gastroenterology
Digestive Disease Week (DDW) 2014
Bile Acid Malabsorption Proves to Be Surprisingly Frequent Source of Readily Reversible Chronic Diarrhea
Chicago – Bile acid diarrhea is often misdiagnosed. According to data presented at the 2014 Digestive Disease Week, a substantial proportion of patients with bile acid diarrhea receive a series of misdirected therapies for other conditions, such as irritable bowel syndrome (IBS). Bile acid diarrhea is caused by bile acid malabsorption, a condition with a broad range of etiologies that results in disturbances in water and sodium transport in the gastrointestinal (GI) tract. Although the underlying causes of bile acid malabsorption are not always easy to reverse, bile acid sequestrants are effective for controlling the diarrhea. The value of considering bile acid malabsorption as a cause of chronic diarrhea is an essential first step toward implementing effective therapy. Studies at DDW focused attention on a persistent but reversible problem.
Bile Acid Malabsorption is Often Overlooked
Bile acid diarrhea is common. It can arise from one of several gastrointestinal (GI) diseases or from pharmacological agents or surgical procedures, such as cholecystectomy, that result in excess amounts of bile acid reaching the colon. The major consequence of spilling bile acids into the lower GI tract is a prosecretory effect, but other mechanisms may be involved, including an acceleration of GI motility and mucosal injury. For clinicians, the key is remembering to consider bile acid malabsorption as a major cause of diarrhea among patients with this complaint.
“Bile acid malabsorption is quite common. In adults, the estimated prevalence is somewhere around 1%”.
“Bile acid malabsorption is quite common. In adults, the estimated prevalence is somewhere around 1%,” reported Dr. Julian R. F. Walters, Professor of Gastroenterology, Imperial College, London, UK. Citing disease burden data from the UK, Dr. Walters, whose presentation at this year’s DDW was focused on differences between bile acid malabsorption and the diarrhea subtype of irritable bowel syndrome (IBS-D), emphasized that this “is a prevalence that is somewhat greater than that of celiac disease or Crohn’s disease even though we see far less attention to this problem.”
The impetus for drawing attention to bile acid diarrhea is that it is often missed even though it is relatively easy to control. According to Dr. Walters, bile acid sequestrants are the mainstay of therapy and have a straightforward mechanism. By binding to bile acids, these agents prevent free bile acid from reaching the colon to exert prosecretory effects. Cholestyramine, colestipol, and colesevelam represent the three available bile acid sequestrants, but these may not be interchangeable. Many of the clinical trials demonstrating benefit have been conducted with cholestyramine, which is the only sequestrant with an indication for the control of bile acid diarrhea in many countries. In Canada, the specific indication for cholestyramine is symptomatic control of bile acid induced diarrhea due to short bowel syndrome.
SeHCAT Test or Empirical Dose Titration?
“A lot of the work, including many of the empirical treatment trials, has been conducted with cholestyramine,” reported Dr. Walters. Such studies have been typically conducted in patients with bile acid malabsorption established with the SeHCAT test, a sensitive tool for confirming this cause. SeHCAT employs a radiolabeled taurine-conjugated bile acid analog to demonstrate impaired bile acid retention.
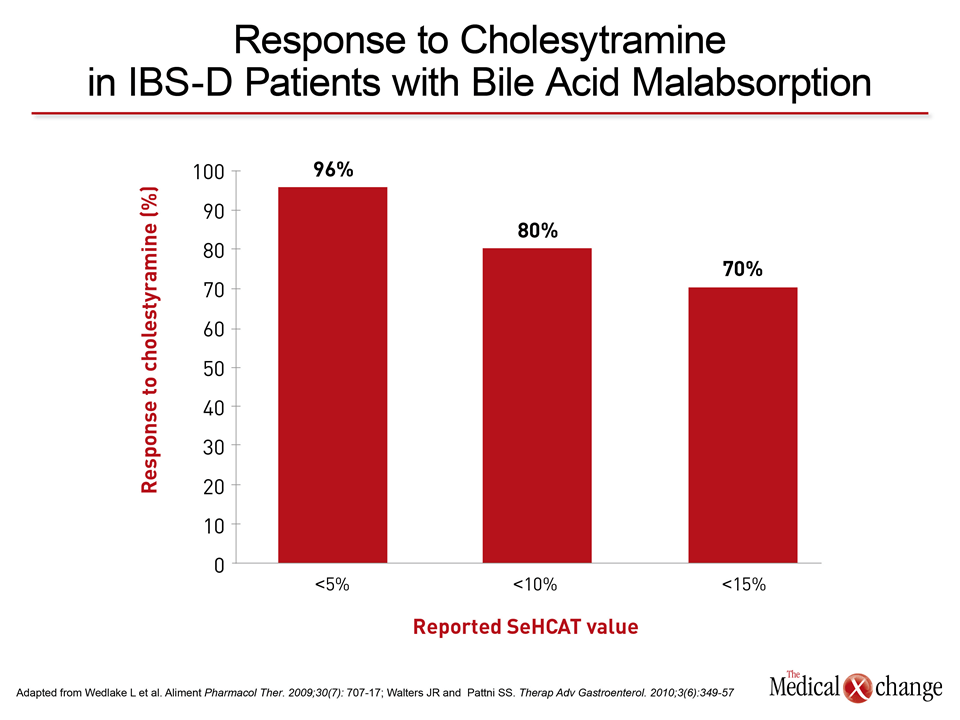
The weakness of SeHCAT, which requires a gamma camera analysis, is that it is not uniformly available. C4 liquidchromatography, which is less sensitive, is an alternative but, like SeHCAT, may also be difficult to order. Fecal stool assays, the gold standard for detection of bile acid malabsorption, are less expensive but poorly accepted by patients, who must collect the samples. For a more practical approach, many experts, including Dr. Walters, suggest that an empirical course of a bile acid sequestrant, which directly reverses the mechanism of bile acid diarrhea, is a reasonable approach to diagnosis, particularly when the index of suspicion is high for the presence of bile acid malabsorption. In an analysis of 15 published trials cited by Dr. Walters (Wedlake L et al. Aliment Pharmacol Ther 2009;30:707-17), response to cholestyramine was 70% with a SeHCAT retention cut-off of <15%, 80% with a cut-off of <10%, and 96% with a cut-off of <5% (Fig. 1).
The dose-response relationship between the severity of bile acid diarrhea and response to cholestyramine speaks to the efficacy of bile acid sequestration, but Dr. Walters cautioned that there is interpatient variability in response by time and dose. In some patients initiated on a standard dose of cholestyramine, which is widely considered to be 4 g twice per day, response is relatively prompt with good symptom control within a day or two of initiating therapy. In others, symptoms may diminish more slowly and higher doses will be required to achieve adequate control. In difficult cases, uncertainty can be avoided by using one of the objective diagnostic tests, but Dr. Walters encouraged empirical dose titration whether bile acid sequestrants are used as a test or treatment to achieve an optimal response. The powder formulation of cholestyramine, relative to fixed-dose pills or capsules of alternative bile acid sequestrants, is particularly versatile for dose adjustments needed to confirm the diagnosis or adjust response.
Bile Acid Malabsorption and Diverse Causes of Chronic Diarrhea
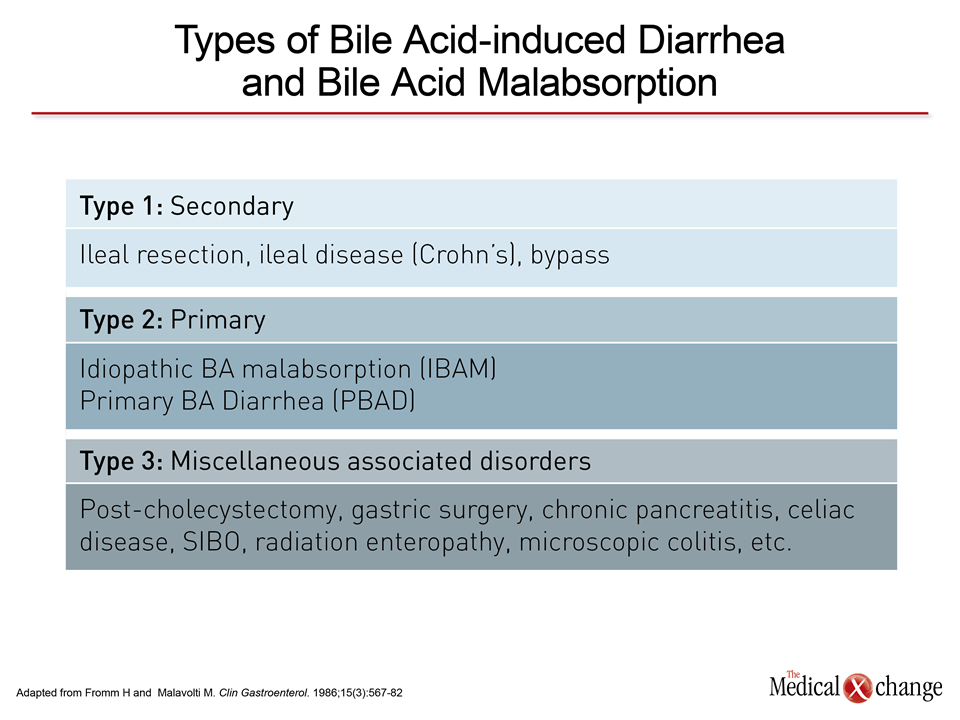
The data establishing bile acid malabsorption as one of the most common underlying causes of chronic diarrhea are abundant. One reason is that bile acid malabsorption often occurs in the absence of any known etiology. This idiopathic formis classified as type 2, which is distinguished from ileal resection or ileal diseases, such as Crohn’s, that define type 1 and the broad list of alternative but known causes of excess bile acid in the colon that define type 3 (Table 1).
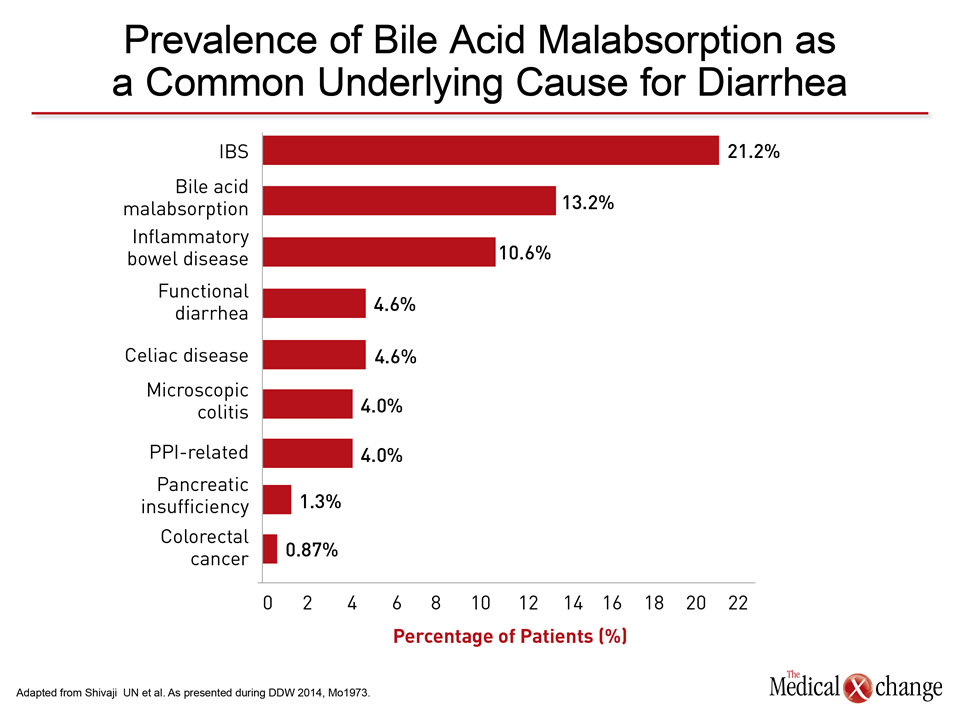
The data presented at the 2014 DDW underline the diversity of underlying causes of diarrhea associated with bile acid malabsorption. In a series of 613 consecutive referrals to a GI clinic of which 151 had chronic diarrhea, bile acid malabsorption, confirmed with the SeHCAT test, was the cause in 13.2%, making this the second most common cause of chronic diarrhea after IBS, which accounted for 21.2% of cases (Fig. 2).
“Bile acid malabsorption was a somewhat more common cause of chronic diarrhea than inflammatory bowel disease and about three times more common than functional diarrhea, celiac disease, or colitis,” reported Dr. Uday N. Shivaji, who led the study at the Leeds Gastroenterology Institute, Leeds, UK.
From the clinical perspective, it is noteworthy that no cause of bile acid diarrhea could be found in 65%. These were among data presented at DDW to encourage clinicians to consider disturbances in bile acid as a major cause of diarrhea even in the absence of a known cause of this problem.
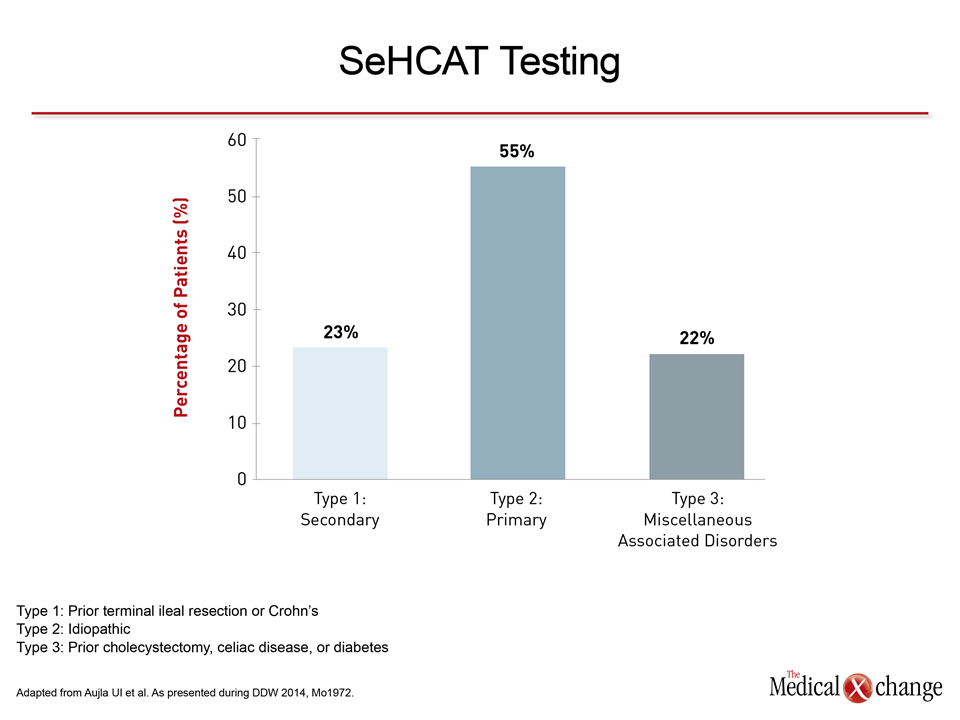
A second study in a series of 118 patients drew a similar conclusion. Of the 118 patients with chronic diarrhea evaluated with SeHCAT, 43% demonstrated bile acid malabsorption. All were treated with bile acid sequestrants with the majority achieving a good response. Again, IBS-D was more common, but the high rates of bile acid malabsorption underline the importance of giving this condition prominent consideration in a differential diagnosis.
In this study, 55% of patients had no known cause for the bile acid malabsorption and were thus classified as having type 2, 23% had type 1 disease defined by prior terminal ileal resection or Crohn’s, and 22% had type 3 disease defined by prior cholecystectomy, celiac disease, or diabetes (Fig. 3).
“Our data suggest that the label of IBS-D may be applied too often,” reported Dr. Usman I. Aujla, who was lead author of this study, which was conducted at the Epsom and St. Helier University Hospitals, both located in London, UK. “Our data are consistent with a substantial body of evidence that bile acid malabsorption is not uncommon in an unselected series of patients with chronic diarrhea.”
The premise of much of the data presented on chronic diarrhea due to bile acid malabsorption is that this condition should be considered even in the absence of a history that would suggest a mechanism for excess excretion of bile acids into the colon. However, even many of those with chronic diarrhea due to type 1 and 3 forms of bile acid malabsorption may also be missed. Due to the large number of etiologies for bile acid diarrhea, many can be overlooked. In new data presented at DDW 2014, attention was drawn to the risk of bile acid diarrhea from treatments of cancer.
Implications of Cancer
“There have been several published reports of radiation-related bile acid diarrhea, but data we have collected suggests that bile acid malabsorption is a more common problem in cancer patients than previously understood and that the malabsorption is due to diverse causes,” reported Dr. Frank Phillips, Royal Marsden Hospital, London, UK.
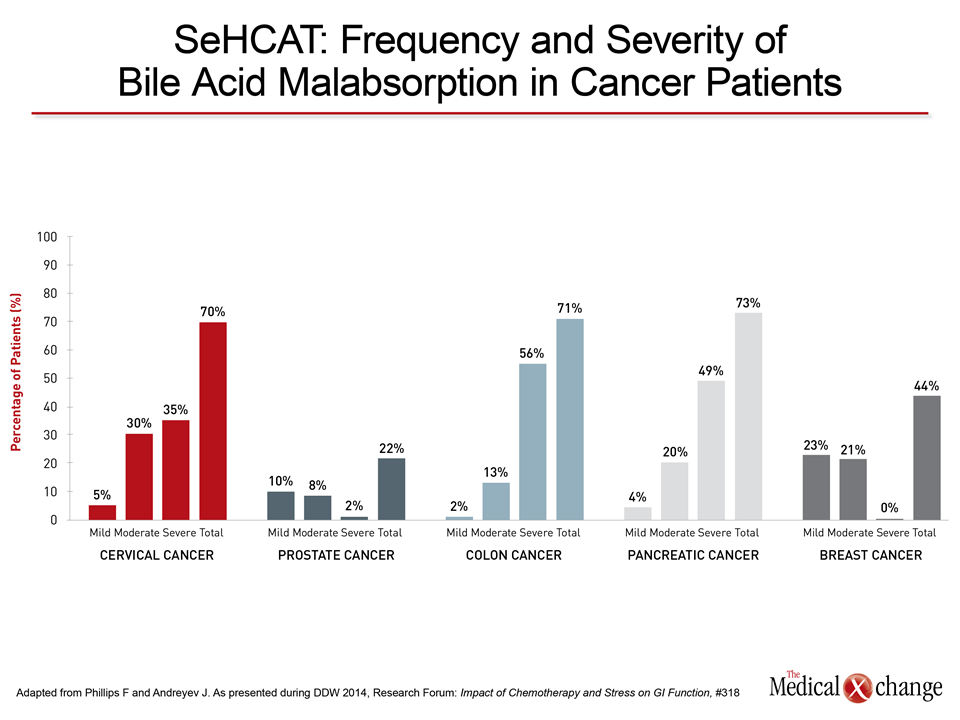
In a retrospective analysis of 506 consecutive cancer patients with chronic diarrhea referred for SeHCAT, the proportion of those found to have bile acid malabsorption ranged from 22% in prostate cancers to 70% in patients with myeloma, cervical, colon or pancreatic cancers (Fig. 4). The differences were attributed to the treatments and their potential to affect bile acid metabolism. For example, high rates were observed in myeloma because one of the most commonly used therapies, lenalidomide, adversely impacts bile acid retention.
“We consider this a landmark study because it establishes bile acid malabsorption as a very frequent cause of diarrhea secondary to cancer treatments,” Dr. Philips reports. In this study, which stratified SeHCAT by severity, the majority of patients in some cancer groups, such as colon and pancreatic cancer had the most severe form of bile acid malabsorption whereas others, such as breast cancer, had more mild forms of bile acid malabsorption. Based on these data, bile acid malabsorption should be given strong consideration as a possible cause in cancer patients presenting with chronic diarrhea, according to Dr. Phillips. In many of these patients a trial of bile acid sequestrants may be the least expensive and easiest strategy for diagnosis although objective tests should be considered when response is incomplete even after dose adjustment.
Conclusion
Bile acid malabsorption is a major but under-recognized cause of chronic diarrhea. While there are many causes of bile acid malabsorption, surveys suggest that most cases are idiopathic. This may explain assertions from experts that patients with chronic diarrhea due to this cause are being frequently misdiagnosed with IBS-D. Unlike IBS-D, for which therapeutic options remain limited, chronic diarrhea due to bile acid malabsorption can be controlled with bile acid sequestrants, the first-line therapy. Earlier consideration of bile acid malabsorption as a cause of chronic diarrhea has important implications for improved outcomes.