Cardiology
American Heart Association (AHA) Scientific Sessions 2014
More Cardioprotection when a Non-statin Cholesterol-lowering Agent is added to a Statin
Chicago – Lowering LDL-cholesterol (LDL-C) is a mainstay of cardiovascular (CV) prevention, but this has been mainly supported by evidence from statin trials. IMPROVE-IT is the first trial to demonstrate that there is an incremental benefit when adding a non-statin agent to statin therapy. The trial also showed that reducing LDL-C with a combination of a statin and non-statin to levels lower than those achieved with a statin alone further reduced CV events, reaffirming the hypothesis that reducing LDL-C prevents CV events.
Although lowering LDL-cholesterol (LDL-C) to prevent cardiovascular (CV) events has been based on treatment with statins, current guidelines recommend that favorable effects can also be achieved with non-statin agents such as ezetimibe or bile acid sequestrants in people who do not tolerate statin therapy or only at low dose (Anderson TJ et al. Can J Cardiol 2013;29:151-67). Despite current therapies, however, patients remain at high risk. IMPROVE-IT was the first large, double-blind, randomized trial to evaluate whether adding another type of cholesterol-lowering agent to statin therapy could lead to a further reduction in heart attacks and strokes in high-risk patients with acute coronary syndrome (ACS).
Lower LDL-C Levels Achieved
IMPROVE-IT involved 18,144 patients aged ≥50 years who had been hospitalized for an ACS event (STEMI, NSTEMI/unstable angina) at over 1100 sites in 39 countries. All patients received standard interventional and medical therapy, explained principal trial investigator Dr. Christopher Cannon, Brigham and Women’s Hospital, Boston, MA. Their baseline LDL-C levels were in a medium range (1.3-3.2 mmol/L, or 1.3-2.6 mmol/L if they had previously received lipid-lowering therapy).
Further lowering of LDL-C with a non-statin added to statin therapy is associated with a greater reduction in CV events in high-risk patients.
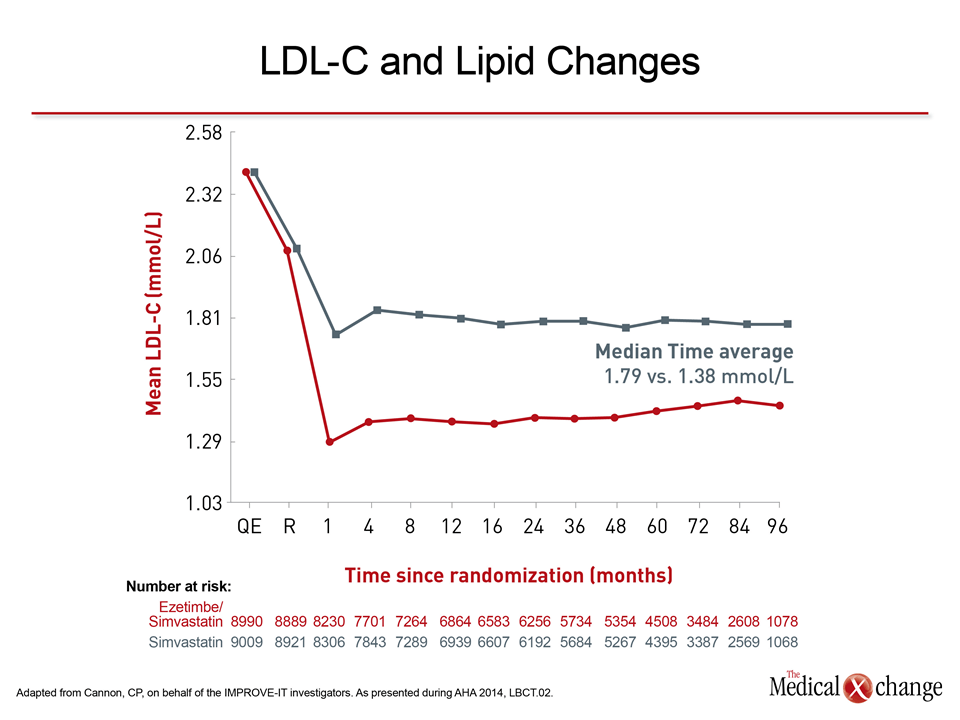
Randomized treatment consisted of simvastatin 40 mg or a fixed-dose combination of ezetimibe 10 mg/ simvastatin 40 mg (not available in Canada). Following guideline recommendations at the time, simvastatin was uptitrated to 80 mg if LDL-C was >2 mmol/L. The LDL-C target for the monotherapy arm was <1.8 mmol/L and the combination was assumed to further lower LDL-C by 0.39 mmol/L, Dr. Cannon explained. At 1 year, mean LDL-C was 1.8 mmol/L in the monotherapy group vs 1.38 mmol/L with the combination. The achieved median LDL-C levels over 9 years were 1.8 mmol/L and 1.39 mmol/L, respectively.
Lower LDL-C Further Reduces CV Events
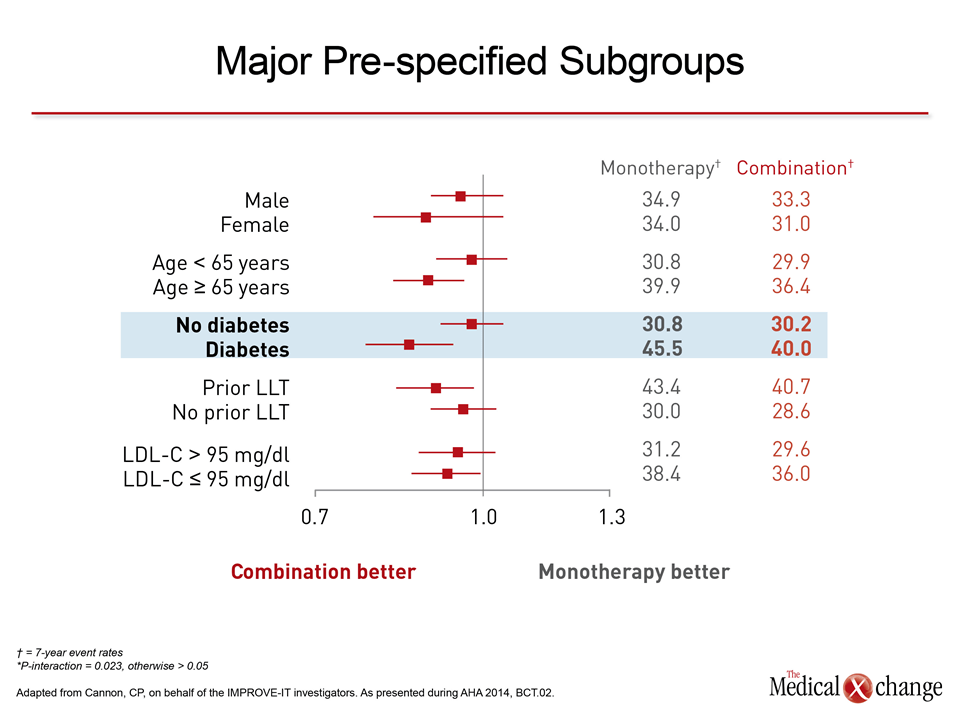
“In patients with diabetes, more aggressive lipid modification produced a greater apparent benefit.”
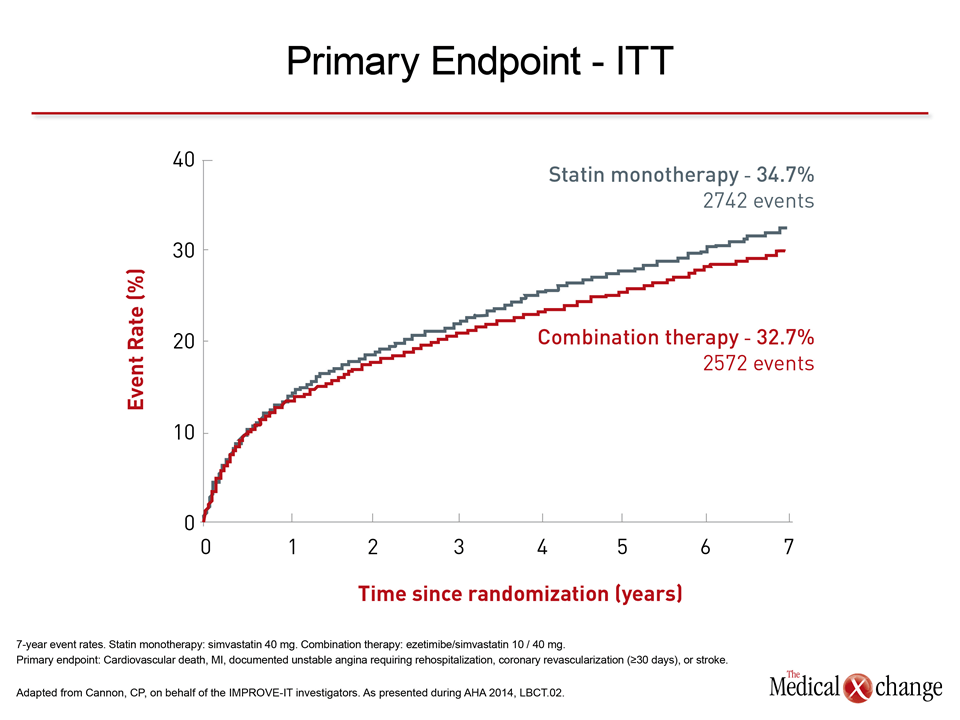
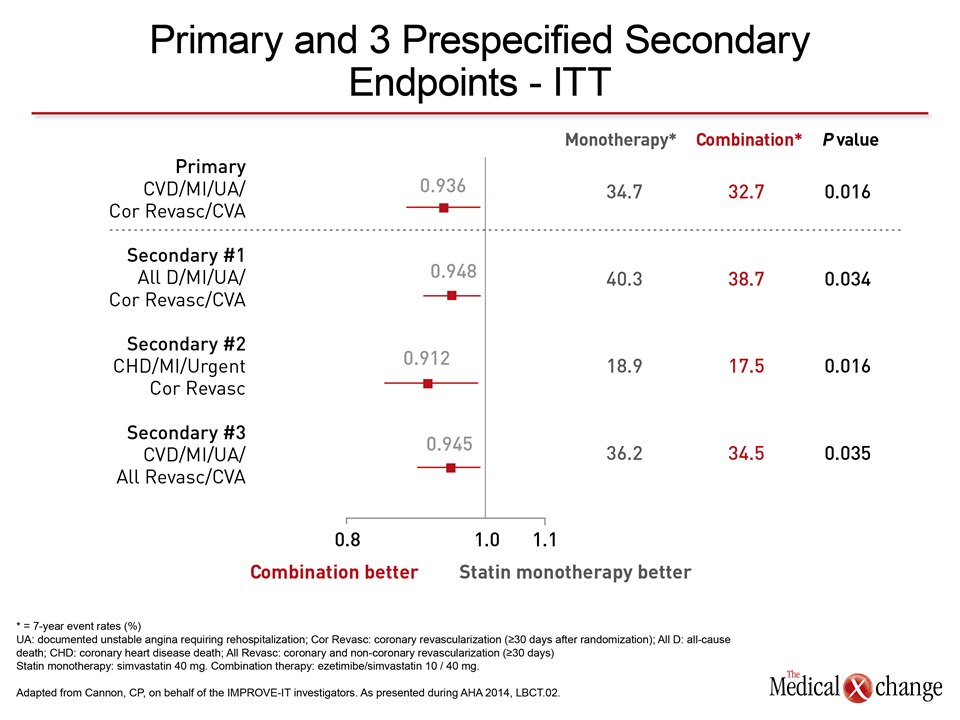
The results were consistent across all major pre-specified subgroups. “Interestingly, in patients with diabetes, more aggressive lipid modification produced a greater apparent benefit, with a 5.5% absolute reduction in events compared with non-diabetic patients,” Dr. Cannon noted (Fig. 1).“The big question was, would the further change in LDL-C with a non-statin agent lead to a reduction in CV events, and we saw that it did,” Dr. Cannon declared. After 7 years of follow-up, event rates were reduced from 34.7% to 32.7% (P=0.016). “The addition of ezetimibe produced a significant 6.4% reduction in the primary composite endpoint of CV death, nonfatal MI, nonfatal stroke, rehospitalization for unstable angina, and coronary revascularization, or stroke,” Dr. Cannon confirmed. “That translated into a number of patients needed to be treated (NNT) to prevent one of these events of 50, well within the range of our standard therapies.” “There were significant reductions of 13% in MI (P=0.002) and 14% in stroke (P=0.052), very hard endpoints and important medical problems for patients,” and a 5% trend toward a reduction in coronary revascularization. Benefit with the added drug was seen to start at one year.
Non-statins vs Statins
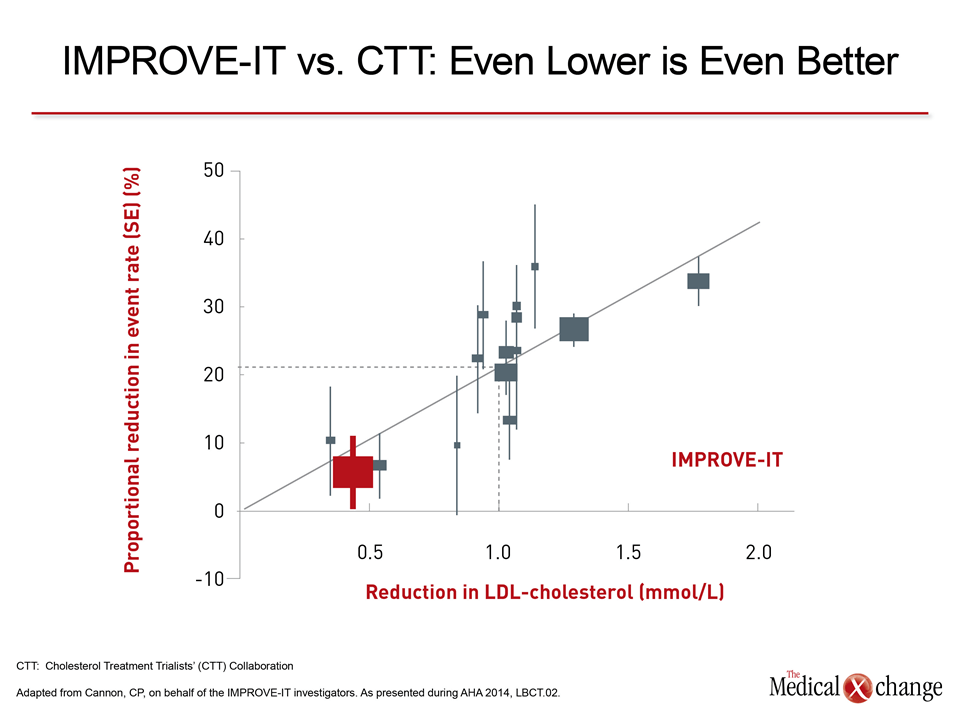
“The next big question was how a non-statin agent and the benefit match up against that of statins,” Dr. Cannon noted. An analysis by the Cholesterol Treatment Trialists’ (CTT) Collaboration concluded that every 1 mM of LDL-C lowering with a statin produces an approximate 20% treatment benefit (CTT Collaboration. Lancet. 2010;376:1670-1681). The same type of analysis with IMPROVE-IT data showed that “every one of these endpoints fell on or near the line of 20% benefit”, indicating the treatment effect associated with adding ezetimibe to a statin was at least consistent with, if not greater than that achieved with statins alone (Fig. 2).
Implications for Treatment Options
Dr. Jean C. Grégoire, Institut de Cardiologie de Montréal, Université de Montréal, co-author of the Canadian Cardiovascular Society’s 2012 dyslipidemia guidelines update, welcomed the IMPROVE-IT results as “very good news for physicians and for our patients.”
He noted that “before IMPROVE-IT, no trial had demonstrated benefit of a non-statin treatment in combination with a statin. Because the statin/non-statin combination was able to decrease the LDL-C to such a low value, it is possible that if we lower LDL-C more, we can improve outcomes,” he stated. “This applies to any kind of non-statin medication with an indication to decrease cholesterol, including bile acid sequestrants, ezetimibe, and fibrates, although fibrate are not widely used,” Dr. Grégoire noted. “It is interesting that all patients in the IMPROVE-IT trial were well treated, so below target. This means that if you start with low LDL-C but you reach a very low level and you get benefit, it affirms the hypothesis that if you reduce the LDL-C you prevent CV events,” he said. “And as IMPROVE-IT fits very nicely on the CTT linear regression line, it suggests that if we decrease the LDL-C very low you are going to continue to get benefit,” he added.
Conclusion
The IMPROVE-IT trial showed that further lowering of LDL-C with a non-statin added to statin therapy is associated with a greater reduction in CV events in high-risk patients. This offers hope and questions for study as to whether other non-statin medications with an indication to reduce LDL-C may further improve benefit when added to statin therapy.