Gastroenterology
United European Gastroenterology Week (UEGW) 2013
Beyond TNF Inhibitors for IBD: New Safety and Efficacy Data Move Adhesion Factor Inhibitors Forward
Berlin – New biologics are poised to expand treatment options for inflammatory bowel disease (IBD). Although only one agent for which new data were presented at the 2013 United European Gastroenterology Week (UEGW) has demonstrated efficacy and safety in extensive clinical testing, several in clinical trials show promise. Together, the data generated by these agents demonstrate that mediators of inflammation other than tumor necrosis factor (TNF) provide effective targets for therapy in IBD. The relative anti-inflammatory effect provided by inhibition of alternative molecular targets may or may not exceed that of TNF inhibitors, but the major advantage of new biologics may be more localized activity in the gut, reducing risk of systemic adverse events.
Long-term Data Validate Safety and Localized Activity
Data presented at the 2013 United European Gastroenterology Week (UEGW) on two adhesion factor inhibitors and an anti-interleukin 23 (IL-23) antibody predict a significant expansion of biologics for the control of IBD. Newly presented 2-year safety data with one of the adhesion factor inhibitors, vedolizumab, which had completed phase 3 trials in both Crohn’s disease (CD) and ulcerative colitis (UC), reinforced the safety observed over shorter periods.
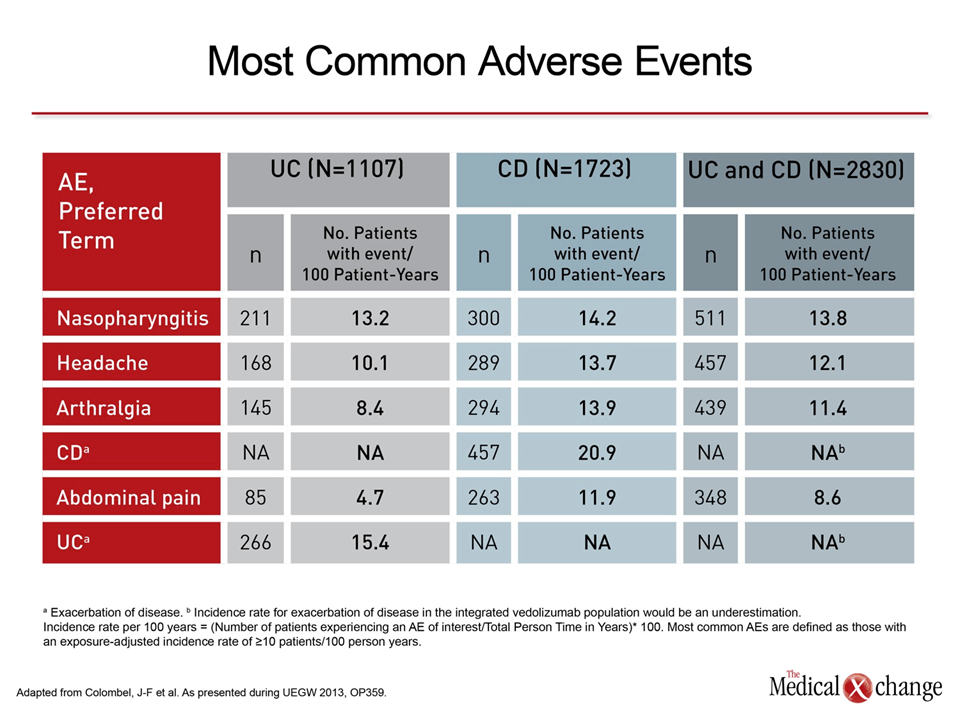
“We are still seeing low rates of serious adverse events (AEs) and no red flags for safety issues when patients are followed long-term,” reported Dr. Jean-Frederic Colombel, Chairman, IBD Center, Icahn School of Medicine at Mount Sinai, New York, NY. Pooling data from 1107 patients participating in phase 3 CD studies and 1723 patients participating in phase 3 UC trials, Dr. Colombel reported that the three most common AEs and their incidences were nasopharyngitis (13.8%) headache (12.1%) and arthralgias (11.4%) (Table 1). In this dataset the median duration of exposure is 1 year.
The low rate of AEs overall and serious AEs in particular is consistent with the presumed localization of activity in the gut. Adhesion factors, also known as integrins, are critical for bringing inflammatory cells to their site of activity. Both vedolizumab and etrolizumab, another adhesion factor inhibitor for which phase 2 data were presented at UEGW, have been designed to target those integrins specific to the gut. Although vedolizumab and etrolizumab may differ in other respects, both selectively block the α4β7MAdCAM-1 complex, which is known to mediate leukocyte homing to the intestine. Specificity to the gut was not shared by natalizumab, another integrin inhibitor, with very limited use because of concern about progressive multifocal leukoencephalopathy (PML).
The long-term safety data presented at UEGW with vedolizumab continue to validate this specificity of action. Dr. Colombel noted that more than 900 patients have now remained on vedolizumab for at least 2 years. There have been no cases of PML. There have also been low rates of other serious AEs, including other immune-related events, such as infection. Although similar conclusions cannot yet be drawn from the experience with etrolizumab, a placebo-controlled phase II trial with 124 patients also indicated no serious safety concerns. At UEGW, a substudy of the phase II etrolizumab study confirmed activity localized to the intestine and reinforced plans for clinical development.
“The evidence of targeted binding provides a proof of concept for the mechanism of action. Along with the evidence of activity and the tolerability profile, the data to date supports a phase 3 trial program,” reported Dr. Séverine Vermeire, University Hospitals, Leuven, Belgium.
The localized activity of adhesion factor inhibitors does not appear to diminish the high rates of remission that has been characteristic of biologics, judging from a study with vedolizumab that specifically evaluated steroid-free remissions among UC patients participating in the phase 3 trial program. A new analysis of the placebo-controlled trials GEMINI 1, performed in UC patients, and GEMINI 2, performed in CD patients, demonstrated that this rigorous criterion of benefit was frequently sustained.
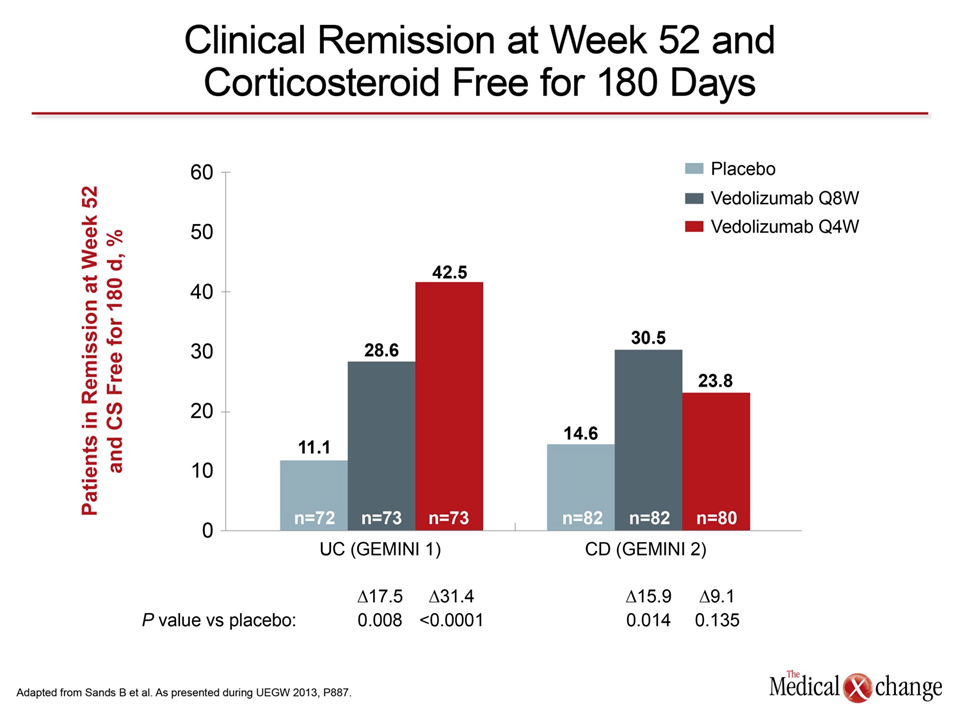
“The proportion of patients in remission at 52 weeks and steroid-free for at least 180 days was significant relative to placebo and is encouraging relative to other active agents” reported Dr. Bruce E. Sands, Director, Pediatric IBD Center, Icahn School of Medicine at Mount Sinai, New York, NY. Typical of IBD, steroid-free remission rates were greater in UC than in CD, but activity in both was favorable. In the UC group, 42.5% of patients treated with the every-four-week (Q4) dose, were both steroid free for at least 180 days and in clinical remission at 52 weeks (Fig. 1).
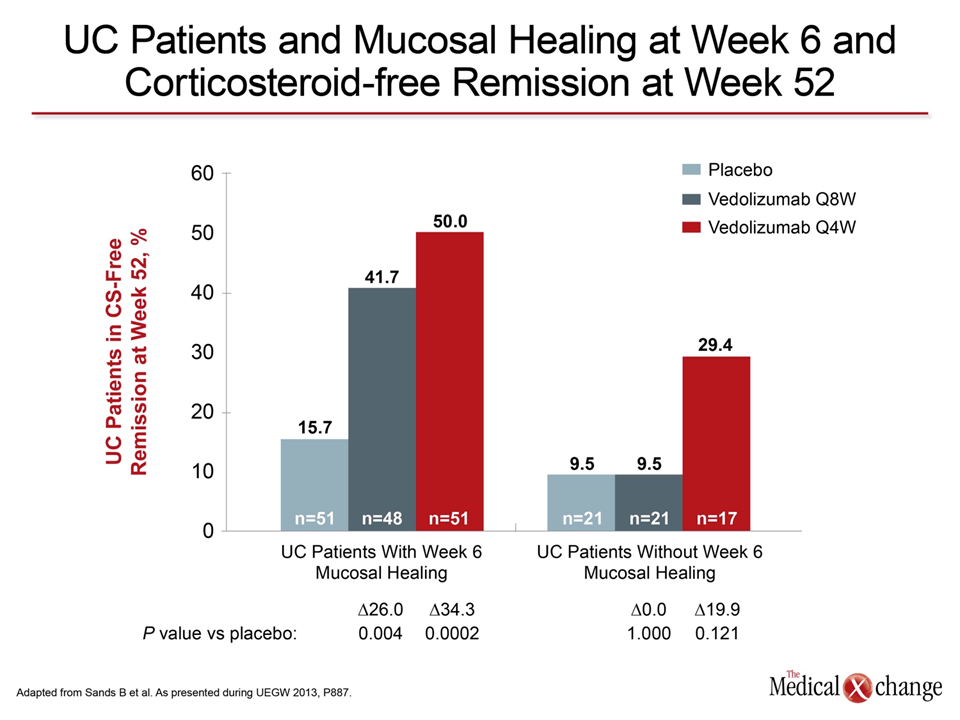
Ad-hoc analyses of these data suggest rapid response is a predictor of long-term benefit. In those on the Q4 regimen in GEMINI 1, 50% of those who achieved mucosal healing at 6 weeks, vs. 29.4% of those who did not, were in steroid-free remission at 52 weeks (Fig. 2).
Other molecular targets to halt the inflammatory response are also being pursued, including the pro-inflammatory cytokine IL-23. Again, the goal is to achieve an anti-inflammatory effect at least equal to that of TNF inhibitors but with a more favorable AE profile. In preliminary clinical data on the safety and efficacy of AMG139, a human monoclonal anti-IL-23 antibody that has entered phase 2 trials for CD, improvements in the Crohn’s Disease Activity Index (CDAI) was accompanied by reduction in C-reactive protein (CRP) with no serious AEs observed.
“The data so far have been promising and support a clinical trials program in CD as well as other inflammatory diseases, such as psoriasis,” reported Dr. Philip Miner, Oklahoma Foundation for Digestive Research, Oklahoma City, OK.
Conclusion
It is likely that anti-TNF agents will soon be joined by other biologics that target other molecular mediators of the inflammatory response. One such agent, the anti-integrin agent vedolizumab, has completed phase 3 trials with evidence of a low risk of serious AEs with a substantial number of patients on long-term therapy. One potential advantage of some of the newer agents is highly localized activity in the intestine, thereby avoiding systemic risks.