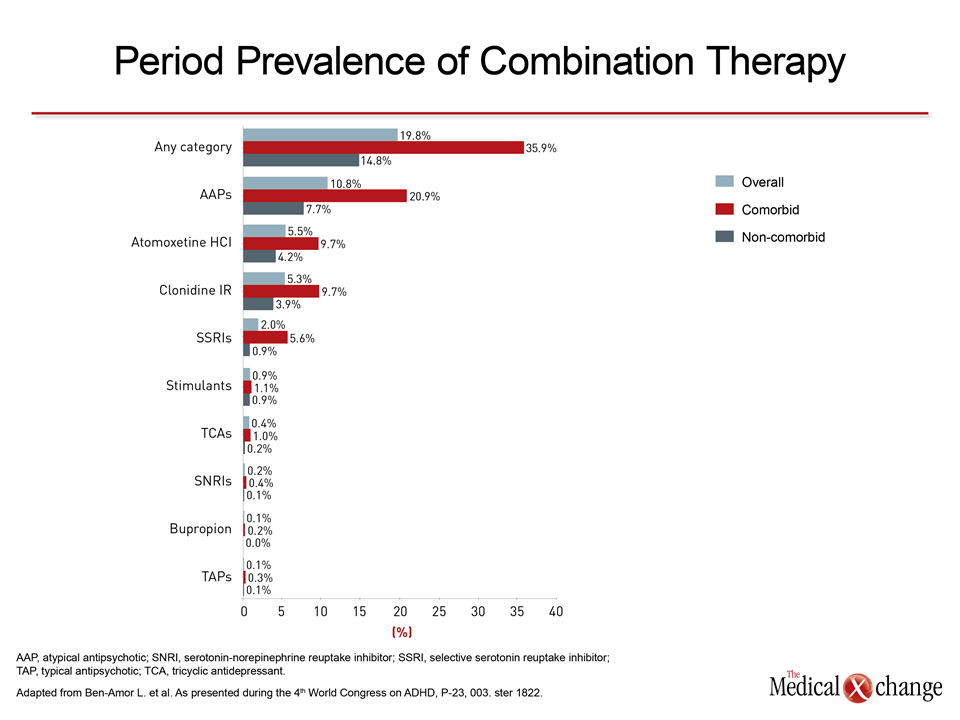
Of the adjunctive agents combined with stimulants in the RAMQ study, the most common were antipsychotics, which are known to reduce aggressive behaviors, atomoxetine, which is the only non-stimulant agent identified by CADDRA as a first-line therapy for ADHD, and alpha-2 agonists such as clonidine, which has demonstrated benefit as a monotherapy and adjunctive therapy against ADHD symptoms in controlled studies but have not yet been approved for this indication. In general, patients with a comorbid condition were twice as likely to receive any of the adjunctive therapies employed as those without (Fig. 2).
The substantial proportion of children with ADHD who are on combination therapy was not unexpected. The proportion of children with an inadequate response to stimulant therapy has been previously estimated to be in the range of 30%, according to several studies cited by Dr. Ben-Amor. Moreover, previously conducted studies, such as one conducted in the United States (Sikirica V et al. J Manag Care Pharm 2012;18:676-89), have also found substantial rates of combination prescriptions in children with ADHD. It is notable that many of the agents most commonly combined with stimulants in the US study, as in the Quebec study, were antipsychotic drugs and alpha-2 agonists.
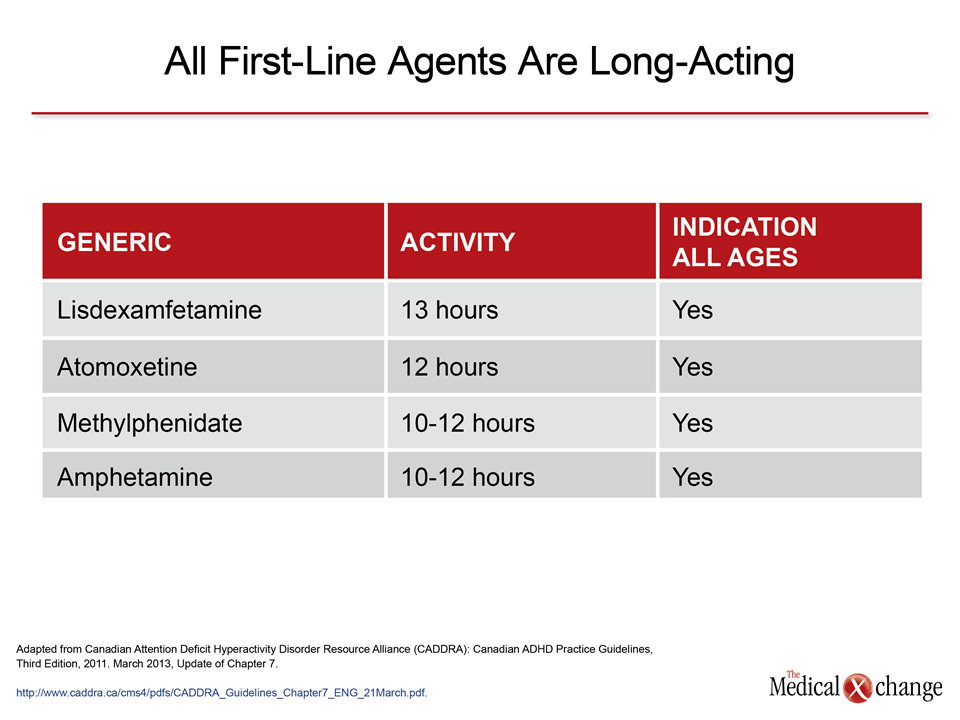
In current CADDRA guidelines, which only include long-acting stimulants and atomoxetine for first-line therapy for children and adolescents with uncomplicated ADHD, switching first-line agents or between classes of stimulants is a reasonable approach if response to the initial agent is inadequate. It may be particularly appropriate to offer a stimulant with a longer duration of action than the initial agent if one is available. The clinical value of extended symptom control is the primary reason all of the first-line agents recommended by CADDRA have relatively long half-lives (Table 1).
Whether children on combination therapy in the RAMQ database had stimulant therapy optimized before initiating combination therapy is unclear, but use of short-acting agents was common when the study population was stratified for their stimulant prescriptions, particularly among those taking methylphenidate of which nearly 30% of prescriptions were for short-acting formulations. CADDRA lists short-acting methylphenidate and short-acting amphetamines as second-line therapy for both children and adolescents.
Health Canada has recently approved an adjunctive therapy for ADHD, providing an approved option for patients not effectively controlled on long-acting, first-line agents.
At the time that data was presented, there were “no combination therapies approved for the treatment of ADHD in Canada,” according to Dr. Ben-Amor. She suggested this data provides evidence “that more treatment options, including combination strategies, are needed” because of the reasonable expectation that more options provide a “greater potential to match patients with an effective therapy.” However, as of July 5, 2013, Health Canada has approved guanfacine extended release (XR) as an adjunctive therapy for ADHD, providing an approved option for patients not effectively controlled on long-acting, first-line agents.
Objective Data and Guidance for Combination Therapy are Needed
When considering combination therapy for ADHD, the problem is not just an absence of approved therapies but a basic lack of data. While this survey suggests that clinicians are improvising with psychoactive agents when an initial stimulant therapy is not providing adequate control of symptoms, it is not clear that the choices being used are the most rational whether or not individuals have a comorbid diagnosis. The RAMQ data indicates that specialists are more likely to be involved in the care of children with a comorbidity, but Dr. Ben-Amor indicated that objective data is needed to guide both specialists and primary care physicians. “Stimulants are effective in ADHD, but for those without adequate control at the maximum tolerated dose, the next step is not well defined,” Dr. Ben-Amor remarked.
CADDRA guidelines support the use of augmentation strategies when response to long-acting stimulants is inadequate at optimally-tolerated doses, but they suggest that this type of care should be provided by specialists. Examples of third-line agents listed by CADDRA include modafinil, buproprion, and imipramine, but the data from the RAMQ database indicate that alpha-2 agonists are more likely to be used by clinicians in combination than any of these three drugs. In a recently-published overview of these agents, the author concluded that there is clinical data to support both guanfacine and clonidine in the treatment of ADHD (Sallee F et al. J Child Adolesc Psychopharmacol 2013;23:308-19).
ADHD and Comorbidities
Data from the RAMQ database indicated that about half of the stimulants were prescribed by pediatricians. The proportion was only slightly lower in children with comorbid disease. Relatively few prescriptions for stimulants or for combinations were written by neurologists in the RAMQ analysis, but psychiatrists prescribed combination therapy in almost 20% of those with comorbid disease versus 11.5% of those with ADHD alone.
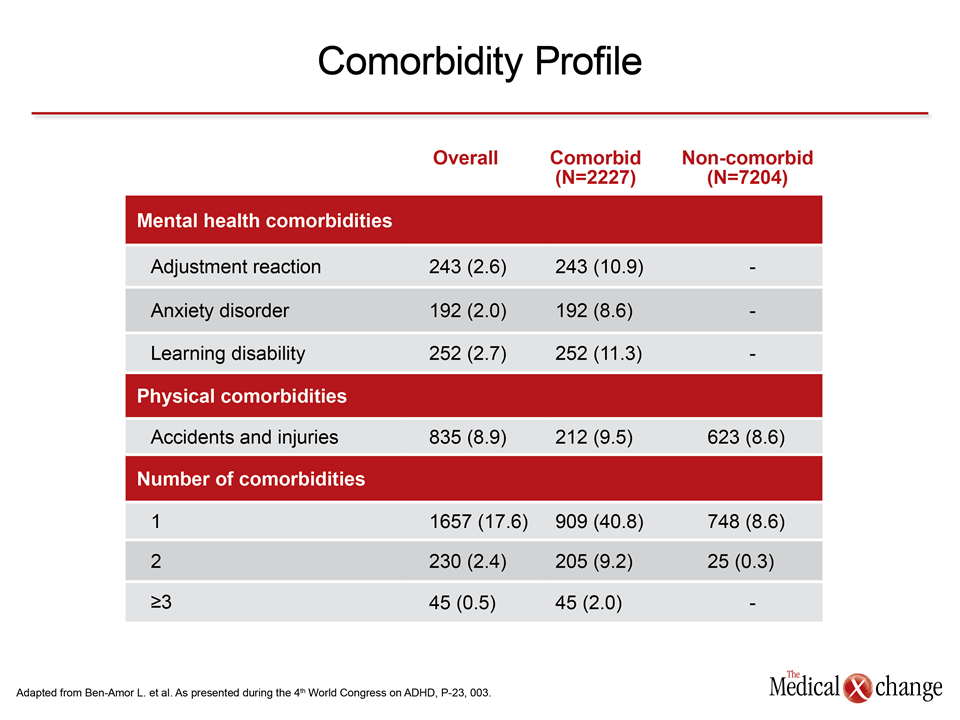
ADHD appears to be accompanied by a wide variety of comorbid mental health or neurological disorders, but the three most common comorbidities in the order of their prevalence in RAMQ were learning disability (11.3%), adjustment reaction (10.9%), and anxiety disorder (8.6%). More than 10% of the study population had 2 or more comorbidities (Table 2).
The Value of Sustained Symptom Control
ADHD is a common condition. In Canada, the estimated prevalence is 9% for boys and 4% for girls. Although ADHD can persist into adulthood, its early recognition and treatment has the potential to circumvent the risk of developmental problems associated with the adverse effect of symptoms on a broad range of daily activities. While impaired school performance was once the primary focus of therapy, it has been increasingly recognized that sustained symptom control beyond school hours has implications for normal social development.
In CADDRA guidelines, duration of effect is listed second after age as one of 13 key factors to consider in drug selection. Although it was suggested that pharmacologic treatment of ADHD should not be initiated before the age of 6 except by a specialist, the guidelines indicate that the value of sustained symptom control may increase with age, particularly in ADHD subtypes that have the potential to adversely affect social relations, home life, or organizational function. It was noted, for example, that hyperactivity in early childhood can evolve into stimulus-seeking behavior in adolescence, which may have implications for optimal therapeutic approaches.
The contribution of the RAMQ data is that it verifies a widespread perception that a substantial minority of children and adolescents with ADHD are not achieving sufficient symptom control on stimulants alone. The next step is to develop data that will guide rational choices for the next step in treatment.
The contribution of the RAMQ data is that it verifies a widespread perception that a substantial minority of children and adolescents with ADHD are not achieving sufficient symptom control on stimulants alone. According to Dr. Ben-Amor, the next step is to develop data that will guide rational choices for the next step in treatment.
“We think that combination therapy is needed in some proportion of patients but we do not know what the best combination might be, particularly if we think about different types of patients,” Dr. Ben-Amor said. “This study, I think, tells us we need data.”
Conclusion
Data drawn from clinical practice in Quebec indicated that a small but substantial minority of children and adolescents with ADHD are not achieving sufficient symptom control on long-acting stimulant therapy alone. Even in ADHD patients without a diagnosed comorbidity, 15% are taking two or more additional agents for symptom control. While CADDRA guidelines recognize that augmentation to stimulant therapy with other psychoactive agents may be needed in some individuals, the Quebec study results underline the need for objective data to guide rational choices.