Cardiology
American Heart Association (AHA) Scientific Sessions 2014
Newer P2Y12 Inhibitors in ACS: Significant Reduction in Stent Thrombosis and Mortality
Chicago – In a 12-month “real world” study of P2Y12 inhibitors in over 6500 ACS patients treated at a single centre, one agent was associated with lower stent thrombosis and mortality rates in all patients compared with two other agents in the study. The new findings suggest that treating these patients with this agent, instead of the previous standard treatment, could reduce the risks of stent thrombosis by 50%, which usually requires a repeat procedure or may even be fatal.
Over the past decade, clopidogrel has been the standard antiplatelet agent, but the newer oral P2Y12 inhibitors prasugrel and ticagrelor provide more potent and consistent inhibition of platelet aggregation during maintenance therapy in ACS patients, as shown in landmark clinical trials. Compared with clopidogrel, ticagrelor in the PLATO trial showed a significant reduction in ischemic events in all ACS patients, including those who underwent revascularization and in those who had received medical treatment. In the TRITON-TIMI 38, significant reductions in ischemic events were observed in all patients treated with prasugrel, but not in only medically treated non-ST-elevation (NSTE) ACS patients in TRILOGY-ACS. Researchers in the UK led by Dr. Javaid Iqbal, University of Sheffield, investigated 12-month outcomes with the P2Y12 inhibitors clopidogrel, prasugrel and ticagrelor in ACS patients at a single regional centre in the city of Sheffield. “This is the first study in a real-world, ‘all-comers’ population,” noted Dr. Iqbal. Data were collected for 6742 ACS consecutive patients attending the cardiac catheterization lab between 2009 and 2013. All these patients (36% STEMI, 64% NSTE-ACS) received ASA together with clopidogrel (67%), prasugrel (15%) and ticagrelor (18%). “The choice of P2Y12 inhibitor reflected changes in the European guidelines over time,” Dr. Iqbal explained. “When ticagrelor became available in 2011, our institution was one of the first to adopt it for ACS patients.
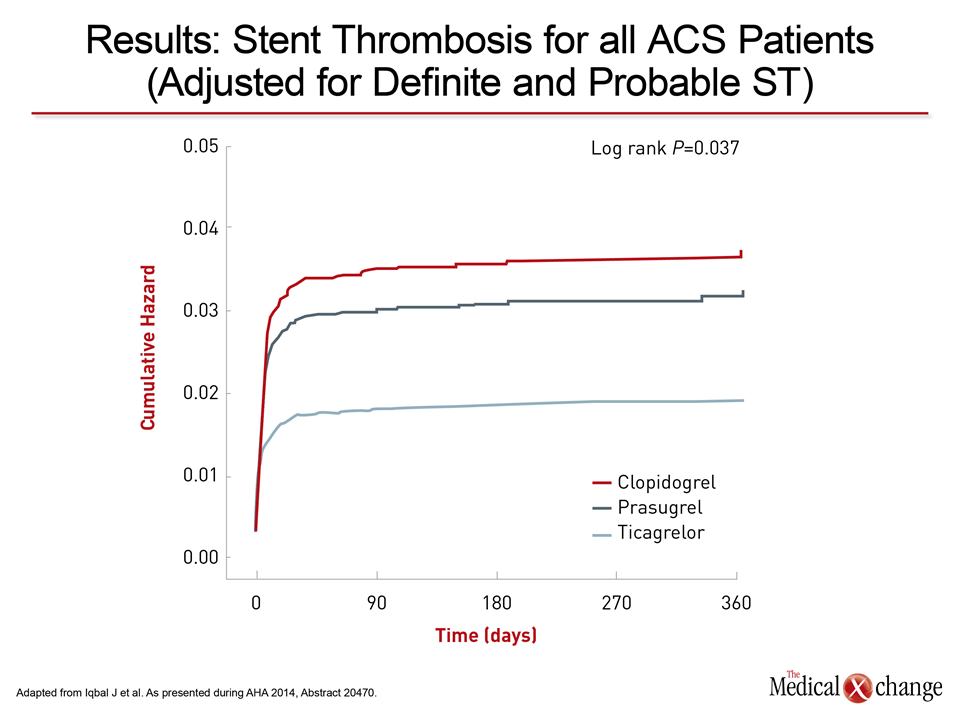
Significant Reduction in Stent Thrombosis
Among patients at the centre who received ticagrelor, the incidence of definite stent thrombosis at 12 months was <1%, Dr. Iqbal reported. The incidence of definite/probable stent thrombosis was significantly lower with ticagrelor compared with clopidogrel and prasugrel (2.1% vs. 4.2% and 4.5%, P<0.01) and remained significant after adjustment for differences in baseline characteristics among the three treatment groups (Fig. 1). In evaluating independent predictors of stent thrombosis, a 13% risk reduction was revealed with prasugrel vs. clopidogrel, whereas “ticagrelor really halved the risk of stent thrombosis compared with clopidogrel.” TIA/stroke was an independent risk factor for stent thrombosis. “This was important because for prasugrel there is a contraindication in patients aged ≥75 years or with a history of TIA/stroke, but these patients were aged <75 years and did not have a previous history of stroke,” Dr. Iqbal commented. In the overall population, all-cause mortality was significantly reduced with prasugrel and ticagrelor compared with clopidogrel. Between prasugrel and ticagrelor, the reductions in all-cause mortality were not statistically significant due to small numbers, although for ticagrelor there was a trend toward an effect, Dr. Iqbal explained. “From our data it does look like that in terms of the stent thrombosis alone, ticagrelor seems to be performing better,” Dr. Iqbal concluded. “We don’t have a randomized controlled trial at the moment, but that is what the data are currently suggesting from our analysis.”