Diabetes
European Society of Cardiology (ESC) Congress 2013
First Two Large Multinational Trials Validate Cardiovascular Safety of DPP-4 Inhibitors in the Treatment of Diabetes
Amsterdam – Cardiovascular (CV) safety has been confirmed in the first two of a series of multinational studies conducted with dipeptidyl peptidase-4 (DPP-4) inhibitors. Four trials were launched in response to a U.S. Food and Drug Administration recommendation issued in 2008 that requested evidence of CV safety for any new antihyperglycemic agent. Each been powered to evaluate CV safety as a primary endpoint in high CV risk patients even though the CV safety signal from previously pooled phase 3 data post-hoc analyses had been encouraging. The two trials presented at the 2013 European Society of Cardiology (ESC) Congress provide the first validation of CV safety with DPP-4 inhibitors. Two more trials are underway. When all four trials are completed, an exceptionally large body of data will be available to judge both CV safety, which is the primary endpoint for each, and the overall tolerability of a class of drug.
SAVOR-TIMI 53 and EXAMINE Trials
The two large multicenter placebo-controlled trials testing the cardiovascular (CV) safety of dipeptidyl peptidase-4 (DPP-4) inhibitors were among the most closely watched late-breaking trials presented at the 2013 European Society of Cardiology (ESC) Congress. The SAVOR-TIMI 53 trial evaluated saxagliptin in 16,492 type 2 diabetes mellitus (T2DM) patients who had a history or were at high risk of CV disease. The EXAMINE trial evaluated 5,380 T2DM patients who had been diagnosed with an acute coronary syndrome (ACS) within the 90 days prior to enrollment. The primary endpoint of CV safety was expressed as non-inferiority to placebo for the composite endpoint of death from CV causes, non-fatal myocardial infarction (MI) or non-fatal stroke. Both met their primary endpoint.
“When added to standard of care [for management of both T2DM and CV risk], saxagliptin neither reduced nor increased the risk of the primary composite endpoint,” reported Dr. Deepak Bhatt, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA. “The data fulfill the [U.S. Food and Drug Administration] FDA mandate.”
The mandate refers to the decision by the FDA to require a demonstration of CV safety for all new drugs in the treatment of T2DM. It was created several years ago after evidence indicated that rosiglitazone was associated with adverse effect on CV outcomes. Major trials were then launched for each of the DPP-4 inhibitors: sitagliptin, saxagliptin, linagliptin, and alogliptin. Although similar in intent, each of the trials employed slightly different designs and recruited T2DM patients at different levels of CV risk. The SAVOR-TIMI 53 trial with saxagliptin and the EXAMINE trial with alogliptin have now been completed. The TECOS trial with sitagliptin has a planned completion in December 2014. The completion of the CAROLINA trial with linagliptin is expected in 2018.
Guided by definitions provided by the FDA, the trial endpoints to validate non-inferiority to placebo for CV safety have been similar. However, each DPP-4 trial was structured to also evaluate superiority to placebo for CV risk reduction once non-inferiority is demonstrated. This outcome was included because of a signal of potential CV protection from clinical end experimental data, particularly a post-hoc, pooled meta-analysis of randomized, controlled trials of at least 6 months’ duration. In this analysis of 18 trials with more than 8,544 patients, DPP-4 inhibitors were associated with a 52% reduction (95% CI 0.31 – 0.75; P=0.001) relative to placebo in the risk of any adverse CV event (Patil HR et al. Am J Cardiol 2012;110:826-33).
The CV safety trials mandated by the FDA might provide an opportunity to prospectively demonstrate a CV risk reduction beyond the immediate goal of confirming CV safety.
CV Safety and CV Protection
These and other data have led to speculation that the CV safety trials mandated by the FDA might provide an opportunity to prospectively demonstrate a CV risk reduction beyond the immediate goal of confirming CV safety. At this year’s ESC, the chief investigators of the SAVOR-TIMI 53 and EXAMINE trials, as well as the ESC-invited discussants, characterized the primary outcome of CV safety as reassuring. However, the absence of any evidence of CV protection in these first two trials was characterized as disappointing. Based on the previous signal of benefit, several of the speakers speculated on the reasons for an absence of CV protection. Based on this speculation, the data from these studies do not apparently preclude the possibility of demonstrating protection in future studies.
“These data contain a positive message about CV safety, but we need more data before we can say that there is no CV benefit. It may be that 2 years of follow-up was inadequate to see a difference.”
“These data contain a positive message about CV safety, but we need more data before we can say that there is no CV benefit. It may be that 2 years of follow-up was inadequate to see a difference,” observed Dr. Michel Komajda, Head of the Cardiovascular Department, Pitié Salpêtrière Hospital, Paris, France. The remarks by Dr. Komajda, who was the ESC-invited discussant of the SAVOR-TIMI 53 trial, were echoed by Dr. Eugene Braunwald, Brigham and Women’s Hospital, Boston, MA, who was the ESC-invited discussant of the EXAMINE trial. Implying that design issues may have prevented a demonstration of CV protection, he indicated the initial failure to show CV protection was surprising in the context of “a large body of basic research” that supported the expectation of CV risk reductions.
More Data will be Helpful
Despite similar goals, each of the DPP-4 trials deserved to be evaluated independently not only because of potential differences between the agents but because of basic differences in the risk populations recruited for study and the power to show differences over the periods of follow-up.
A comparison of SAVOR-TIMI 53 and TECOS, which is the next DPP-4 inhibitor trial scheduled for completion, is illustrative. Unlike EXAMINE, which required ACS within 90 days of enrolment, SAVOR-TIMI 53 and TECOS enlisted high-risk populations more typical of routine clinical practice but with significant differences between the two. In SAVOR-TIMI 53, entry criteria included age of 40 years or older and either an established history of CV disease or multiple risk factors. In TECOS, patients were required to be age 50 years or older with a major clinical manifestation of disease, such as previous myocardial infarction, angiographic evidence of stenosis, or peripheral arterial disease. TECOS, with an enrolment of approximately 14,000 patients is, like SAVOR-TIMI 53, a large trial, but it was initiated earlier and will end later, so the mean follow-up will be longer. SAVOR-TIMI 53 was powered from 1040 events. TECOS is powered for 1300. In both SAVOR-TIMI 53 and EXAMINE, glycemic control was greater in the experimental arm. TECOS is designed to provide glycemic equipoise between the two arms, eliminating a potentially confounding variable.
The CAROLINA trial, which will be the last of the DPP-4 CV safety trials to be completed, recruited 6000 patients age 40 years or older with established CV disease or diabetes with end-organ damage. Unlike the other placebo-controlled CV safety studies, patients in CAROLINA will be randomized to the study DPP-4 inhibitor or the sulfonylurea glimepiride.
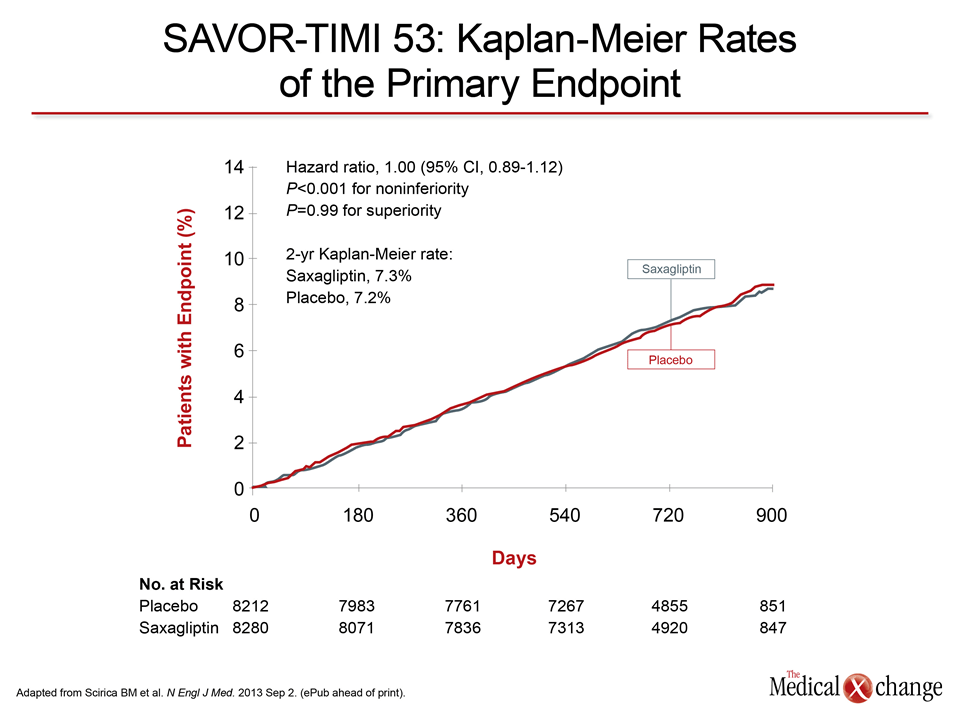
Based on the two DPP-4 inhibitor trials completed to date, the CV safety of this drug class appears established. At the end of the median 2.1-year follow-up, saxagliptin in SAVOR-TIMI 53 was exactly neutral for the primary composite endpoint, producing a hazard ratio (HR) of 1.00 (95% CI 0.89 – 1.12; P<0.001 for non-inferiority to placebo). However, there was no evidence of superiority (P=0.99) for the composite endpoint or for any event analyzed separately with the exception of hospitalization for heart failure, which was increased in the saxagliptin group (HR 1.27; P=0.007). Dr. Bhatt said the risk was concentrated in patients with a history of heart failure (Fig. 1). TECOS will shed more light on this matter as time to congestive heart failure is a secondary outcome measure.
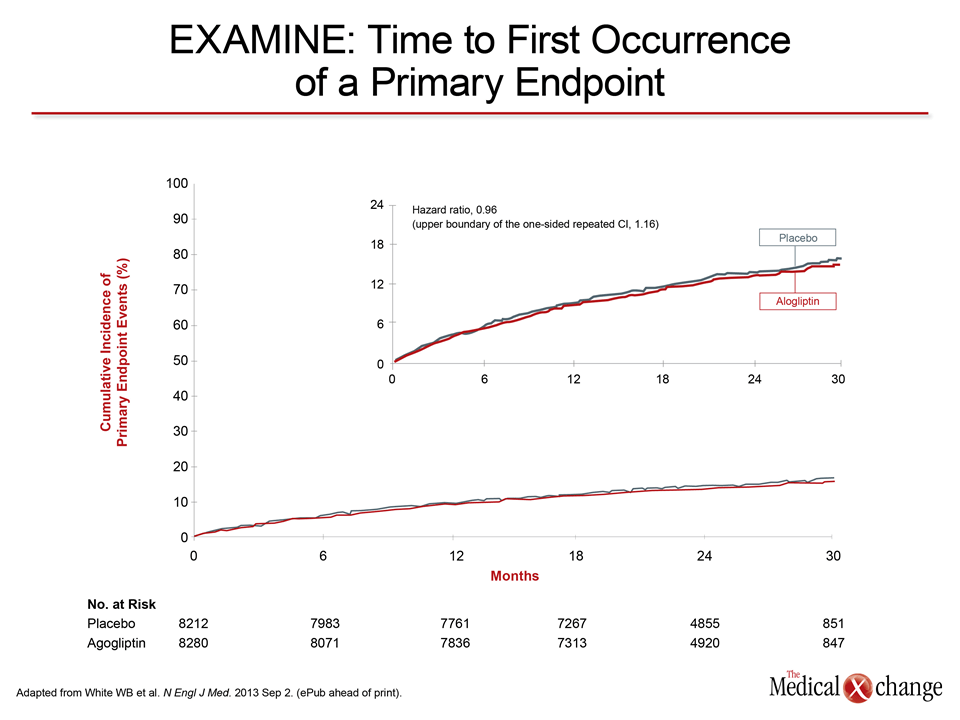
In EXAMINE, which enrolled a higher risk population but followed them for a shorter period, the results were similar. The HR for non-inferiority was 0.96 (P<0.001) (Fig. 2). Even though the rate of the composite primary event was slightly lower on alogliptin than placebo (11.3% vs. 11.8%), there was no significant evidence (P=0.32) of superiority for CV protection. Neither an expanded secondary composite endpoint nor any individual events within the primary endpoint showed any significant differences between alogliptin and placebo. No difference in rates of heart failure was observed in this study.
In both studies, glycemic control as measured with HbA1c was significantly greater for those randomized to the DPP-4 inhibitor relative to placebo even though the protocols permitted background antidiabetic therapies to be adjusted. It is notable that a high proportion of patients in both studies, including more than 45% of patients in EXAMINE, were taking a sulfonylurea, which have been associated with an increased risk of stroke in a recent meta-analysis (Monami M et al. Diabetes Obes Metab 2013 April 17 (ePub ahead of print). As for CV risk-lowering therapies, those in EXAMINE, perhaps reflecting a higher risk population, were more likely than those in SAVOR-TIMI 53 to be on aspirin (90% vs. 75%), statins (90% vs. 78%) or beta blockers (82% vs. 62%).
In the presentation of the SAVOR-TIMI 53 and EXAMINE results, the lead investigators and the ESC-invited discussants each commented on the absence of any signal of an increased risk of pancreatitis. There has been speculation about a potential risk of this event derived from a series of case studies, but these two large trials substantially reduce the likelihood that DPP-4 inhibitors are associated with this adverse event.
Ongoing Trials will Grow the Body of Evidence with the DPP-4 Inhibitor Class
The TECOS trial with sitagliptin and the CAROLINA trial with linagliptin will provide further answers and evidence about the long-term safety of the DPP-4 inhibitor class, but the evidence that DPP-4 inhibitors do not increase CV risk is, by itself, important new information, particularly with increasing appreciation of the numerous disadvantages of sulfonylureas, including their potential to contribute to disease progression. As a substitute for sulfonylureas in combination regimens with metformin, DPP-4 inhibitors are attractive because they offer a relatively low risk of hypoglycemia, they are not associated with weight gain, and they are well tolerated.
Conclusion
The first two of the four large CV safety trials with DPP-4 inhibitors, SAVOR-TIMI 53 with saxagliptin and EXAMINE with alogliptin, have provided strong and reassuring evidence that these agents do not increase CV risk. Therefore, the focus is now turning to TECOS, a trial with sitagliptin scheduled for completion in 2014, and CAROLINA, which is scheduled for completion in 2018. Together, these studies will provide the largest body of evidence on CV safety for any class of antidiabetic drug and will be helpful for guiding therapeutic decisions in long-term glycemic control for patients with type-2 diabetes.