Hematology
The National Hemophilia Foundation 66th Annual Meeting
Primary Prophylaxis in Hemophilia: A New Standard in Patient Care
Washington, D.C. – Studies have shown that routine primary prophylaxis with factor VIII and IX concentrates dramatically reduces bleeding rates compared to an on-demand schedule. However, the short half-life of factor concentrates makes for frequent infusions. Applying Fc fusion to recombinant coagulation factors significantly extends factor half-life. Studies have shown that these newer agents permit for lower bleeding rates, fewer weekly infusions with lower or comparable factor use, allowing for potentially improved adherence and patient outcomes.
According to Dr. Steven Pipe, University of Michigan, Ann Arbor, the use of primary prophylaxis with coagulation factors is an essential management tool. “Even delaying prophylaxis 2 or 3 years and starting factor in a toddler who’s already had a chance to bleed is secondary prophylaxis and inferior to primary prophylaxis,” Dr. Pipe emphasized.
A Case for Routine Prophylaxis
In adolescents and adults with severe hemophilia A, results from the SPINART study (J Thromb Haemost 2013;11:1119-27) demonstrated that there was a 94% reduction in the mean annual bleeding rate (ABR) using prophylaxis with a sucrose-formulated recombinant FVIII (rFVIII-FS) over a median follow-up of 1.7 years compared with on-demand, episodic use. There was also a 93% reduction in the average number of joint bleeds in the routine prophylaxis group compared with the on-demand group and 62% of the routine prophylaxis group had no joint bleeds at all.
“Even delaying prophylaxis 2 or 3 years and starting factor in a toddler who’s already had a chance to bleed is secondary prophylaxis and inferior to primary prophylaxis.”
In children up to 16 years of age with hemophilia A and no joint damage on study entry, no joint damage was seen in 9 out of 10 children on routine rFVIII-FS prophylaxis for up to 5.5 years compared with 55% of children given on-demand rFVIII-FS. Routine prophylaxis also provided for 87% fewer annual joint bleeds compared to those treated with the on-demand schedule. Overall, 12.5% developed inhibitors (8 of 64 patients) but there were no life-threatening bleeds in the prophylaxis group vs. 3 in the episodic group.
However, the average half-life of factor VIII agents ranges from 8 to 12 hours—demanding routine injections 3 to 4 times a week. Fusing the FC portion of immunoglobulin G1 to FVIII prolongs the half-life.
In previously treated males ≥12 years of age with severe hemophilia A, Mahlangu et al. found that a recombinant factor VIII fusion protein (rFVIIIFc) with longer half-life resulted in low bleeding rates when dosed 1 to 2 times a week (Blood 2014:123:317-25).
In the study, the superiority of both individualized and weekly prophylaxis regimens over episodic or “on-demand” prophylaxis was demonstrated. The median ABR in subjects treated with rFVIIIFc on an individualized or weekly prophylaxis regimen (q3-5 days) was 1.6 and 3.6, respectively, compared to a median of 33.6 for those treated episodically.
Moreover, 30% of patients in the individualized prophylaxis arm required prophylaxis q5 days during the last 3 months of the trial. No patient in the trial developed inhibitors and there were no drug-related serious adverse events (SAEs).
Kids A-Long Study Update
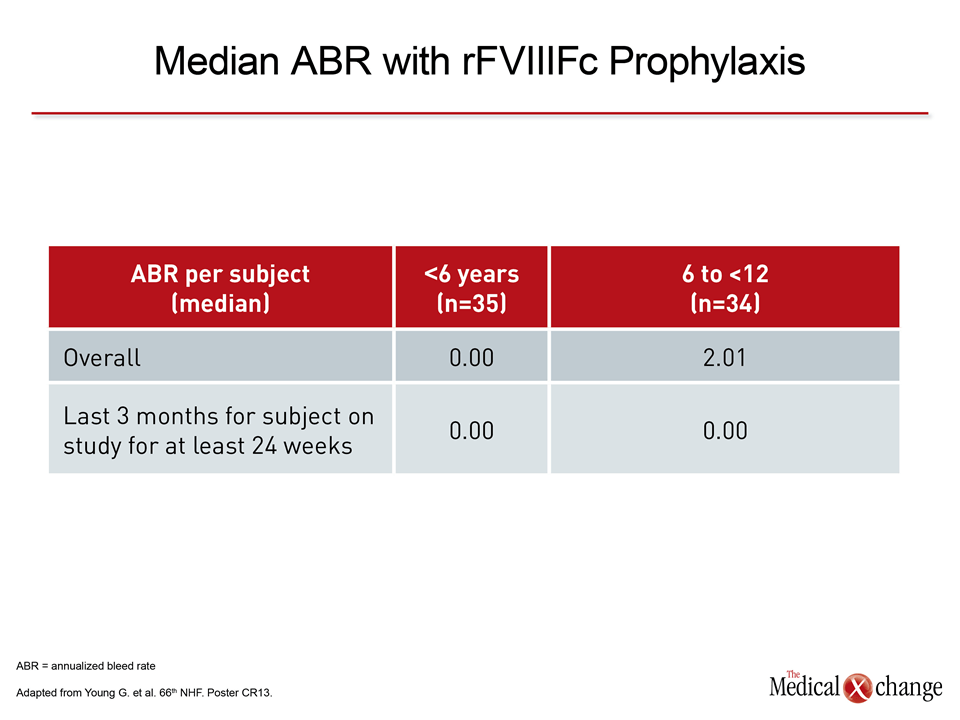
In the Kids A-LONG clinical trial, the long-lasting rFVIIIFc was shown to have about a 50% longer half-life than conventional rFVIII. In an update of the study, Dr. Guy Young, Director, Hemostasis and Thrombosis Center, Children’s Hospital Los Angeles, California, reported that the infusion interval of rFVIIIFc can be reduced to twice a week for most children. In the study, 67 children 50 rFVIIIFc exposure days, the estimated inhibitor incidence rate was zero,” Dr. Young reported, adding that no subjects developed clinically meaningful non-neutralizing antibodies to rFVIIIFc. AEs suspected to be related to rFVIIIFc were noted in 2 children and both continued with the regimen. There were no reports of anaphylaxis, vascular thrombotic events and no deaths.
Pharmacokinetics was performed on a subgroup of children and confirmed a 1.5 to 1.6-fold longer half-life for rFVIIIFc than standard FVIII. “Importantly, 90% of patients stayed on a twice-weekly dosing regimen and had a very low ABR and the drug was effective when bleeding episodes did occur,” Dr. Young noted (Table 1).
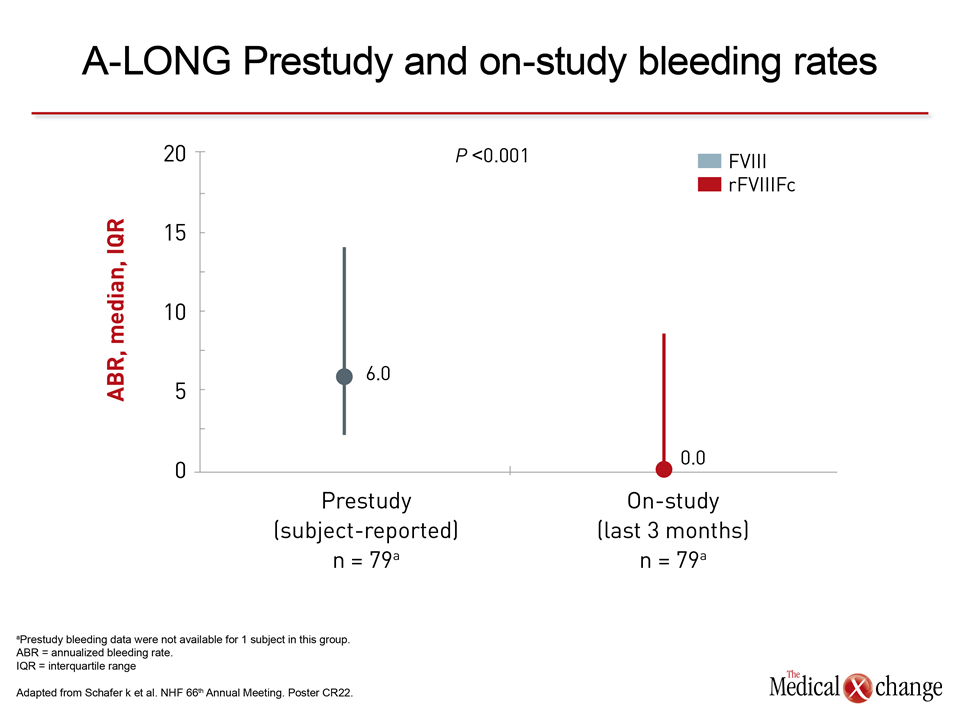
In a post-hoc analysis of the A-LONG study by Schafer K et al., the weekly number of prophylactic infusions decreased in all, but 1 patient switched to rFVIIIFc from conventional FVIII products. The median ABR decreased from 6 before study entry to zero during the last 3 months of the study. The 1 patient whose dosing frequency increased with rFVIIIFc had a pre-study ABR of 42 compared to zero over the last 3 months of the study. Additional Slide 1A (Fig. 1A).
Reduced Factor Use
In hemophilia B, recombinant factor IX Fc fusion protein (rFIXFc) was shown to have a mean half-life of 82.1 hours in the B-LONG clinical trial. The most common pre-study dosing interval was twice a week in over two-thirds of patients.
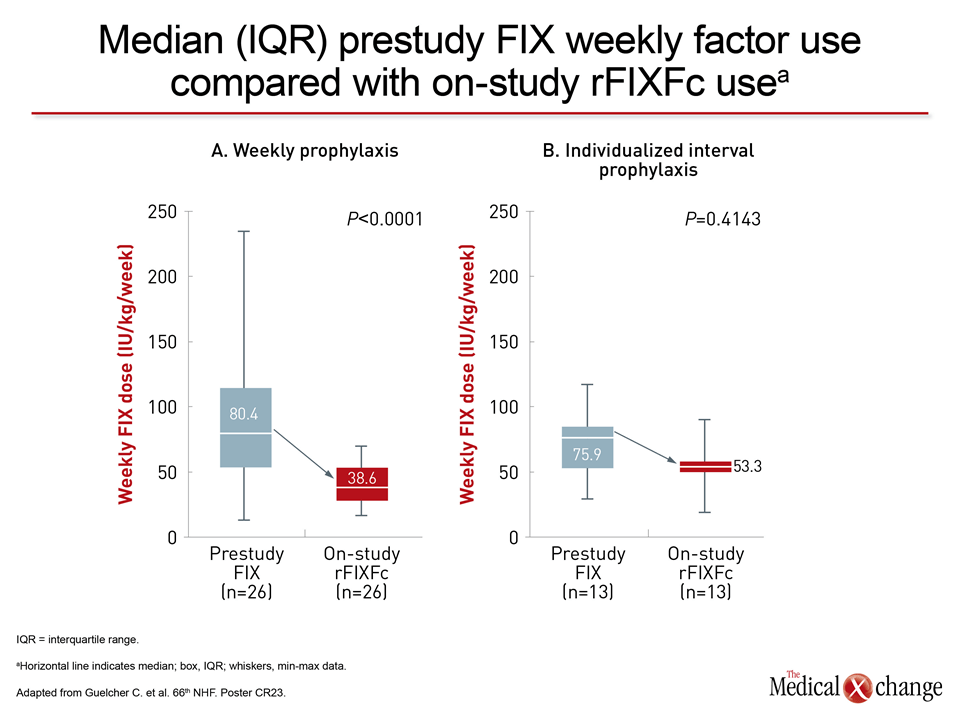
In the B-LONG study, both weekly and individualized prophylactic rFIXFc regimens were evaluated. Compared to pre-study FIX prophylaxis, patients receiving prophylaxis either weekly or on an individualized interval basis had reduced factor use, less frequent infusions and lower bleeding rates (Fig. 1).
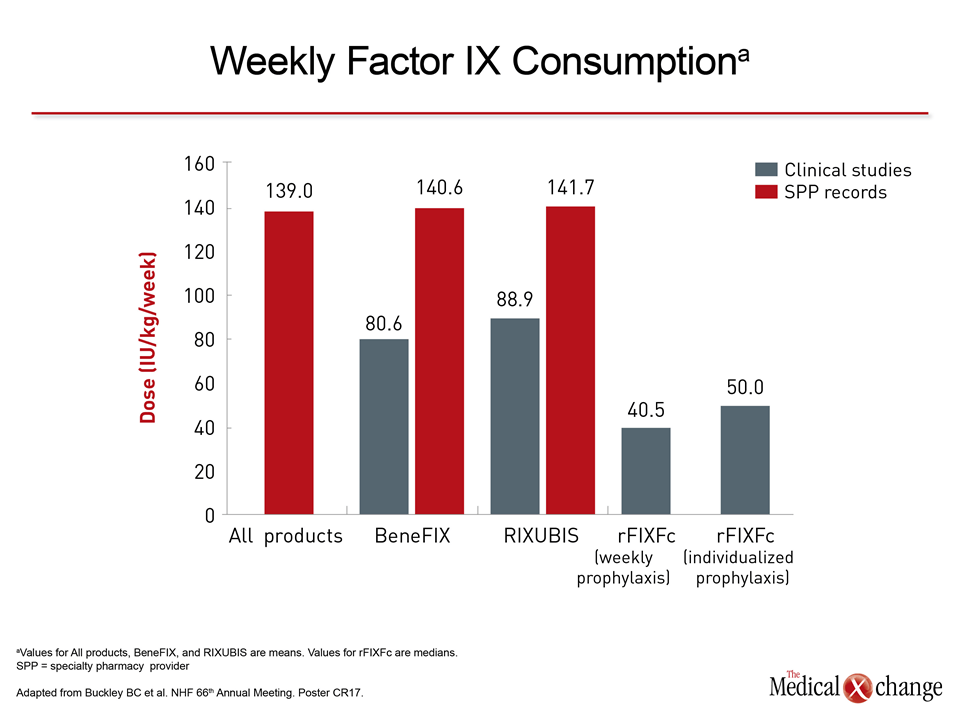
As reported by Powell et al. (Br J HaematolEpub ahead of print Sep 11, 2014), a post-hoc analysis of B-LONG confirmed that patients receiving rFIXFc prophylaxis can markedly reduce infusion frequency and FIX consumption. They are also more likely to maintain FIX activity and experience fewer bleeding episodes compared with prior FIX prophylaxis. Limited dosing and use of rFIXFc are available from the real-world setting but a database from Specialty Pharmacy Provider records suggests that over three-quarters of patients with hemophilia B on a prophylactic regimen have a dosing interval of once a week and the remainder have an infusion interval >q7 days (Poster CR17). Additional Slide 1B (Fig. 1B).
Conclusion
Having access to coagulation factor products with longer half-lives and thus fewer routine infusions may improve patient adherence. The lower mean ABR with the newer extended half-life recombinant agents may significantly enhance quality of life for patients with either form of hemophilia.