RESPIROLOGY
European Respiratory Society (ERS) International Congress 2015
Concrete Steps Taken to Base Severe Asthma Treatment on Molecular Rather than Clinical Phenotypes
Amsterdam – Subgrouping patients according to immune cell composition in the sputum is expected to revolutionize management of severe asthma, according to a series of studies presented at the ERS International Congress 2015. Asthma has long been understood as a heterogeneous condition, but there has been recent progress in using sputum to subgroup patients by molecular phenotype for treatment selection. One study suggested the inflammatory cell composition in sputum might direct treatment choice, while two late breaker studies with novel agents found blood and sputum eosinophil counts to be a predictor of response.
Despite substantial heterogeneity, the diagnosis of asthma is traditionally based on signs and symptoms. This may be both inefficient and counterproductive. New evidence demonstrates heterogeneity in the underlying pathophysiology. A collaborative research effort called U-BIOPRED (Unbiased BIOmarkers in PREDiction of respiratory disease outcomes) has distinguished three stable phenotypes primarily by immune cell composition in the sputum.
Individualized Asthma Treatment Expected
“We believe that our work, dividing severe asthmatics into meaningful categories, is the first step towards being able to provide each sufferer with optimal individualized treatment,” reported a team of investigators from the European Institute of Systems Biology and Medicine, Lyon, France. A research engineer at the institute, Diane Lefaudeux, presented the findings at the ERS International Congress 2015. Dr. Ian Adcock, Head, Molecular Cell Biology Group, National Heart & Lung Institute, Imperial College, London, UK, was a senior author.
“We now believe that there may be a number of causes of asthma, because we have been able to isolate distinct phenotypes in those with severe disease.” Ms. Diane Lefaudeux
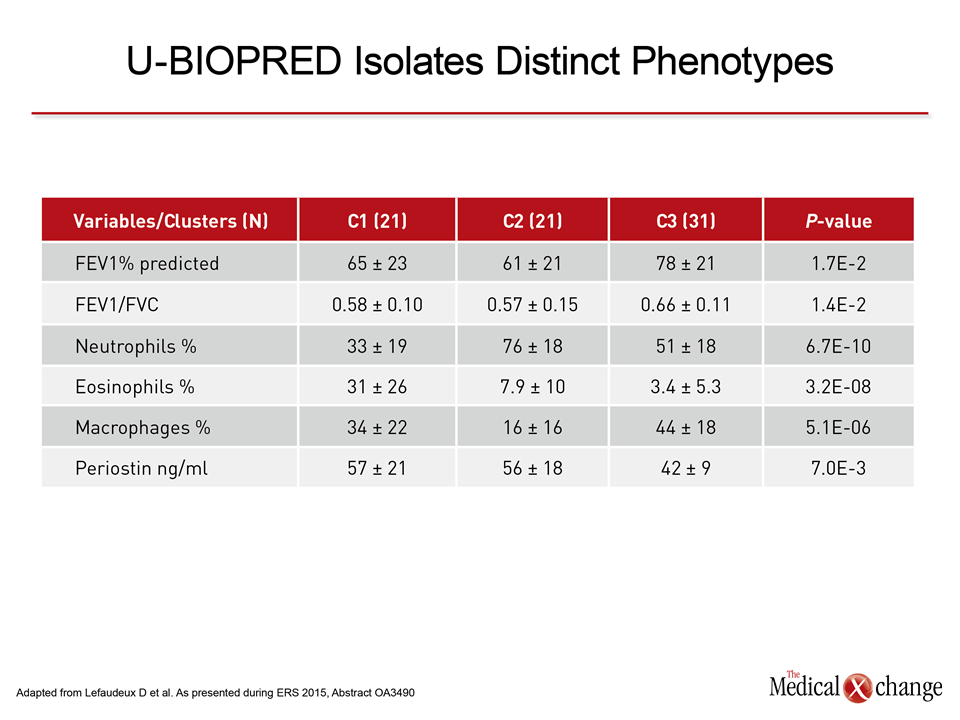
In the U-BIOPRED study, which has received both private and public funding, patient sputum samples were collected from adults and children with severe asthma. The sputum was subjected to a broad array of analyses, including gene expression and proteomics, in the context of disease expression. Of variables most valuable for clinically-relevant patient subtypes, immune cell composition emerged as among the most valid. Largely on the basis of immune cell composition, the authors characterized three clusters of patients, labeled C1, C2, and C3, with features that may be useful for guiding therapy. “C1 has a more pronounced Th2 [T-helper type 2] phenotype than C2 and C3, as defined by the percentage of sputum eosinophils and higher periostin levels,” Ms. Lefaudeux reported. In contrast, C2, which had similar severity based on FEV1% predicted and the FEV1/FVC ratio, had low eosinophil counts but highly-elevated neutrophils (Table 1). The C3 phenotype, according to Ms. Lefaudeux is “clinically milder, with higher FEV1% predicted and FEV1/FVC ratio.”
Late Breaker Studies with Monoclonal Antibodies
These data are consistent with efficacy data from new monoclonal antibodies in the treatment of asthma. Both were presented here as late breakers. In one, the study agent was reslizumab, which targets interleukin-5 (IL-5). Two studies were pooled with a focus on late-onset asthma (>40 years of age). In the other, the study agent was dupilumab, which targets the alpha receptor of interleukin-4 (IL-4Rα). In this phase 2b study, patients were enrolled with uncontrolled asthma despite optimized treatment with inhaled medications, including corticosteroids.
“Late-onset asthma with elevated blood eosinophils is a distinct, difficult-to-treat asthma phenotype for which there is an unmet need for improved therapy.” Dr. Guy Brusselle
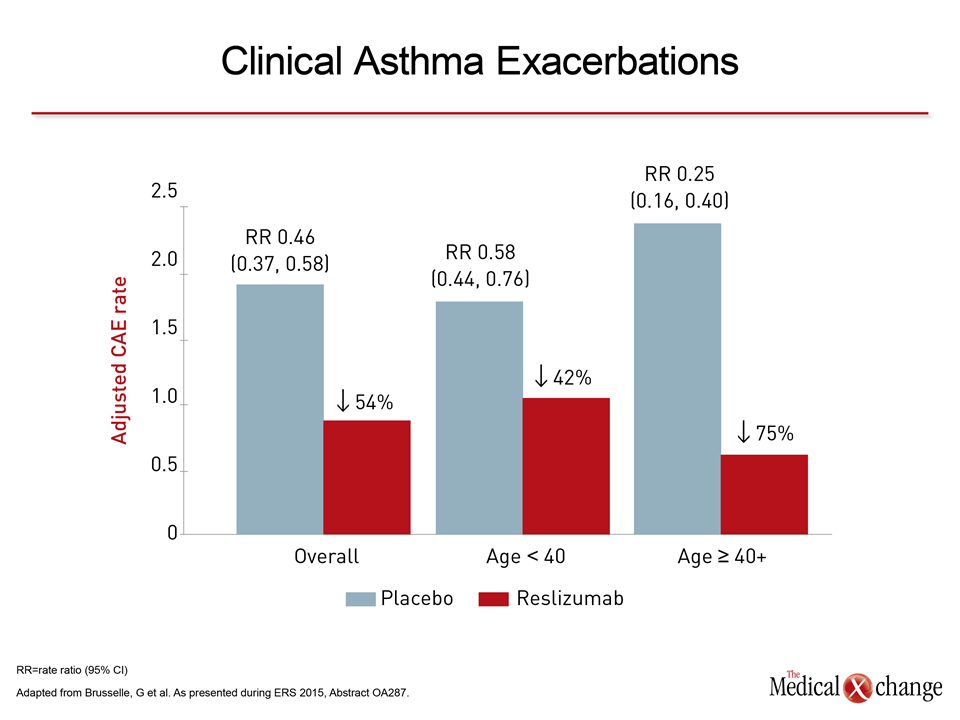
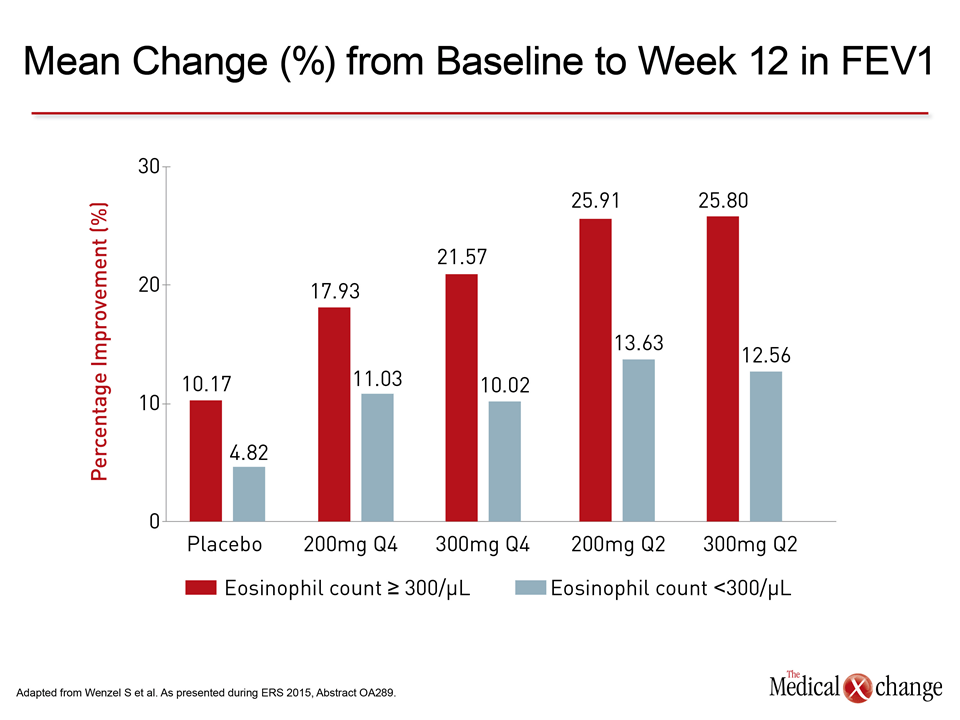
In the placebo-controlled studies with reslizumab, patients were required to have a blood eosinophil count of ≥400/μL. According to the principal investigator, Dr. Guy Brusselle, Department of Respiratory Medicine, Ghent, Belgium, this is a particularly “difficult-to-treat phenotype.” Both studies evaluated 3 mg/kg of reslizumab administered every four weeks. One randomized 476 patients and the other 477 patients. Although the active agent produced large reductions in the rate of asthma exacerbations relative to placebo in all patients, the reductions were larger in those with late-onset asthma (Fig. 1). Moreover, these support U-BIOPRED evidence that eosinophil upregulation may be a clinically-relevant discriminator. In the placebo-controlled study with dupilumab, 776 patients with uncontrolled asthma were randomized to add-on therapy with either 200 or 300 mg of dupilumab administered either every 2 weeks or every 4 weeks. The primary endpoint was change in FEV1 from baseline at week 12 although follow-up continued out to 24 weeks. Benefit was greatest in patients with an elevated sputum eosinophil count (≥300 μL) relative to those with a lower sputum eosinophil count (Fig. 2). Although most patients with asthma do improve with anti-inflammatory therapies, often coupled with bronchodilators, the clinically-important minority of patients who have an inadequate response to these agents has fueled efforts to develop targeted agents for specific molecular pathways. Inhibitors of IL-5 and IL-4 are known mediators of Th2 and upregulation of eosinophils. These therapies are part of an effort to develop more targeted and personalized medicine in asthma control.
Conclusion
The U-BIOPRED sputum “handprinting” project was initiated on the premise that both available and experimental asthma therapies “do not work in all people with this diagnosis,” Ms. Lefaudeux reported. Although Ms. Lefaudeux suggested more data are needed to develop practical tools for phenotyping, the data from late breaking studies with reslizumab and dupilumab encourage these efforts.