neurology
Alzheimer's Association International Conference (AAIC)
Sensitive Tool Identified for Early Detection of Alzheimer’s Disease
Boston – More sensitive methods for early detection of Alzheimer’s disease (AD) that reduce or circumvent the major weaknesses of previous tools are expected to be a major boost in the objective assessment of suspected memory loss. While several approaches are being pursued, most can be administered repeatedly by healthcare staff with minimal training. Of the tests, the advantage of the one that appears closest to clinical application is its relative freedom from confounders such as baseline intelligence. Cognitive function and education have been important obstacles to the reliability of earlier assessments. Tests of early memory loss are expected to allow clinicians to provide reliable information to patients and families even when symptoms are discrete.
Due to the frequency of sporadic memory loss in healthy individuals, objective measures of change in cognitive function are needed. Although a diagnosis of Alzheimer’s disease (AD) can be made with increasing certainty with advancing disease, there is no current tool to guide patients experiencing discrete symptoms recognizable only to themselves or close family members. An accurate screening tool has been intensively sought for patients and families seeking objective information when concerned about real or perceived episodes of mild cognitive impairment. Several strategies are being pursued. Validation data indicate that a method that appears to be nearing release as a routine clinical tool is accurate and reproducible independent of baseline cognitive function.
Promising Test Sensitive to Discrete Symptoms
“The problem with any of the tools that we use now is that they are not accurate for subtle disease, while performance is affected by baseline intelligence, mood disorders, such as depression, or, in some cases, cultural or language barriers. The value of the new test is that it has not been affected by any of these variables or by practice effects,” reported Dr. Yen Ying Lim, who participated in the development of this test when affiliated with the Florey Institute of Neuroscience and Mental Health, University of Melbourne, Australia. Now affiliated with Brown University, Providence, Rhode Island, Dr. Lim reported that the new test, designed specifically for AD, can be performed in about 15 minutes and has high specificity and sensitivity for detecting any form of mild cognitive impairment.
The test, which is being developed under the trade name Cognigram, consists of 4 tasks performed on a computer. Individually, the tasks provide information on psychomotor function, attention, learning, and working memory. For the analysis, two composite scores are derived by pairing the four tasks. This produces one composite score for the psychomotor and attention tasks and another for the learning and working memory. In a validation trial that included 653 elderly individuals, eachproduced reasonably high sensitivities and specificities for both mild cognitive impairment and AD when employed separately but better accuracy when used together.
“In this analysis, the CogState Brief Battery was administered just once and the sensitivity for the learning/working memory composite was 100%. The specificity was 85.7%. For mild cognitive impairment of a non-AD etiology, the sensitivity and specificity were 80.4% and 84.7%, respectively,” reported Dr. Lim, who performed this work with a team of investigators led by Dr. Paul Maruff, who remains at the Florey Institute of Neuroscience and Mental Health. The study population was drawn from the Australian Imaging, Biomarkers and Lifestyle (AIBL) study. Of the 653 patients evaluated, 44 had AD, 48 had mild cognitive impairment of another etiology, and the remaining had no cognitive deficits.
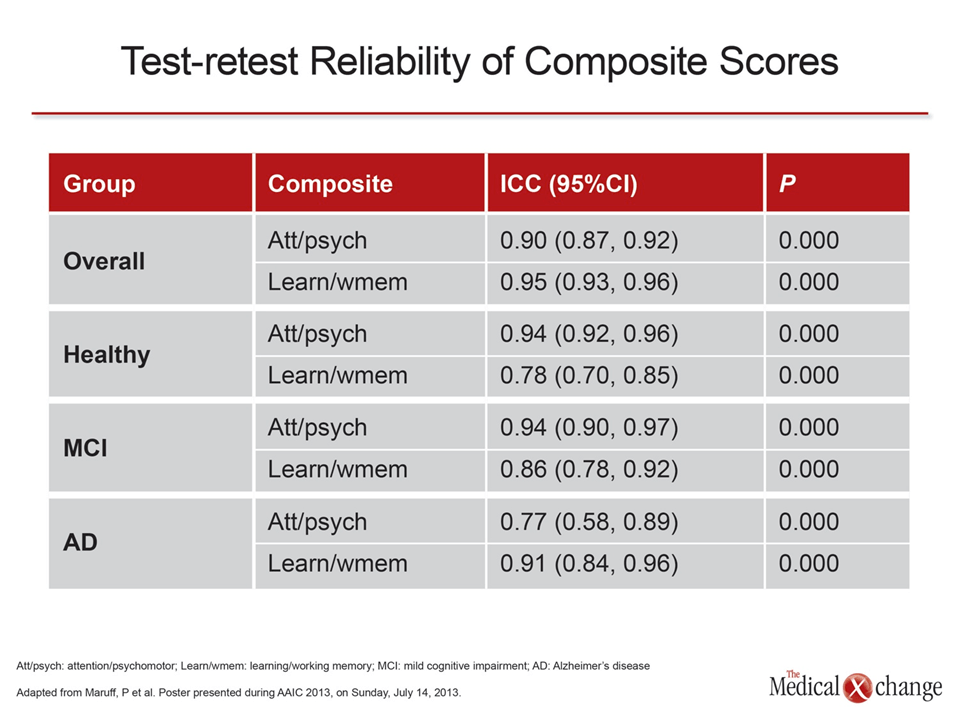
Even though the test is highly effective in detecting AD when administered at a single point in time, the accuracy improves with sequential administration. Importantly, the testing draws on cognitive processing that does not benefit from practice effects. In the most recent study, the test-retest reliability remained high for both composite scores across each of the populations tested (Table 1).
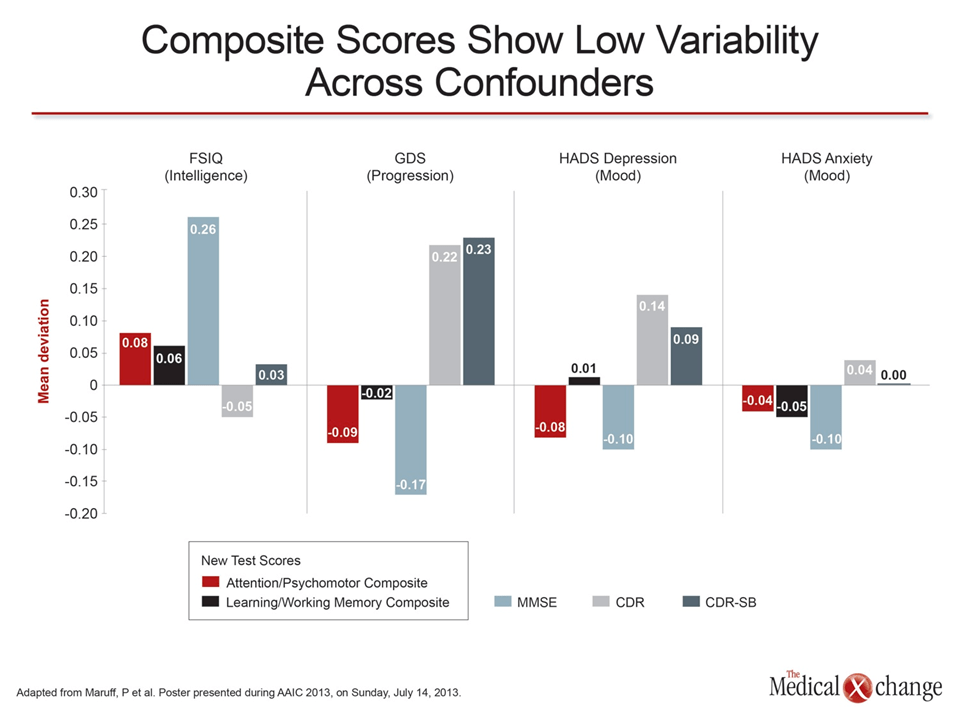
The most significant advantage of the new test is its accuracy across confounding factors such as intelligence and mood. Each composite score was compared against the Mini Mental Status Examination (MMSE), the Clinical Dementia Rating (CDR) or the Clinical Dementia Rating Sum of Boxes (CDR-SB) tests, all of which are commonly used in evaluating AD. Although the composite scores did not always demonstrate the lowest degree of variability for all of the parameters, which included Full Scale Intelligence Quotient (FSIQ), Global Deterioration Scale (GDS), and the Hospital Anxiety and Depression Scale (HADS) for depression and anxiety, the overall consistency was greater (Fig. 1).
“I think there is an important current need for this test. Patients who are experiencing the early stages of memory loss are anxious to receive a diagnosis.”
The test is designed to be administered by any healthcare professional with a minimum amount of training, and it would be appropriate for use even in the primary care setting. The test is already being used widely in clinical research to test emerging treatments, but the study has immediate practical value, according to Dr. Lim.
“Everyone involved in Alzheimer’s research is waiting for an effective intervention. When and if one comes along, this test will be very useful for evaluating whether patients are responding, but I think there is an important current need for this test. Patients who are experiencing the early stages of memory loss are anxious to receive a diagnosis. Certainly, many are hoping for a negative result, but there is value in providing patients with definitive information,” Dr. Lim said.
Two other strategies have also placed a focus on simplicity and ease of administration but may not be as versatile when testing individuals with varying language skills or hearing acuity. One test, developed at the Mount Sinai School of Medicine in New York City, employs audio cues. Called the Audio Recorded Cognitive Screen (ARCS), patients listening on headphones write down responses, and changes in cognitive ability are tracked over time. According to Dr. Margaret C. Sewell, a Mount Sinai researcher who led a study that tested this tool in 19 patients, ARCS was a better discriminator between controls and those with mild cognitive dysfunction than MMSE, the Clock Drawing Test (CDT), or MMSE and CDT combined. She said the tool may be appropriate for use in primary care.
Another tool, called Cognistat, can be administered in 15 to 20 minutes like some other strategies, but it is not designed specifically for memory loss from AD or other pathologies that come with old age. Rather, it captures cognitive loss from a broad range of causes, including trauma. While no new data on this test were presented at this year’s AAIC, this test is also representative of the initiative to improve objective and convenient examination of cognitive function in an office setting.
Conclusion
A broad number of strategies have been developed and are used with varying accuracy in the evaluation of mild cognitive impairment. A new test that circumvents the adverse influence of confounding variables on the sensitivity for AD offers an opportunity to provide guidance at a level of disease activity that would be otherwise undetectable. It is expected to be an important tool for managing individuals who seek guidance when cognitive impairment is suspected.