Gastroenterology
3rd International Symposium on Pediatric Inflammatory Bowel Disease (PiBD 2014)
Challenges in the Management of Pediatric IBD: Expanding Treatment Options
Rotterdam – In Canada, as elsewhere, the incidence of inflammatory bowel disease (IBD) has been rising significantly in children and adolescents, particularly in children aged under 10 years (Crohn’s and Colitis Foundation of Canada, 2012). Children and adolescents with IBD have more extensive and severe disease, need more comprehensive work-up and require more aggressive treatment than adults. They also face the possibility of growth problems and pubertal delay.Results presented at this year’s PiBD conference showed improvement in growth with anti-TNF therapy, as well, similar response and remission rates were observed regardless of immunotherapy use at baseline. Close monitoring of fecal calprotectin to better predict relapse and considering earlier anti-TNF treatment to achieve remission is an important step forward in IBD care.
Pediatric inflammatory bowel disease (IBD) accounts for 20 to 25% of cases of IBD worldwide, and like adult-onset disease, the incidence of pediatric IBD continues to rise. More studies are exploring the use of anti-TNFs as first-line therapy.
Recommending Anti-TNF Therapy in Pediatric CD
New European Crohn’s and Colitis Organisation/European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ECCO/ESPGHAN) consensus guidelines also recommend anti-TNF therapy for inducing and maintaining remission in children with chronically active luminal Crohn’s disease (CD) despite prior optimized immunomodulator therapy and for inducing remission in children with active steroid-refractory disease (Ruemmele FM et al. J Crohns Colitis. Epub June 5, 2014).
“We know this is really good medication, and I believe it is one reason why our North American colleagues are moving more toward anti-TNF therapy as first line.”
These recommendations were based on the results of the REACH study with infliximab (Hyams J et al. Gastroenterology2007;132:863-73) and the IMAgINE 1 study with adalimumab (Ruemmele FM et al. Inflamm Bowel Dis 2009;15:388-94). “We know this is really good medication, and I believe it is one reason why our North American colleagues are moving more toward anti-TNF therapy as first line,” commented Prof. Frank Ruemmele, Hôpital Necker-Enfants Malades, Paris, France.
The Potential to Address Delayed Growth
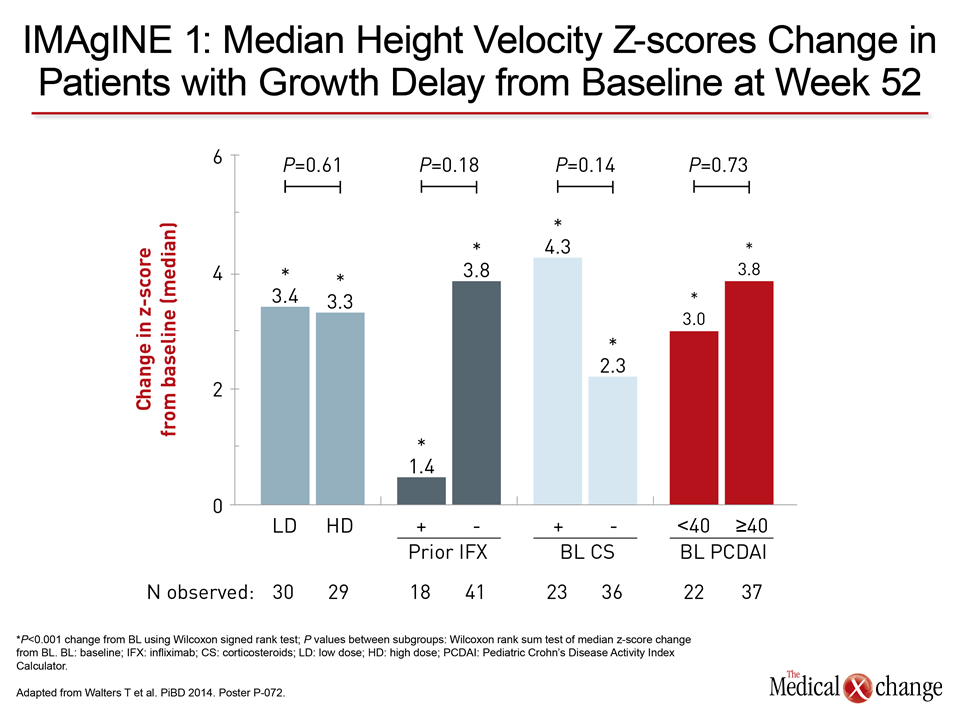
The IMAgINE 1 clinical trial showed a significant improvement in height velocity z-scores from baseline with adalimumab in all patients. Dr. Thomas Walters, The Hospital for Sick Children, Toronto, Ontario, reported that it was also associated with significantly improved growth in those patients who showed delayed growth at baseline (z-score ≤1). There were significant changes through the period of therapy from a median z-score of -2.88 to 2.43 at 26 weeks and 3.31 at 52 weeks (both P<0.001). Growth improvement trended to be larger in patients with baseline corticosteroid use, severe CD, and in infliximab-naive patients (Fig. 1).
“The potential for improvement in growth in these subgroups is probably greater,” Dr. Walters suggested. “This effect requires further prospective study.”
Rates of Response with Concomitant Use of Immunomodulators
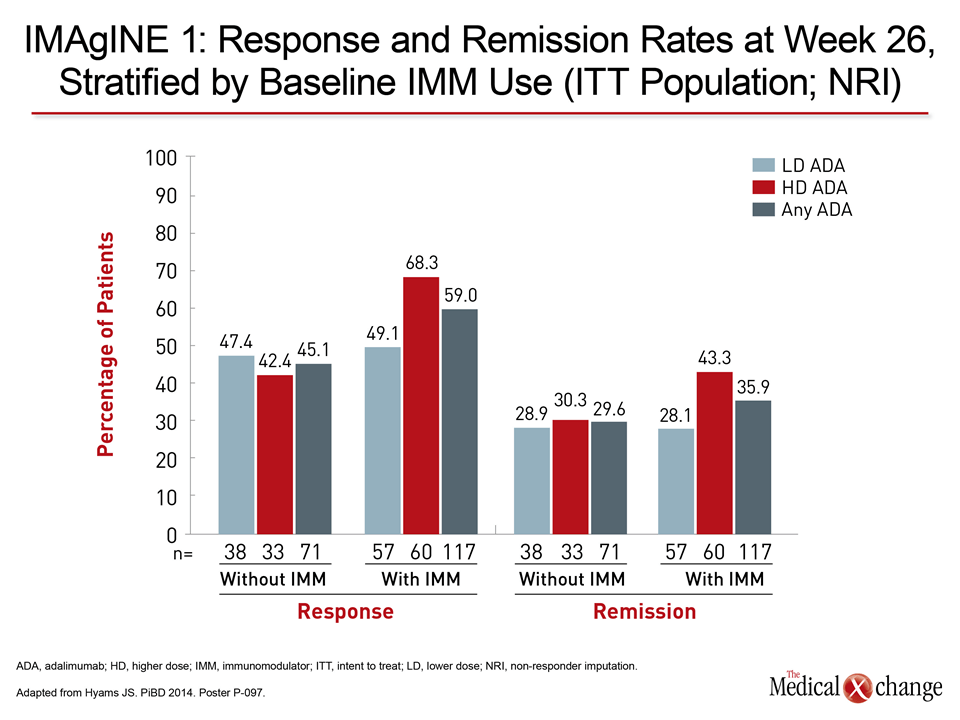
Another analysis of IMAgINE 1 data showed that rates of clinical response and remission achieved with adalimumab were not affected by concomitant use of immunomodulator therapy. As reported by Dr. Jeffrey Hyams, Connecticut Children’s Medical Center, Hartford, rates were comparable at week 26 with or without baseline immunomodulators (Fig. 2). Proportions of patients who experienced serious adverse events (AEs) and serious infectious AEs were also similar in both groups.
Disease Activity Index and Fecal Calprotectin Levels
A multicentre retrospective study presented by Dr. Javier Martín-de-Carpi and colleagues, Hospital Sant Joan de Déu, Barcelona, Spain provided further evidence that adalimumab is safe and effective in inducing and maintaining remission in anti-TNF-naive pediatric CD patients. Among 40 patients treated with adalimumab as first anti-TNF over 16 months, 36 were in clinical remissionaccording to thePediatric Crohn’s Disease Activity Index Calculator(PCDAI) <10 after 24 months of follow-up.
A significant decrease was seen in fecal calprotectin (FC) levels, from a mean of 747 mg/g to 131 mg/g at 12 weeks and to 255 mg/g at 52 weeks (P=0.001). No severe adverse reactions, infections or malignancies were reported.
Exploring the Impact of FC Measurement on the Management of Pediatric IBD
FC levels may be more reliable and non-invasive to predict relapse in CD than ESR or CRP, according to preliminary findings from an ongoing study. Dr. Kevan Jacobson and colleagues, British Columbia Children’s Hospital, Vancouver, reported on 44 pediatric CD patients in clinical remission receiving infliximab maintenance therapy who have been followed for 6 months. Five patients have relapsed, all of whom had elevations in FC (232-2023 mg/g) an average of 72 days before relapse. ESR was also elevated in 5 patients but CRP and PCDAI were elevated in only 2 patients each. The same group is exploring the impact of FC measurement on the management of pediatric IBD.
“Clinicians should move away from single calprotectin measurements, which are not plausible for prediction release, and shift their focus to periodic calprotectin testing to guide the management of IBD.”
A retrospective chart review of 55 patients found that of 42 with FC levels >200 mg/g, 38 had escalation of therapy and/or additional investigations. “Clinicians should move away from single calprotectin measurements, which are not plausible for prediction release, and shift their focus to periodic calprotectin testing to guide the management of IBD,” notedDr. Patrick F. van Rheenen, University Medical Center Groningen, The Netherlands. “If this ‘close monitoring’ strategy proves to be beneficial for patients in a randomized trial, it will be an important step forward in IBD care,” he predicted.
Conclusion
As in adult disease, treatment options in pediatric IBD with anti-TNF therapy are expanding and considered earlier in the treatment algorithm. Adding a closer monitoring using FC measurement may be a more earlier accurate predictor of clinical relapse after remission.