gastroenterology
Digestive Disease Week (DDW) 2014
New Data from IMAgINE 1 Trial Provide Insights on Biologic Use in Pediatric Crohn’s Disease
Chicago – A series of new analyses drawn from the IMAgINE 1 trial have generated insight on how best to employ biologic therapy in children with Crohn’s disease. In new data presented at the 2014 DDW on IMAgINE 1, which randomized 192 children from age 6 to 17 years to a standard or low-dose regimen of adalimumab, concomitant immunologic modulators were not found to improve clinical remission rates, once-weekly dosing was often effective when every-other-week dosing was not, and higher doses of adalimumab led to higher rates of corticosteroid-free remission.
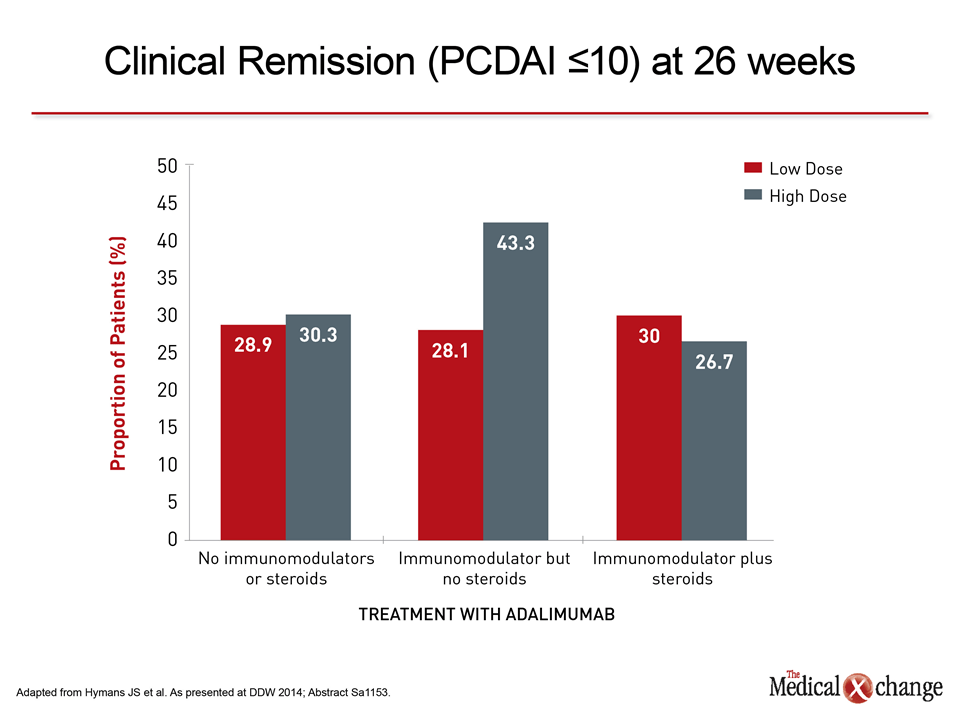
The primary results of IMAgINE 1, presented last year, showed that 39% of those on an every-other-week standard dose (20 mg in children 40 kg) versus 28% of those on low dose (10 mg or 20 mg for the two weight levels, respectively) were in clinical remission at the end of 26 weeks. In a new analysis of the effect of being on non-biologic immunomodulators at baseline, which was the case in about 60% of patients, the clinical remission rates for the high- and low-dose groups were 43.3% and 28.1%, respectively, which did not differ significantly from the rates for these groups seen in the absence of immunomodulators. “While concomitant use of non-biologic immunosuppressants did not affect the incidence of serious infections, it also did not appear to influence the remission rates,” reported Dr. Jeffrey S. Hyams, Connecticut Children’s Medical Center, Hartford. In this dataset, the investigators also looked at remission rates in patients taking immunomodulators with corticosteroids at baseline. In this group, the remission rates at 26 weeks were 26.7% and 30% for the high- and low-dose adalimumab groups, respectively, but, again, this difference was not significantly different than that observed from the overall response rates (Fig. 1). However, once-weekly treatment with adalimumab does appear to increase rates of response. In IMAgINE 1, 83 of the 188 patients moved to weekly dosing, a step more common in those who started treatment on a low dose or who had more severe disease at the start of the study. Slightly more of those who were dose escalated had been treated prior to IMAgINE 1 with infliximab (47% vs. 41.9%). At 52 weeks, 18.8% of those in the low-dose group and 31.4% of those in the high-dose group who were dose escalated were in remissions. “These data suggest that weekly adalimumab doing may be a beneficial treatment strategy for pediatric Crohn’s disease patients who do not achieve a desired response or experience a disease flare on every-other-week dosing, particularly as we did not observe any increased safety risks,” reported Dr. Maria Dubinsky, Cedars-Sinai Medical Center, Los Angeles, California. In a third IMAgINE 1 dataset presented at DDW 2014, the impact of baseline corticosteroid use on end-of-study corticosteroid-free remission rates was evaluated. Of the 188 patients, 38 in the low-dose and 33 in the high-dose groups were on corticosteroids when adalimumab was initiated. At week 26, 33.3% of high-dose and 26.3% of low dose patients had achieved corticosteroid-free remission. According to Dr. Anne M. Griffiths, Hospital for Sick Children, Toronto, Ontario, the rates of steroid-free remission were significantly higher in patients without prior infliximab use, but baseline disease severity was not found to be a significant predictor of steroid-free remission. Overall, the new data are consistent with the previous reports that adalimumab achieves high rates of remission in children with moderate to severe active Crohn’s disease with acceptable rates of adverse events. The new results expand the dataset, suggesting that benefits are observed across subgroups defined by prior and concomitant therapies.