Rheumatology
American College of Rheumatology (ACR) 2015 Congress
Expansion in Biologic Option Critical For Non-Responders to TNF Inhibitors
San Francisco – Evidence that newer biologics are effective for restoring benefit in patients with rheumatoid arthritis (RA) who have lost response to an initial targeted therapy has been expanded by new data presented at the 2015 ACR Congress. Despite the major contribution made by tumor necrosis factor (TNF) inhibitors—and subsequently by other biologics—to the control of moderate to severe RA, new options are needed when initial therapy fails. Data presented here confirm that newer investigational biologics provide high levels of response in patients who have progressed on a previous biologic.
In addition to TNF inhibitors, there are now targeted therapies for interleukin-6 (IL-6), interleukin-1 (IL-1) and the JAK pathway. Agents in each class control inflammation and symptoms associated with RA. Yet, approximately 30% of patients do not respond initially to a first-line TNF inhibitor, and many lose response over time, creating a need for additional options.
Response in TNF Failures
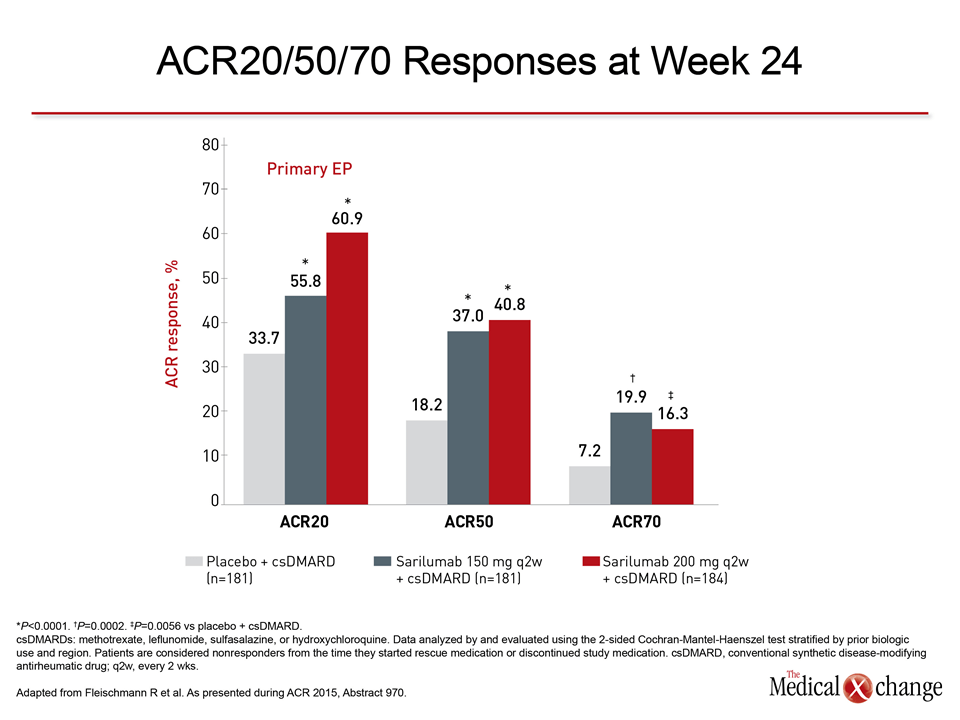
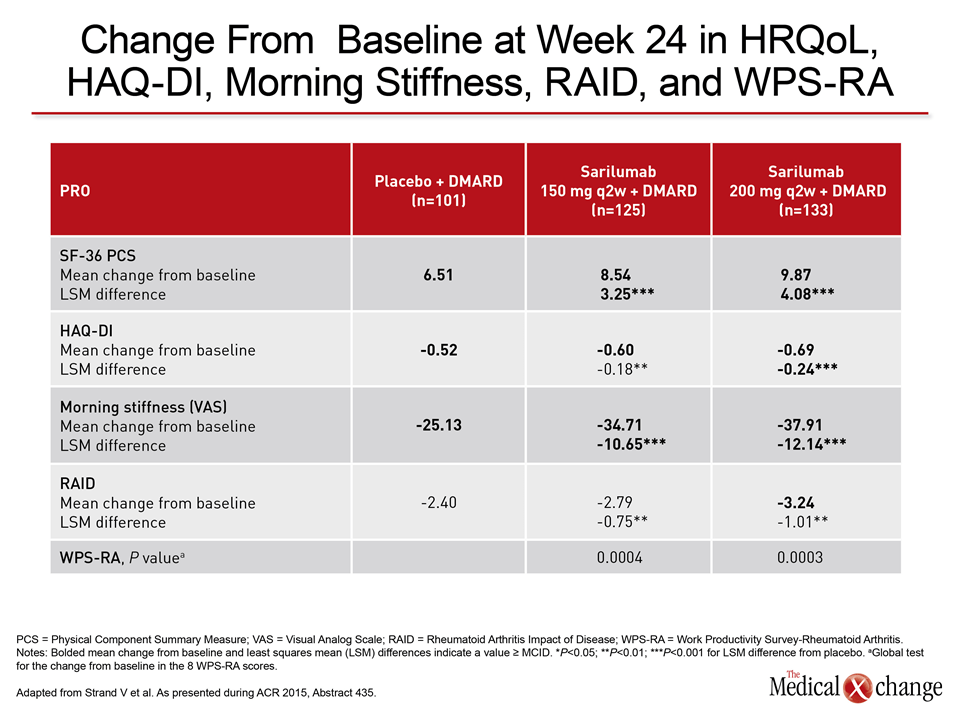
At the ACR, data were updated on a Phase 3 trial with an investigational biologic called sarilumab that targets the IL-6 receptor. The trial was designed specifically to evaluate efficacy in those who have failed, lost response, or become intolerant to at least one anti-TNF therapy, according to Dr. Roy Fleischmann, University of Texas Southwestern Medical Center, Dallas. All patients entered the study and remained on a non-biologic disease-modifying antirheumatic drug (DMARD). Relative to placebo plus a DMARD, either of two study doses of sarilumab plus a DMARD achieved “statistically significant and clinically meaningful changes” in every measure evaluated, according to Dr. Fleischman. This included a near doubling of the proportion of patients achieving an ACR20 response, which was a co-primary outcome. The relative advantage was even greater for the more rigorous ACR50 and ACR 70 responses (Fig. 1). For the other co-primary endpoint of Health Assessment Questionnaire Disability Index (HAQ-DI) as well as the secondary endpoints presented by Dr. Fleischman, such as the Clinical Disease Activity Index (CDAI) and the Disease Activity Score-28 (DAS28), there was also a consistent advantage for either treatment dose over placebo. Data were also presented from the TARGET study, showing an advantage of sarilumab in this population of TNF inhibitor failures for relative improvement in a broad array of quality of life measures, including morning stiffness on a visual analog scale, Work Productivity Survey-Rheumatoid Arthritis (WPS-RA), Rheumatoid Arthritis Impact of Disease (RAID), and the Short Form 36 Physical Component Summary (SF-36 PCS) (Table 1).
In-depth Data from Phase 3 Trial
The key entry criteria for the multinational TARGET trial was active moderate-to-severe RA, prior failure or intolerance to at least one anti-TNF therapy, and a C-reactive protein (CRP) ≥ 8 mg/L. Patients were also required to be on a stable DMARD for at least 6 weeks prior to enrolment. The 546 participants were randomized to placebo, 150 mg sarilumab administered every 2 weeks, or 200 mg sarilumab administered every 2 weeks. Top line results of TARGET were presented earlier this year, but Dr. Fleishman provided the first in-depth and detailed summary of both efficacy and safety. The significance of the study is the expansion of evidence that the expanding array of targeted therapies will offer opportunities to control moderate-to-severe RA in those who do not or no longer respond to TNF inhibitors. The only currently approved biologic targeted at the IL-6 receptor, tocilizumab, has also demonstrated activity in TNF failures, but more choices are needed. Drugs within classes are not interchangeable. Sarilumab, for example, is a fully humanized monoclonal antibody offering the potential for lower likelihood neutralizing antibody (NAB) formation, but agents targeting IL-6, like those targeting TNF, may differ in other clinically-relevant ways. The safety data from TARGET has been reassuring. Although treatment discontinuations due to adverse events was higher on both the 200 mg (9.2%) and 150 mg (7.7%) doses of sarilumab relative to placebo (4.4%), adverse events considered serious were the same for placebo and the 150-mg dose of sarilumab (3.3%) and only slightly higher on the 200-mg dose (5.4%). There were no deaths. The most common treatment-emergent adverse events attributed to sarilumab were infection, neutropenia, and increases in alanine aminotransferase level. According to Dr. Fleischman, the greater activity of the higher dose probably warrants the modest increased risk of an adverse event.
Benefit-to-Risk of Higher Dose
“I would prefer to use 200 plus methotrexate. If a patient does have an adverse event, I would reduce to 150 because I think the risk-to-benefit would support that,” Dr. Fleischman reported. Biologics act directly on key mechanisms of the signaling that drive RA and other autoimmune diseases characterized by inflammation. Although TNF inhibitors provided the proof that targeted therapies can control disease by downregulating cytokines, the value of IL-6 as an important target for control of inflammation is now also well established. It was further expanded by new data at the ACR from the previously reported Phase 3 SARIL-RA-MOBILITY trial, which randomized patients with an inadequate response to methotrexate to sarilumab or placebo. The large advantage of sarilumab on the primary endpoints has driven further development of this molecule. At ACR 2015, the benefit of sarilumab relative to placebo in SARIL-RA-MOBILITY was placed into a context of inflammatory markers by Prof. Maxime Dougados, Paris-Descartes University, France. He noted the results are wholly consistent with the clinical effects observed. “Inhibition of IL-6 signaling via sarilumab was associated with changes in parameters associated with chronic inflammation, including a decrease in CRP, an increase in hemoglobin, a normalization of albumin, a normalization of fibrinogen, and an increase in total and LDL cholesterol,” Dr. Dougados reported.
Conclusion
Biologics have represented a major advance for control of RA inadequately responsive to DMARDs, but there is an urgent need for more targeted agents because of the sizeable proportion of patients with primary treatment failure to TNF inhibitors or who develop resistance or intolerance of first-line biologics. New data with an investigational IL-6 inhibitor suggest progress is being made.