ADHD
3rd EUNETHYDIS International Conference on ADHD
Consolidating Benefit with Newer Options for ADHD: Core Symptom Control in Large Trials
Istanbul – The efficacy of alternative therapies for the control of attention deficit hyperactivity disorder (ADHD) has been validated in a series of studies presented at the 3rd EUNETHYDIS Conference. Stimulant medications are the guideline-recommended first-line therapy for ADHD, but up to 30% of ADHD patients do not respond adequately to these agents, according to published studies and new data presented here. The alternatives for stimulants include a selective alpha-2a (α2a) receptor agonist and a selective norepinephrine reuptake inhibitor (SNRI). Each was associated with highly-significant reductions in the core ADHD symptoms of hyperactivity, inattention, and impulsivity in a series of large multicenter, placebo-controlled trials. The objective evidence included data specifically collected with the selective α2a receptor agonist in adolescents, a group that has not been uniformly included in previous ADHD studies with this agent. These new data outline an evidence-based strategy for improving ADHD control in those with symptoms despite optimized first-line therapy.
Not all ADHD Patients Achieve Adequate Response to First-line Therapy
A substantial subset of children with ADHD patients are not adequately controlled on first-line stimulants. According to previously-published estimates, up to 30% of individuals with ADHD do not achieve an adequate response to stimulants at acceptably-tolerated doses (Banaschewski T et al. Eur Child Adolesc Psychiatry. 2004; 13 (Suppl 1): S102-16). Similar data were reported here from the Caregiver Perspective on Pediatric ADHD (CAPPA) study. In this study, the proportion of ADHD children with substantial symptoms while taking stimulant therapy ranged from 13.8% to 36.4% on domains of the ADHD Rating Scale-IV (ADHD-RS-IV) hyperactive/impulsive subscale (Fig. 1).
“Caregivers overall report that first-line stimulant medications are effective, but there is clearly a subset of patients for whom adjunctive or alternative therapies are needed.”
“Caregivers overall report that first-line stimulant medications are effective, but there is clearly a subset of patients for whom adjunctive or alternative therapies are needed,” reported the CAPPA team of authors that included Dr. Javier Quintero, PhD, University Hospital Infanta Leonor, Madrid, Spain.
In the CAPPA study, 3688 caregivers in 10 European countries completed a survey that evaluated their perception of ADHD symptom control in children on and off medication. While caregivers reported that most children “often” or “very often” have symptoms of hyperactivity and inattention off medication, the substantial levels of symptoms occurring “often” or “very often” on medication support previous data that stimulants are not always sufficient for optimal ADHD control.
The underlying reasons to consider adjunctive or alternative agents are varied and “may be due to partial response or intolerance of stimulant side effects,” but the need for alternatives in such scenarios “is consistent with my experience.”
The issue is relevant in Canada, according to Dr. Judy van Stralen, an expert on ADHD at the Centre for Pediatric Excellence, Ottawa, Ontario. According to Dr. van Stralen, “there are patients who are unable to achieve optimal functioning on stimulants alone.” While noting that the effect size of stimulants is large and that the majority of patients do respond adequately to these drugs, she suggested that the underlying reasons to consider adjunctive or alternative agents are varied and “may be due to partial response or intolerance of stimulant side effects,” but the need for alternatives in such scenarios “is consistent with my experience.”
Latest Data: Focus on Adolescents
In Canada, both extended-release (XR) guanfacine and atomoxetine provide options to stimulants for the control of ADHD. Guanfacine XR is approved for children aged 6 to 12 years as an alternative monotherapy or adjunctive agent, and atomoxetine is approved for children 6 years old or older, adolescents and adults, as an alternative monotherapy agent. Several studies at EUNETHYDIS greatly expand evidence of benefit from guanfacine XR in adolescents, including a double blind, placebo-controlled trial limited to this age group. In this study, 314 ADHD patients aged 13 to 17 years with a baseline ADHD-RS-IV score of ≥32 and a Clinical Global Impression-Severity of Illness (CGI-S) score of 4 were randomized to 1 mg guanfacine XR or placebo. The dose of guanfacine XR was raised, if needed, to a maximum of 7 mg over a 7-week optimization phase. The primary endpoint was the reduction in ADHD-RS-IV score at the end of 13 weeks on therapy.
The mean change from baseline was about a 25-point reduction in the guanfacine XR group and a less than 20-point reduction in the placebo group, providing an absolute advantage of 6.03 points for guanfacine XR and an effect size of 0.52 (P<0.001). Although the numerical advantages for several Weiss Functional Impairment Rating Scale – Parent Report (WFIRS-P) domains, including learning and school and family, approached but did not reach statistical significance, the proportion of patients achieving a CGI-S score ≤2 also significantly favored guanfacine XR (50.6% vs. 36.1%; P=0.010) over placebo.
“Guanfacine XR achieved its primary endpoint at the end of 13 weeks in adolescents,” confirmed Dr. Timothy E. Wilens, Massachusetts General Hospital, Boston. Noting that 80% of ADHD children have persistent symptoms throughout adolescence, Dr. Wilens indicated that these data support the benefits of guanfacine XR already demonstrated in younger children. He also reported that the safety profile in adolescents is consistent with that seen in children.
“There were no clinically-meaningful differences between guanfacine XR and placebo on hematology, chemistry, or urine analyses,” Dr. Wilens reported. Although several specific adverse events were more common on guanfacine XR than placebo, such as somnolence (43.9% vs. 21.3%), fatigue (22.3% vs. 12.3%) and nasopharyngitis (11.5% vs. 5.8%), the majority of these events was mild to moderate and tended to resolve over the course of the study. Discontinuation of therapy due to an adverse event occurred in 9 patients on guanfacine XR and three taking placebo.
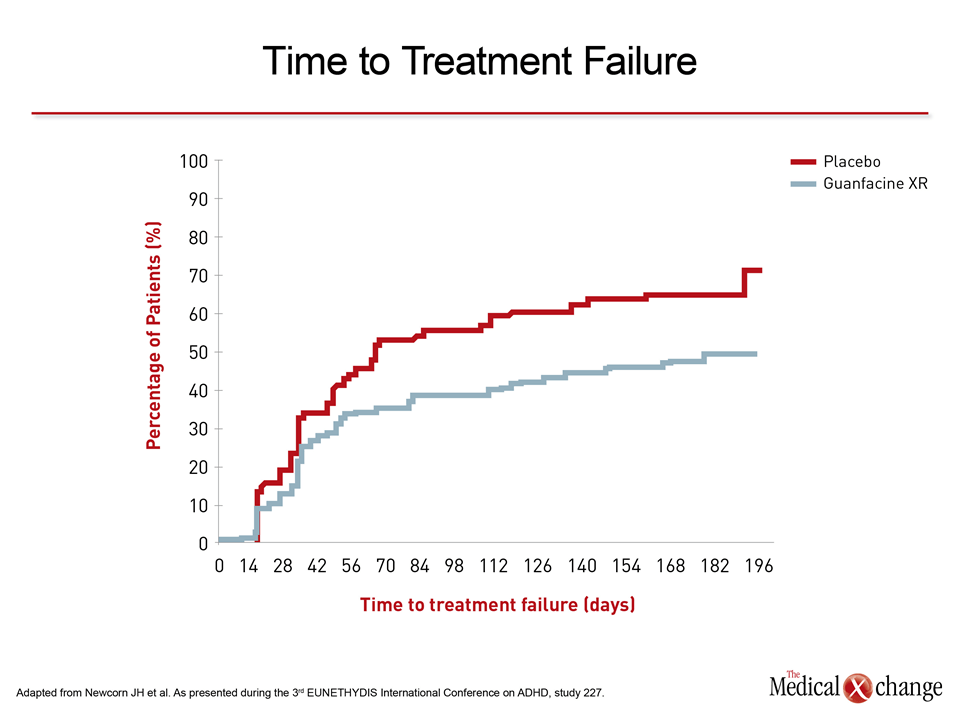
A long-term double-blind maintenance study that enrolled ADHD patients from the age of 6 up to the age of 17 has also expanded controlled evidence of benefit from guanfacine XR in adolescents. In this study, 528 patients entered an open-label phase in which patients initiated treatment on 1 mg guanfacine XR once daily and were then dose optimized to maximum dose of 7 mg. After 13 weeks in the open label phase, responders were randomized to remain on their optimized dose or initiate placebo. They were then followed for an additional 26 weeks in a double-blind phase. The primary endpoint in this study was time to treatment failure.
“Both the cumulative proportion of treatment failures (49.3% vs. 64.9%) and the median time to treatment failure (218 vs. 56 days) favored guanfacine XR,” reported Dr. Jeffrey H. Newcorn, Icahn School of Medicine at Mount Sinai, New York City, New York (Fig. 2). He noted that although there is little comparable information with stimulants using a similar withdrawal design, now but not previously required by regulatory agencies, the data “support the value of maintenance guanfacine XR in pediatric patients up to the age of 17 who respond to initial therapy.”
Symptom Reduction
In another phase 3 study testing newer therapies for ADHD, enrolment was open to children and adolescents aged 6 to 17 years. In this study, 338 patients with ADHD of at least moderate severity (ADHD RS-IV score ≥32) were recruited at 58 treatment centers in Europe, the United States and Canada. The patients were randomized to guanfacine XR, atomoxetine, or placebo in a double-dummy design. The primary endpoint was change in ADHD-RS-IV from baseline. The ADHD-RS-IV score reductions were 15 on placebo, 23.9 for guanfacine XR, and 18.8 for atomoxetine. Both differences were significant relative to placebo (Fig. 3).
In this study, “atomoxetine was included to provide reference data and the study was not designed to provide a head-to-head comparison,” reported the lead investigator, Dr. Amaia Hervás, Child and Adolescent Mental Health Unit, University Hospital Mútua de Terrassa, Barcelona, Spain. However, she observed that a pre-specified secondary analysis “showed a significant difference in ADHD-RS-IV score (effect size 0.44; P=0.001), indicating that the symptom reduction was greater for guanfacine XR than atomoxetine.”
After enrolment and randomization, all patients entered a dose optimization phase that lasted 4 weeks in children (6 to 12 years) and 7 weeks in adolescents (13 to 17 years). Dose optimization was defined as ≥30% improvement in ADHD-RS-IV score and a Clinical Global Impression – Improvement (CGI-I) score of 2 (much improved) or 1 (very much improved) in the absence or safety or tolerability issues. For guanfacine XR, the dose increments were 1 mg one week apart to a maximum of 4 mg in children and 7 mg in adolescents. For atomoxetine, the dose increments were 1.2 mg/kg in those <70 kg but was increased to 40 mg at the second visit in those who weighed more and had an inadequate response. In these children, up to 100 mg was allowed, if needed.
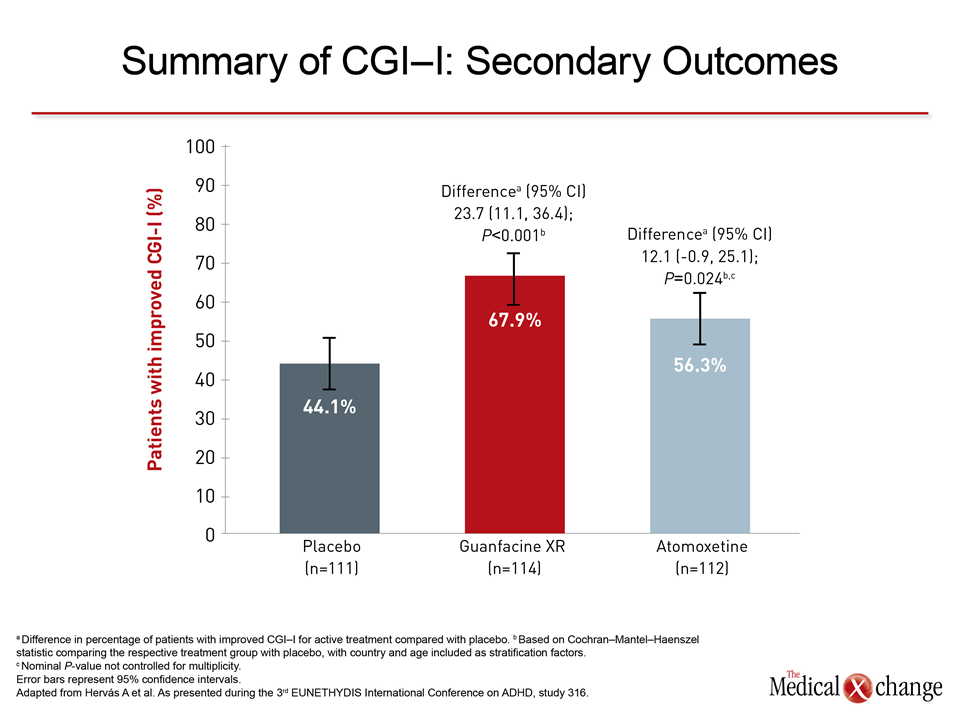
Secondary Outcomes
At the end of 13 weeks on active therapy, the guanfacine XR and atomoxetine also differed on several additional secondary outcomes. These included the global score of the WFIRS-P and the CGI-I (Fig. 4). Within the WFIRS-P, both guanfacine XR and atomoxetine produced improvements relative to placebo in the domains of learning and behavior in school, but only guanfacine XR significantly improved domains of family and child self-concept.
Dr. Judy van Stralen, who was a co-author of this study, was asked to comment on these results from a Canadian perspective. While she suggested that these data support guanfacine XR as “an adjunctive and alternative option when stimulants alone are not sufficient medical treatment of ADHD,” she also reported that the data are consistent with her practice. “In my clinical experience, guanfacine XR has been an excellent choice for some patients significantly changing their level of functioning for the better,” remarked Dr. van Stralen.
Conclusion
A series of studies have provided new objective evidence regarding the role of guanfacine XR and atomoxetine therapies for ADHD. Although stimulants are the first-line choice and provide adequate efficacy in the majority of patients, such options as guanfacine XR and atomoxetine demonstrate substantial treatment effects, according to a large and expanding pool of data from double-blind studies. The new trial data have also provided evidence that the efficacy of guanfacine XR is clinically meaningful in both children and adolescents. These data expand objective evidence about treatment options for those ADHD patients who do not achieve adequate response to the first-line agents.