rheumatology
2013 ACR/ARHP Annual Meeting
Frequency at which Target Serum Urate Levels Are Missed in Gout is Prompting Strategy Modifications
San Diego – The increasing burden of gout in Canada as in other countries where prevalence is growing will be exacerbated if clinicians do not improve the rates at which urate-lowering therapies are optimized. The guideline-recommended target for serum urate is ≤ ~360 mmol/L (6 mg/dL), but even lower levels may be appropriate in patients with frequent flares. In data presented at the 2013 ACR/ARHP meeting, evidence of a rising prevalence of gout was joined by studies demonstrating significant differences in the rates at which serum urate targets are reached with commonly-used preventative therapies. By itself, gout alone was associated with a 50% increase in the risk of emergency room visits in one survey, but gout with tophi more than doubled the rate after adjusting for co-morbidities. These figures underline the importance of initiating a strategy with the greatest likelihood of reaching target serum urate levels once the acute attack of gout is controlled.
Are Current Target Goals Enough?
In Canada, as elsewhere with aging populations and a rising rate of obesity, the prevalence of gout is rising rapidly, but the burden to the healthcare system could be greatly reduced simply by optimizing urate-lowering therapies (ULTs). After an initial symptomatic flare, most patients will have recurrences, making preventive therapies essential even when lifestyle changes are used to lower risk.
“Despite currently available ULTs, more than 50% of all patients with gout do not attain the treatment goal,” reported Dr. Puja Khanna, Division of Rheumatology, University of Michigan, Ann Arbor. Referring to a target serum urate level of ≤ ~360 mmol/L (6 mg/dL), which has been endorsed by both the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR), Dr. Khanna suggested that even this target may not be sufficiently rigorous in those with tophi or frequent flares, which are associated phenomena. Several experts have proposed a target of ≤ ~300 mmol/L (5 mg/dL) in high-risk individuals.
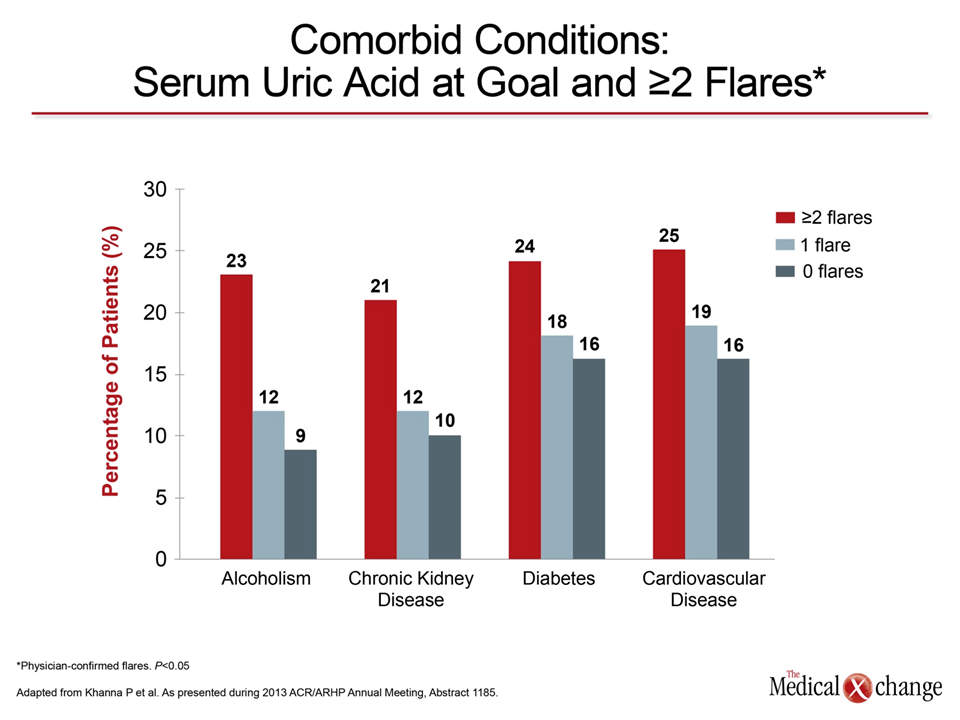
“In our chart review of 2,505 patients, approximately one-third of patients who did achieve the guideline-recommended serum urate target had 2 or more flares over a 12-month period,” Dr. Khanna reported. “Patients reaching the serum urate goal of 6 mg/dL [~360 mmol/L] or less and having two or more flares per year were more likely to have tophi, kidney disease, and other comorbid conditions [Fig. 1], but the data suggest that more attention needs to be paid to the adequacy of treatment response.”
Serum Urate Levels, Renal Impairment and Preventing Further Dysfunction
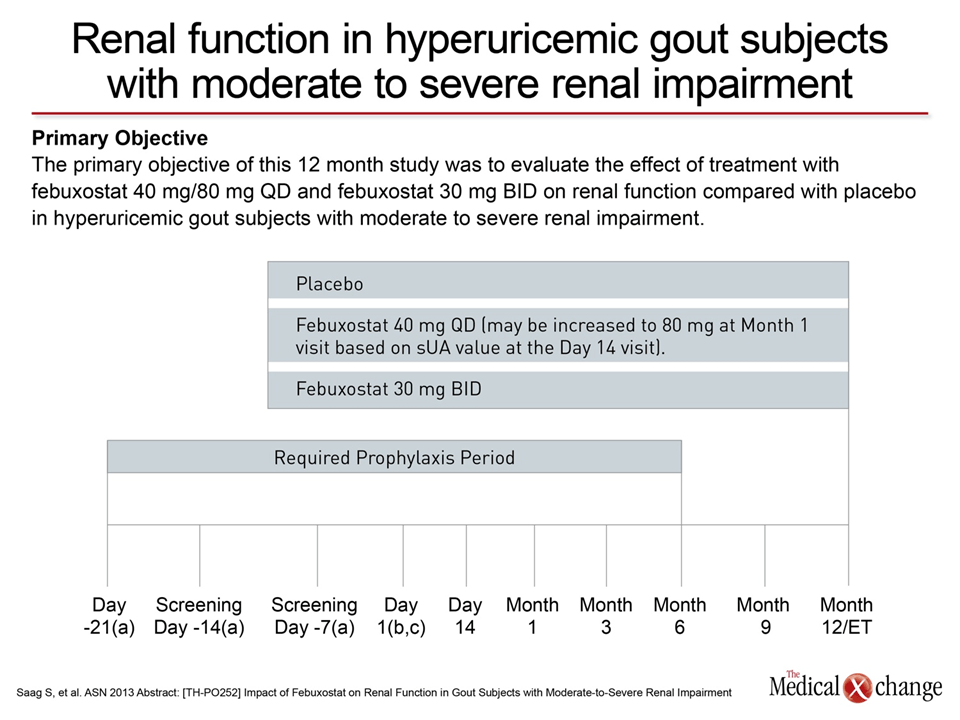
There are a large number of conditions that predispose patients to gout, including metabolic syndrome and hypertension, but decreased renal elimination of uric acid is a factor in the majority of cases. While uricosuric agents such as probenecid were once widely used for gout, the xanthine oxidase inhibitors (XOI) allopurinol and febuxostat have proven more versatile by providing reductions in serum urate across etiologies. This includes activity in patients with moderate-to-severe renal impairment, an activity confirmed in a placebo-controlled trial presented at this year’s ACR/ARHP meeting with the XOI febuxostat.
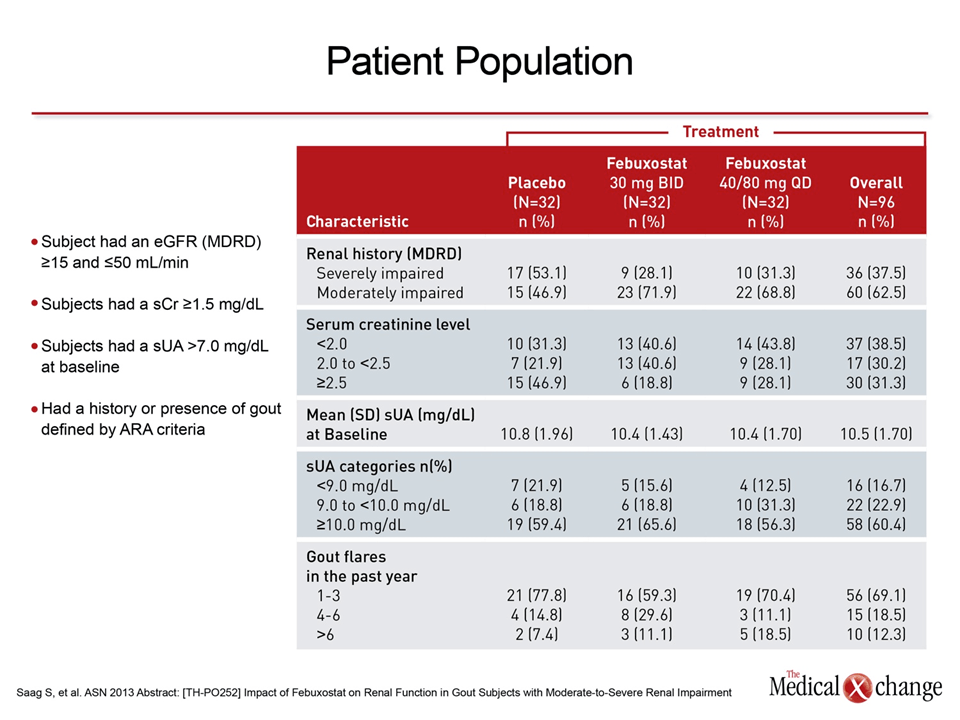
In that multicenter, double-blind trial, 96 patients were randomized to one of three groups: febuxostat 30 mg twice daily (BID); an up-titrated, febuxostat once-daily (QD) regimen, starting at 40 mg and increasing to 80 mg; or placebo. The mean serum urate at baseline was ~625 mmol/L [10.5 mg/dL]. At entry, all patients had an estimated glomerular filtration rate (eGFR) <50 mL/min/1.73 m2, of which about one third had an eGFR <15 mL/min/1.73 m2. The primary endpoint was a serum urate < ~360 mmol/L [6.0 mg/dL].
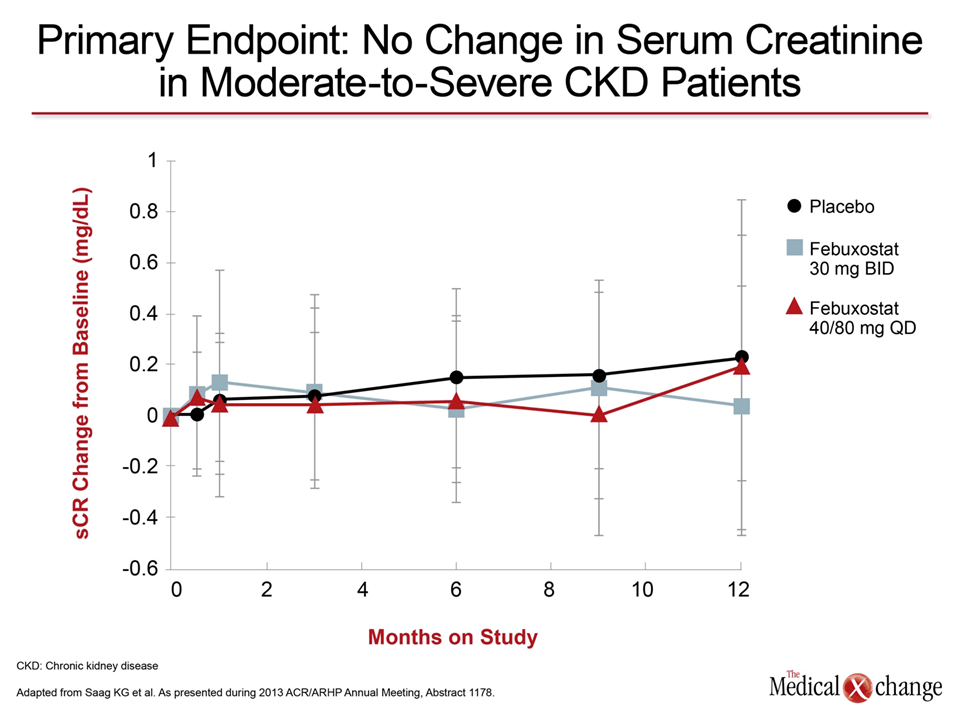
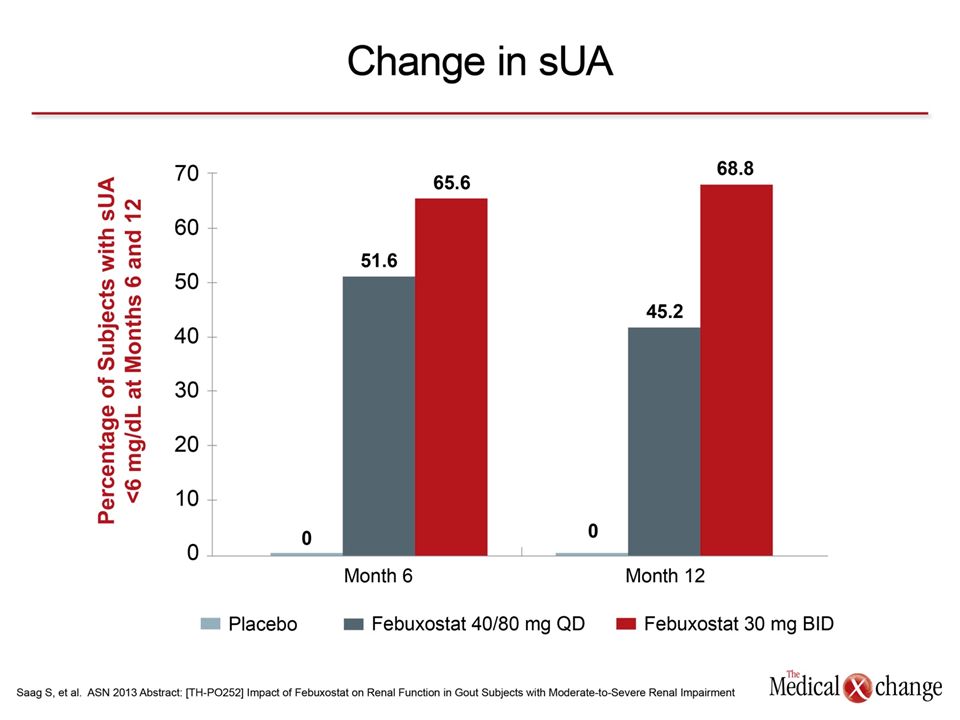
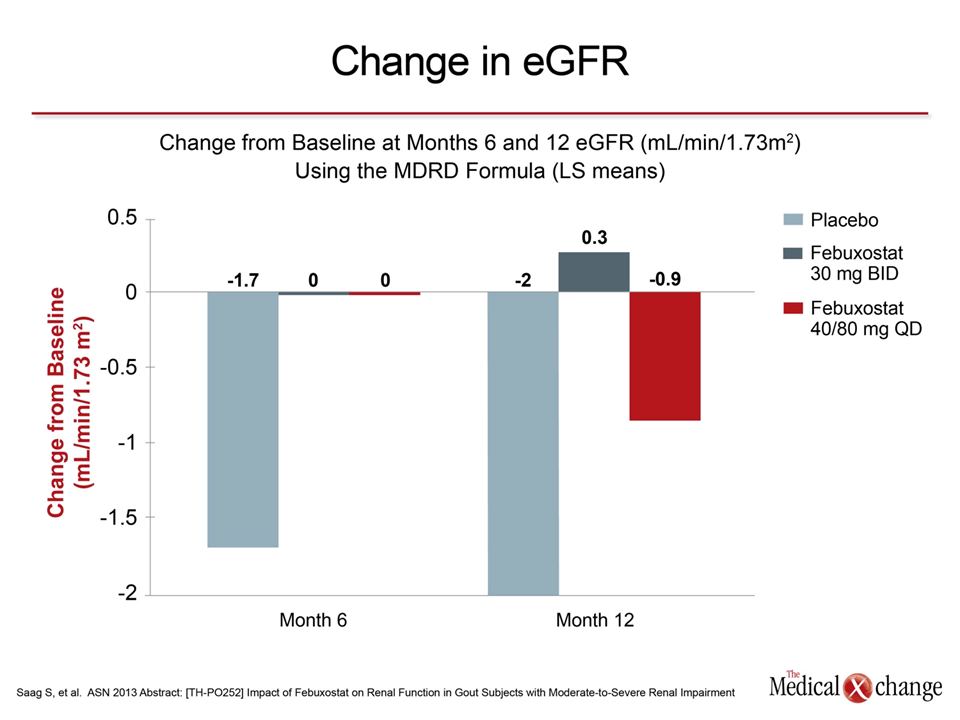
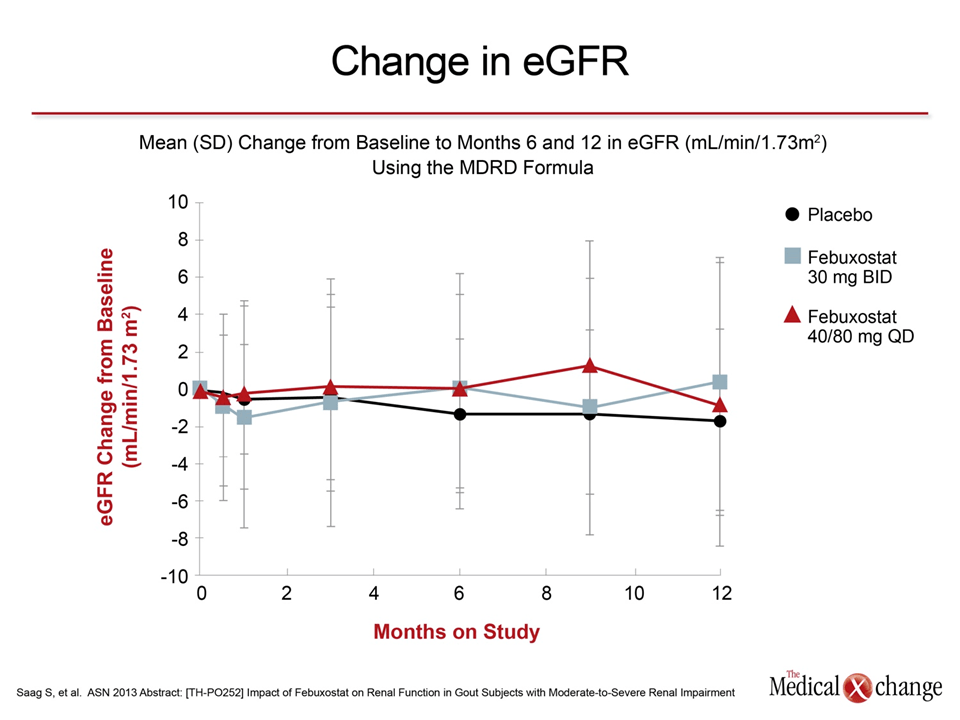
At the end of 12 months of therapy, the proportion of patients who reached the primary endpoint was 0% in the placebo group, 69% (P<0.001 vs. placebo) in the group randomized to 30 mg febuxostat BID and 45% (P<0.001 vs. placebo) in the group randomized to the febuxostat 40/80 mg QD dose. The mean eGFR at the end of 12 months in the three groups was not changed (Fig. 2), but there was a remarkable consistency of effect when mean serum urate levels at 6 and 12 months were compared.
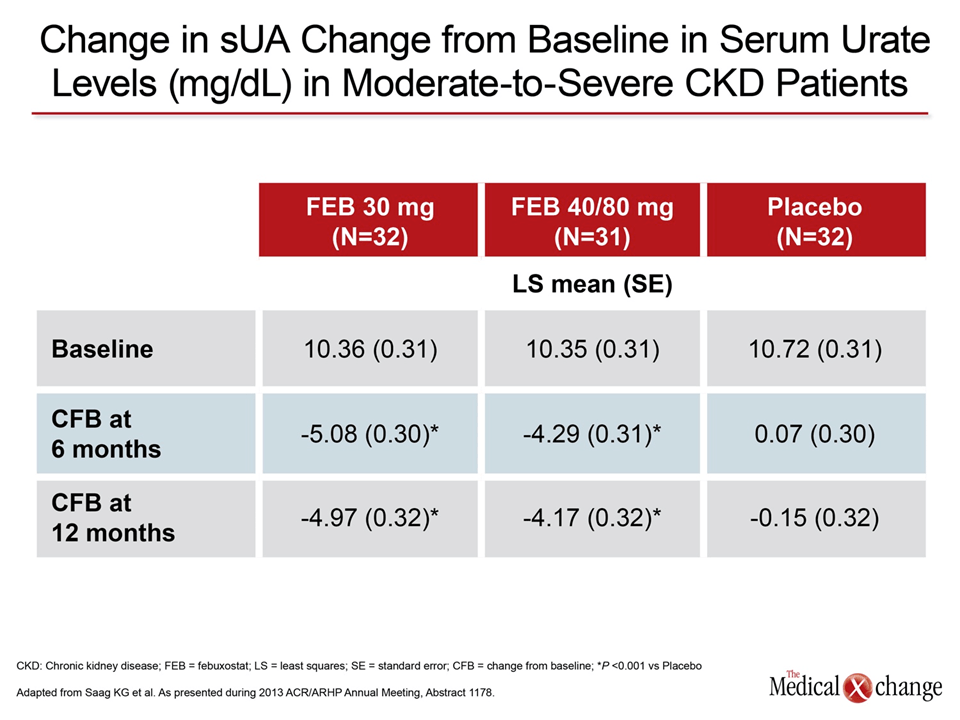
“When 12 months were compared to 6 months, the mean reductions from baseline in the serum urate levels with either the 30 mg (~296 vs. ~302 mmol/L [4.97 vs. 5.08 mg/dL]) and 40/80 mg (~261 vs. ~248 mmol/L [4.39 vs. 4.17 mg/dL]) doses were very similar,” reported Dr. Kenneth Saag, Birmingham VA Medical Center, Alabama (Table 1). These data reinforce other evidence that febuxostat produces a sustained urate-lowering effect even when renal impairment is severe.
Control of serum urate levels may not only be important for reducing gout but also for avoiding further decline in renal function.
In patients with renal impairment, control of serum urate levels may not only be important for reducing gout but also for avoiding further decline in renal function, according to a separate set of data presented at the ACR/ARHP. In that retrospective analysis of 16,186 patients with serum urate levels > ~416 mmol/L [7.0 mg/dL], keeping serum urate levels < ~360 mmol/Lwas associated with a 37% reduction in having a 30% or greater reduction in eGFR or progressing to an eGFR <15 mL/min/1.73 m2. While diabetes, cardiovascular disease, and a high serum urate level prior to treatment were among factors that predicted this degree of progression in renal impairment, the protective effect of optimized urate-lowering therapy was highly significant (P<0.0001).
“Being at goal was highly protective against progression of renal dysfunction when compared to not being at goal, suggesting another important reason to reach guideline-based targets,” reported Dr. Gerald D. Levy, Kaiser Permanente Downey Medical Center, California.
In that retrospective study, a chart review demonstrated that the majority of patients were treated with allopurinol, which has long been a first-line therapy in the prevention of gout recurrences. Of note, the 2012 ACR guidelines list both allopurinol and febuxostat as first-line ULTs. At many centers, febuxostat has been reserved as an alternative to generic allopurinol, but this strategy was challenged by two analyses conducted with a large electronic medical records (EMR) database. Presented at this year’s meeting by Dr. Khanna, one compared the agents in naïve patients and the other evaluated outcomes when patients were started with allopurinol and switched to febuxostat.
The EMR used for both studies included data on 18,389 gout patients from 1200 U.S. healthcare systems. In the study focusing on the effect of these therapies in naïve patients, 42.2% of the febuxostat group vs. 29.2% of the allopurinol group (P<0.05) achieved the serum urate goal of ≤ ~360 mmol/L. At 2 years, the advantage for febuxostat remained significant (58.2% vs. 48.2%; P<0.05). This difference was observed even though a higher proportion of febuxostat patients (46.4% vs. 34.7%) had renal impairment defined as eGFR <60 mL/min/1.73 m2 at the time therapy was initiated, which appears to reflect a preference of this agent by clinicians in the event of renal dysfunction.
“The data from this real-life study suggest that a greater proportion of patients achieve the guideline-based urate goals on febuxostat,” Dr. Khanna reported. Overall, the odds ratio (OR) of achieving ≤ ~360 mmol/Lwas 1.725 (95% CI 1.480 – 2.012) for febuxostat relative to allopurinol after controlling for age, comorbidities, gender, race, and presence of tophi.
In the other study, the same database was used to evaluate whether similar control of serum urate is achieved when switching to febuxostat after initiating therapy with allopurinol vs. starting therapy with febuxostat. In the study cohort, 16,366 patients were identified who started and remained on allopurinol, 884 who started and remained on febuxostat, and 505 who started on allopurinol and switched to febuxostat when the serum urate goal of ≤ ~360 mmol/Lwas not achieved.
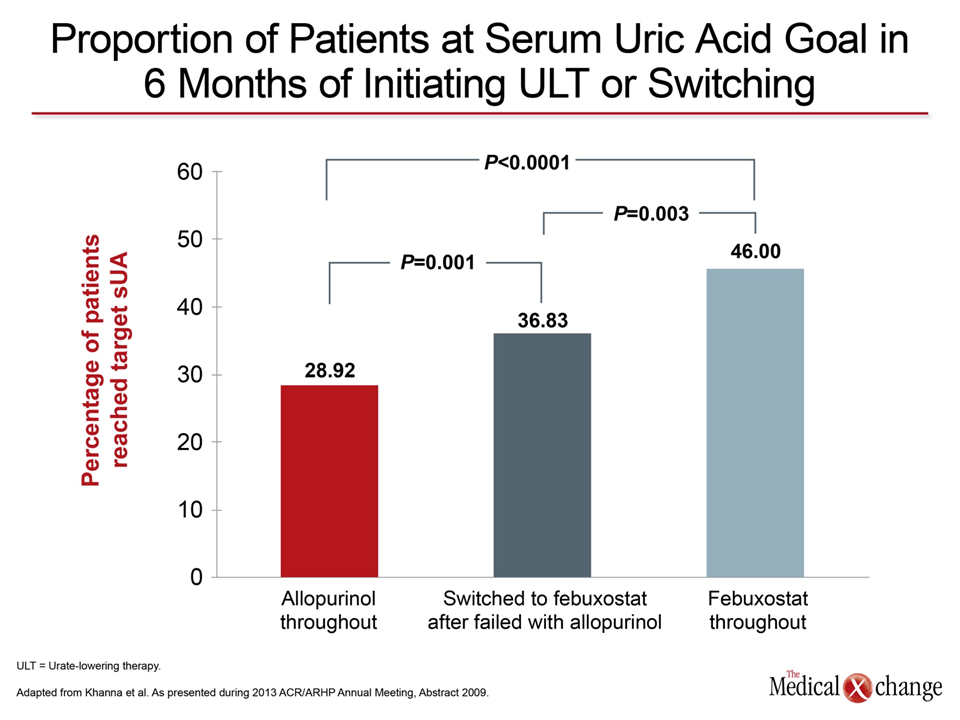
“The proportion of allopurinol-switched-to-febuxostat patients who reached the target serum urate level was significantly higher than that among the allopurinol-throughout patients [36.8 vs. 28.9%, P=0.001]. However, this proportion was significantly lower than that observed among the febuxostat-throughout patients [36.8% vs. 46.0%, P=0.003],” Dr. Khanna reported (Fig. 3).
Efficacy, Quality of Life in Patients with Tophi
Relative efficacy may be of particular concern in patients with tophi, according to data drawn from the Consortium of Rheumatology Researchers of North America (CORRONA) gout registry and presented at this year’s meeting. In this analysis of 524 gout patients enrolled in the database by 54 rheumatologists, 116 had tophi and 408 did not. When compared, those with tophi had more comorbidities, particularly chronic kidney disease (29% vs. 14%; P=0.001), were less likely to have a serum urate level ≤ ~360 mmol/L, and more likely to have flares even when serum urate levels were at the guideline-recommended target.
“Although 58% of patients with tophi had a serum urate level ≤6 mg/dL [~360 mmol/L], the average number of flares in the previous 12 months was four,” reported Dr. Leslie R. Harrold, Division of Rheumatology, University of Massachusetts School of Medicine, Worcester. In such patients, Dr. Harrold suggested that lower serum urate levels may be appropriate. In the CORRONA registry, 39% of patients with tophi had a serum urate level ≤ ~300 mmol/L, which seemed to confer greater protection against flares, although the small numbers in this study prevented meaningful comparisons.
The need to increase the rates at which guideline-recommended serum urate goals are reached, and to consider even lower goals in those at high risk of flares, is emphasized by the large healthcare burden incurred by gout. In data from the 2012 U.S. National Health and Wellness Survey (NHWS) presented here, gout was associated with large increases in healthcare utilization, particularly when therapy was inadequate.
“By raw numbers, patients with gout had 1.5 times as many emergency room visits than patients without gout. Among those with self-reported tophi, the OR of an emergency room visit was increased 2.5-fold,” reported Dr. Javinder A. Singh, Division of Rheumatology, University of Alabama, Birmingham. “In-patient hospitalization was also higher in those with gout compared to those without.”
In the NHWS, which is a nationally-representative online survey with data on 71,157 individuals, the 1,347 with a diagnosis of gout and on therapy were compared both to the 69,161 patients without gout and to the 649 patients with gout but not taking treatment. The mean time since diagnosis was 12.3 years with 52% reporting mild gout, 33% moderate gout, and 15% severe gout. While those with gout had far greater rates of comorbidities relative to those without, it is notable that both the mean average mental (43.5 vs. 50.7; P<0.05) and physical (39.0 vs. 44.7; P<0.05) quality of life scores, as captured on the Short Form 36 (SF-36) questionnaire were significantly lower in those with tophi.
Conclusion
The prevalence of gout is increasing in Canada and many other areas of the world where rates of obesity are climbing in an aging population. The first-line defense against the public health burden is lifestyle changes that lead to weight reduction and avoidance of risk factors, such as excessive alcohol intake. However, in those who develop an initial flare, the risk of recurrent flares is high, indicating a need for pharmacological agents to bring serum urate levels to the current guideline-recommended level of ≤ ~360 mmol/L [6 mg/dL]. Optimizing therapy to reach this goal has implications not only for quality of life but also for reducing complications and reducing healthcare utilization.
Additional Slides
Figures 4 (Fig. 4), 5 (Fig. 5), 6 (Fig. 6), 7 (Fig. 7), 8 (Fig. 8) and 9 (Fig. 9).