Rheumatology
European League Against Rheumatism (EULAR) 2015 Congress
Interleukin-6 Inhibitors: Improving Biologic Specificity in the Control of Rheumatoid Arthritis
Rome – A new wave of biologics targeted at interleukin-6 (IL-6) is expected to provide an incremental advance in the treatment of rheumatoid arthritis (RA), judging from data presented at this year’s EULAR. Relative to tumor necrosis factor alpha (TNF-α), IL-6 may be a more rational biologic target because of evidence that it is active earlier in the course of RA pathophysiology, may be more directly implicated in pain signaling, and can be linked closely to major molecular processes driving joint destruction. Several new generation IL-6 inhibitors have reached late stages of clinical testing with promising activity and acceptable tolerability. The newer agents have the potential to build upon the efficacy of earlier generations of biologics.
Building on Biologics
A large part of the effort to build on the benefit of biologics for the control of rheumatoid arthritis (RA) is being concentrated on the inhibition of interleukin-6 (IL-6) activity, judging from the preponderance of data presented at EULAR 2015. Available biologics are highly effective in a substantial proportion of individuals, but new options in this disease are needed for the large proportion of patients who do not achieve or lose sustained disease control on first-generation agents.
The activity of the pro-inflammatory cytokine IL-6 may be more relevant than TNF-α to the specific pathological processes that drive RA.
Relative to TNF-α, the activity of the pro-inflammatory cytokine IL-6 may be more relevant to the specific pathological processes that drive RA, according to Dr. Ernest Choy, Professor of Rheumatology, Cardiff Institute of Infection and Immunology, Cardiff, UK. Specifically, IL-6, which is one of the most abundant cytokines expressed in the synovial fluid of RA patients, is more closely associated with the transition to chronic phase inflammation as well as to upregulation of joint destructive proteolytic enzymes.
IL-6 has long been recognized as an attractive target in RA, but interest intensified when it was understood that it can mediate inflammation by both conventional membrane-bound receptors (IL-6R) and through trans-signaling mediated by circulating soluble IL-6 receptors (sIL-6R), according to Dr. Cem Gabay, Professor, Service of Rheumatology, Geneva University Hospitals, Geneva, Switzerland. The close correlation between IL-6 and number of active joints and other signs of disease activity in experimental models is attributed to the key role of sIL-6R trans-signaling in RA progression.
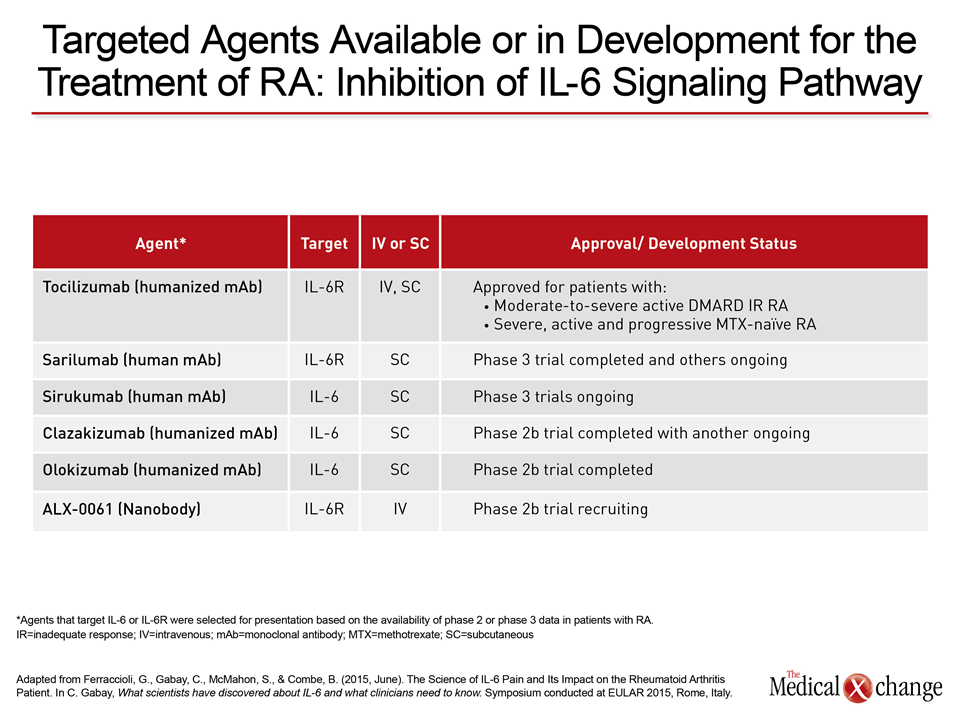
Attention to IL-6 inhibition as a therapeutic target in RA is being intensified by a large agent development program in this area, according to Dr. Gabay. The new agents represent related strategies against a target already proven to be viable with tocilizumab, the first agent in this therapeutic class (Table 1).
MOBILITY Trial: 52-week Results
Of these IL-6 inhibitors, the 52-week data from the multinational MOBILITY trial with sarilumab were presented at EULAR 2015. Of the most significant findings, the disease control was as good or better for most measures of disease activity after one year on therapy relative to that observed at 24 weeks. The long-term control reinforces both the clinical value of the therapy and the importance of IL-6 as a target.
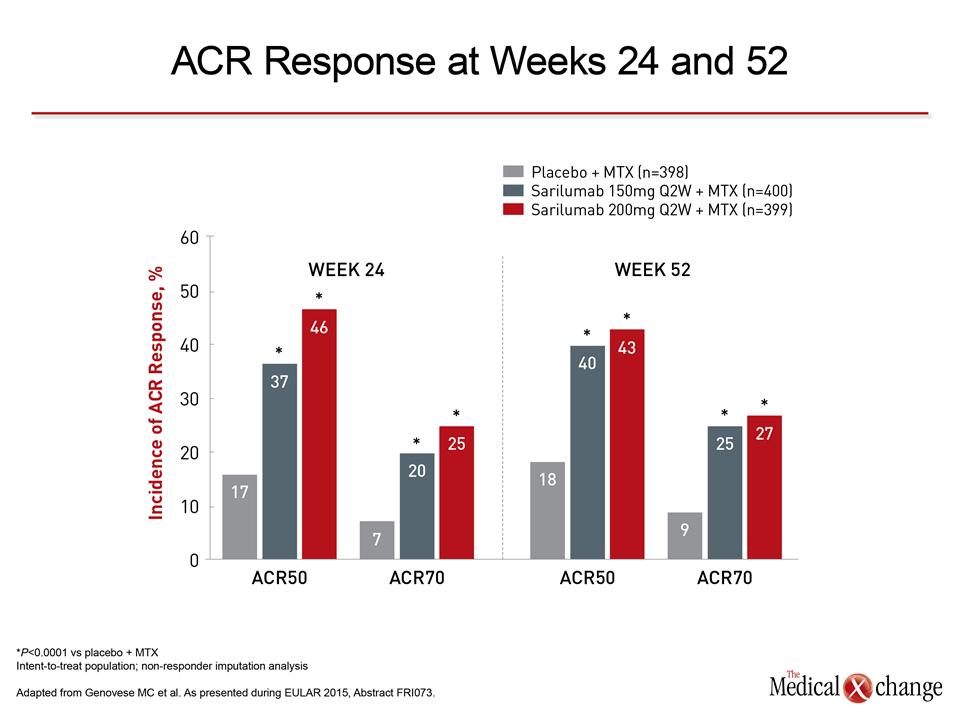
The intent-to-treat analysis of the MOBILITY trial included 1197 moderate-to-severe RA patients randomized equally to one of three groups: 1) placebo subcutaneous (SC) injections every 2 weeks (Q2W) plus methotrexate (MTX); 2) sarilumab 150 mg SC Q2W plus MTX; or 3) sarilumab 200 mg SC Q2W. Of the variety of 52-week MOBILITY datasets presented at EULAR, including safety and quality of life (QOL), the sustained disease control, as well as the specific activity in patients entering the study with severe disease was the most notable.
Overall, the proportions achieving 20%, 50%, or 70% improvements in American College of Rheumatology criteria (ACR20, ACR50, and ACR70) from baseline were similar or climbed modestly from 24 weeks to 52 weeks on either dose of sarilumab. In the group with severe disease, which represented 82% of the patients enrolled, the relative improvements in measures of disease activity were generally greater than those observed in patients with moderate disease with no increase in relative risk of adverse events even at the higher of the two doses.
“Adverse events and serious adverse events were more frequent than on placebo but similar in sarilumab groups with moderate and severe disease,” reported the principal investigator on this analysis, Dr. Mark C. Genovese, Co-Chair, Division of Immunology and Rheumatology, Stanford University Medical Center, Stanford, California. According to Dr. Genovese, the most common adverse event among patients taking sarilumab, other than injection site reactions, was infection, but risk of infection was not correlated with treatment duration.
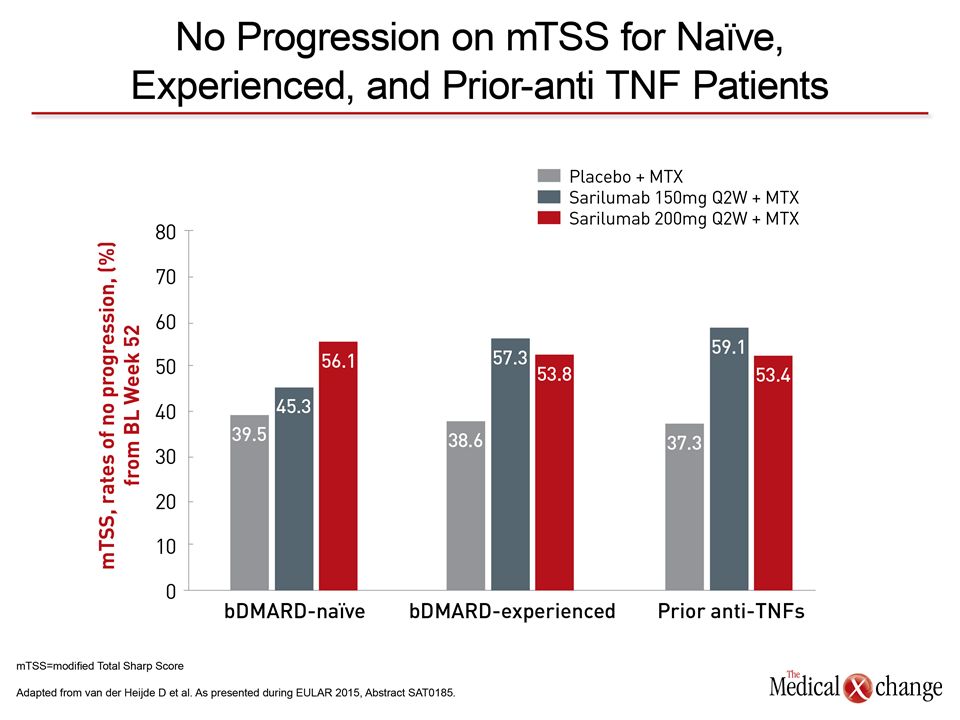
The relative ability of highly targeted IL-6 inhibitors to prevent the progressive joint deterioration associated with RA is an area of intensive investigation. A post-hoc radiographic analysis from MOBILITY was encouraging (Fig. 1). Of the promise of biologics, improved symptom control is important, but preserving the integrity of joints may be the ultimate measure of effective treatment.
Conclusion
There is a variety of evidence to suggest that inhibition of IL-6 is a more promising and specific target for the control of RA and perhaps other inflammatory joint diseases than TNF-α. Whether or not this is proven with an expanding selection of IL-6 inhibitors, the substantial proportion of patients not adequately controlled on current therapeutic options encourages an expansion of treatments with proven efficacy.
Additional Slides
Figure 2 (Fig. 2).