cardiology
2015 Canadian Cardiovascular Congress (CCC)
Debating North American Cholesterol Guidelines and the Role of PCSK9 Inhibitors
Toronto – Low-density lipoprotein cholesterol (LDL-C) goals for the treatment of dyslipidemia differ among US and Canadian guidelines. At the 2015 CCC, an expert from the US debated with his Canadian counterparts on how goals are best defined on the basis of randomized controlled trials. This debate is timely. Treatment goals, particularly in high-risk patients, are more frequently achieved with PCSK9 inhibitors than with previous options. Defining goals according to risk is an essential step toward the ultimate objective, which is to reduce cardiovascular (CV) morbidity and mortality.
Background
Randomized clinical trials (RCTs) show that lowering LDL-C reduces rates of cardiovascular (CV) events. However, the level of LDL-C at which no further risk reduction can be achieved has never been determined, and current US and Canadian guidelines differ in their recommendations. In the US, no specific LDL-C target has been identified. Rather, the guidelines encourage relative reductions in LDL-C from baseline based on multiple risk factors. In Canada, the LDL-C goal for high-risk patients is <2.0 mmol/L or ≥50% reduction from baseline.
US versus Canadian Guidelines
Providing the US perspective in a debate at the 2015 CCC, Dr. Deepak L. Bhatt, Executive Director, Interventional Cardiovascular Programs, Harvard Medical School, Boston, MA, argued that CV risk in relationship to LDL-C levels requires a “very complex equation” that takes into account such factors as adherence, lifestyle medication, and therapies. He defended the decision by the authors of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guidelines to avoid defining a specific LDL-C target.
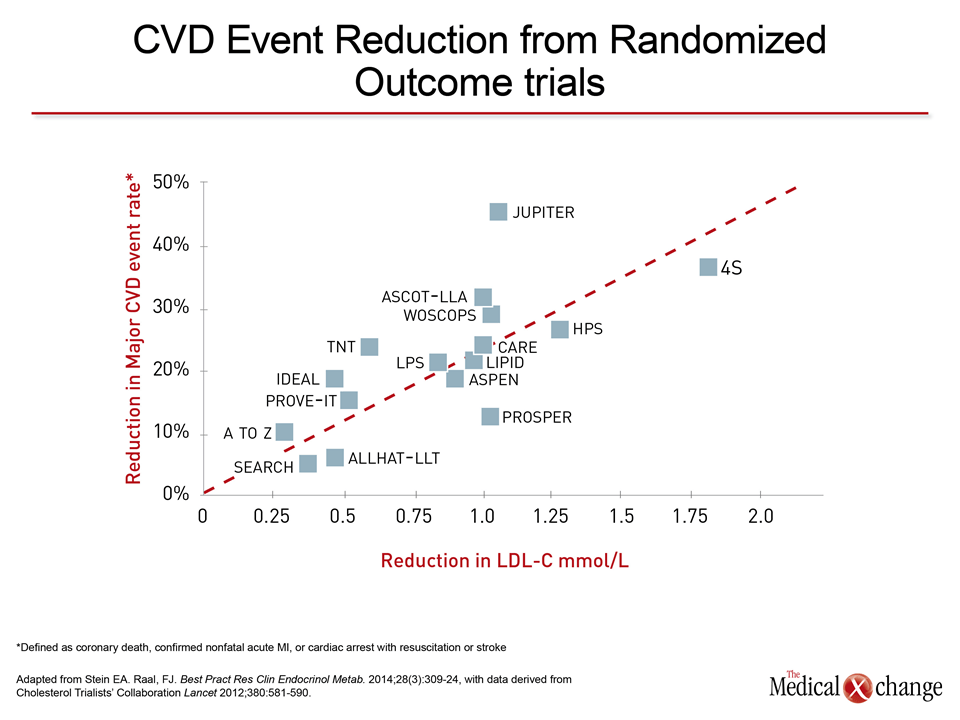
“Until we have RCT data showing that any particular compound reduces CV events, we should still anchor our decisions to RCT data and not to some magical mystical LDL number,” Dr. Bhatt said. Although he acknowledged that RCTs have correlated LDL-C and reductions in CV events, he emphasized that these are on a continuum not linked to a specific LDL-C value (Fig. 1).
“At the end of the day, we need to get the LDL as low as safely possible and we need guidance.” Dr. Shaun Goodman
Rather than defining the LDL-C goal as a specific number, the ACA/AHA guidelines call for LDL-C reductions of 30%–50% or >50% depending on risk factors such as atherosclerotic cardiovascular disease (ASCVD), “out-of-control” LDL-C, age, diabetes mellitus and 10-year ASCVD risk of ≥7.5%.
Providing thedefence for Canadian Cardiovascular Society guidelines, Dr. Shaun Goodman, Associate Head, Cardiovascular Medicine, St. Michael’s Hospital, Toronto, said that it is appropriate to provide real-life guidance to clinicians. Even with risk-based reduction ranges, he indicated that targets help drive clinicians to intensify therapy in order to achieve LDL-C levels associated with risk reductions relative to higher LDL-C levels in RCTs. “Can we rely on a 50% lowering? Wouldn’t you like to be in an even lower group if you had CV disease?” Dr. Goodman asked. He noted that there is good evidence that LDL-C <1.8 mmol/L is associated with CV risk reductions relative to higher levels in high-risk patients, making at least this degree of LDL-C lowering a reasonable goal even if even further reductions provide further risk reductions.
“Both sets of guidelines need to be updated because there is increasing evidence-based support for non-statin therapy”.
Dr. Shaun Goodman
Both the ACC/AHA and the Canadian treatment guidelines have been primarily informed by the large, multicenter trials conducted with statins over the past 20 years. Although the authors of the ACC/AHA and Canadian guidelines drew different conclusions about the clinical application of these data “both sets of guidelines need to be updated because there is increasing evidence-based support for non-statin therapy,” according to Dr. Goodman.
PCSK9 Inhibitors
Although this non-statin evidence includes a trial published earlier this year with ezetimibe, the multiple trials with the PCSK9 inhibitors alirocumab and evolocumab have greatly increased evidence that relative reductions in LDL-C correlate with relative reductions in CV events regardless of the treatment with which they are achieved.
In the ODYSSEY LONG-TERM study, for example, LDL-C was reduced by 62% on alirocumab relative to placebo (Robinson JG et al. N Engl J Med 2015;372:1489-99). Although CV risk reductions are being tested as a primary outcome in the ongoing ODYSSEY OUTCOMES trial, a post-hoc analysis of the LONG-TERM trial associated this reduction in lipids with a 52% reduction (P=0.02) in a composite ofCV events that included death from coronary heart disease.
Similar data were presented with evolocumab in the OSLER study, which was published simultaneously with ODYSSEY LONG-TERM (Sabatine MS et al. N Engl J Med 2015;372:1500-9). Overall, the trial data of the efficacy for lipid lowering with these drugs “is incontrovertible,” according to Dr. Jean Genest, Professor of Medicine, McGill University, Montréal, Québec.
Differences in lipid-lowering effect, if any, from the PCSK9 inhibitors is unclear, according to Dr. Milan Gupta, Associate Clinical Professor, Department of Medicine, McMaster University, Hamilton, Ontario. “Both agents have the ability to lower cholesterol remarkably by at least 60 to 70% with pretty equivalent doses, but the advantage of alirocumab is that with the [optional] every two-week dose of 75 mg, one still gets a very robust 40 to 50% LDL lowering for those patients where there may be some concern about achieving very low LDLs,” Dr. Gupta said.
The two recently-published PCSK9 trials did differ in design, according to Dr. Gupta. Specifically, he pointed out that the single alirocumab RCT was double-blind while the trial with evolocumab employed an open-label design. Moreover, the trial with alirocumab had a longer median treatment time and a less heterogeneous patient population, including more patients with a history of CV disease, more patients with a diagnosis of heterozygous familial hypercholesterolemia, and more patients who were also taking high-dose statin therapy.
The Future
Guidelines for CV risk reductions with lipid-lowering, which were largely based on statin trials, are likely to be revisited with more evidence that non-statin therapies also provide CV risk reductions. In particular, ongoing outcomes trials with PCSK9 inhibitors have the potential to redefine goals.