Respirology
American Thoracic Society (ATS) 2016 International Conference
Landmark FLAME Data Support Guideline Change in COPD Patients with a History of Exacerbations
San Francisco – In patients with chronic obstructive pulmonary disease (COPD), two long-acting bronchodilators (LABA/LAMA) reduce the rate of exacerbations when compared to a single long-acting bronchodilator (LABA) plus an inhaled corticosteroid (ICS), according to a newly-completed multinational trial that compared these strategies over 52 weeks. Several experts characterized the data as practice changing.
FLAME Results
In this trial, called FLAME, which randomized 3362 patients, a single-dose combination of a long-acting beta agonist (LABA) plus a long-acting muscarinic antagonist (LAMA) was found more effective than a single dose combination of a LABA and inhaled corticosteroid (ICS), which is guideline-recommended. This included the primary endpoint of exacerbations but also an extensive list of secondary endpoints. According to the principal investigator of the trial, Dr. Jadwiga A. Wedzicha, National Heart and Lung Institute, Imperial College, London, UK, “we now have the evidence to change the treatment algorithms.”
“We now have the evidence to change the treatment algorithms.”
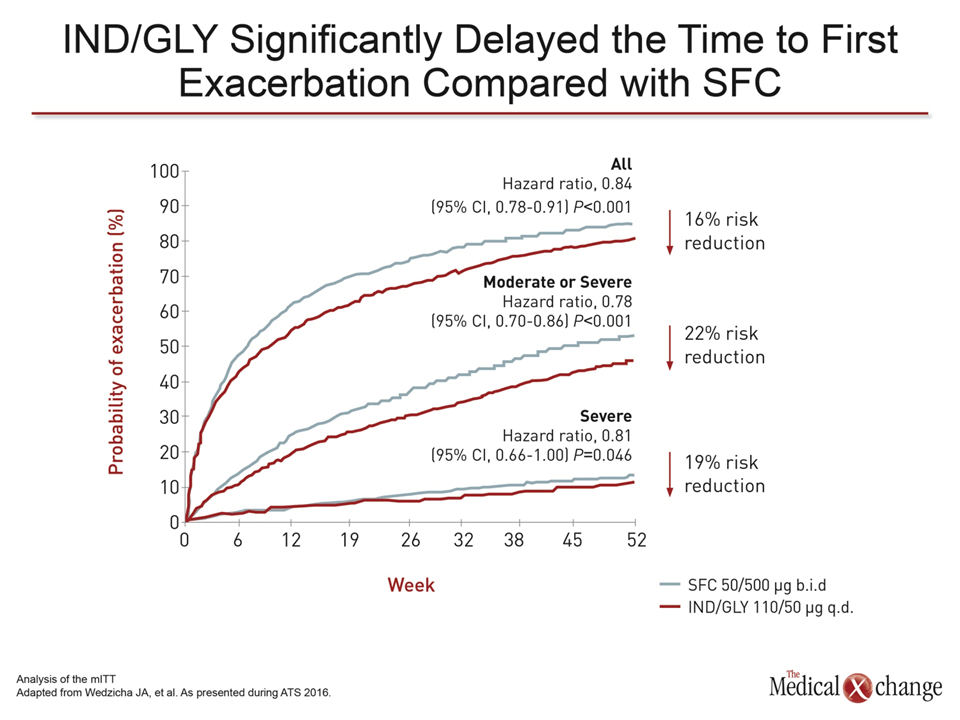
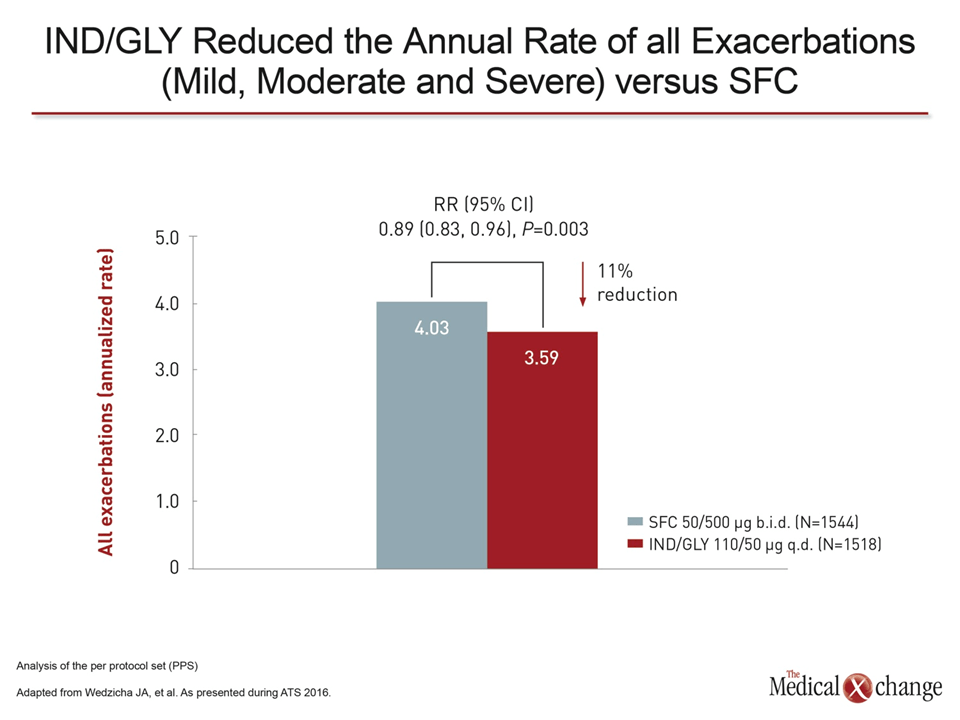
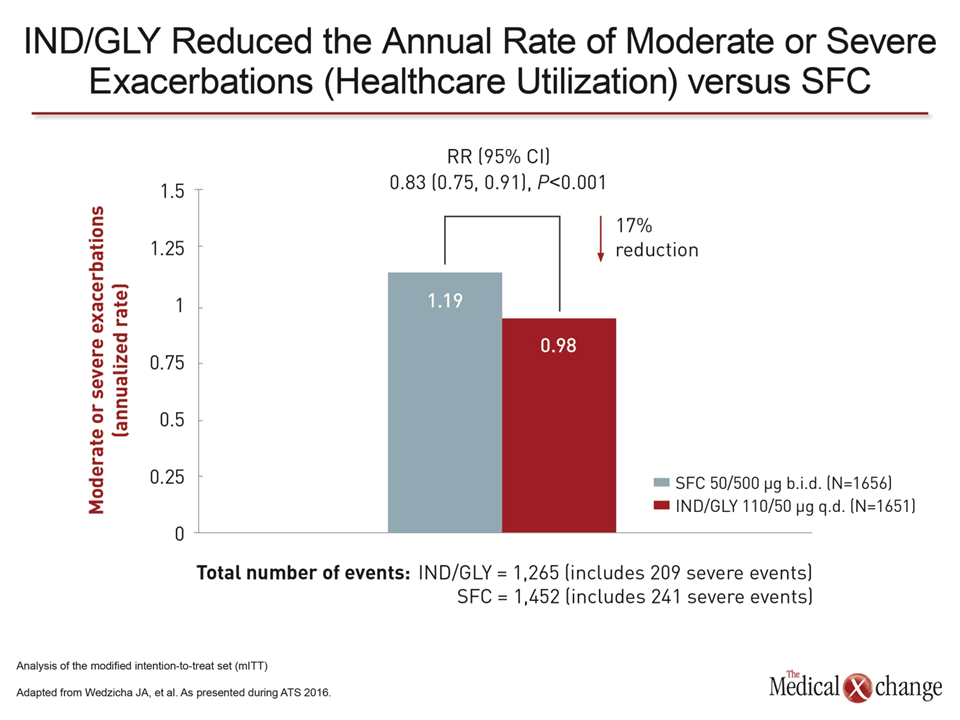
The trial data were presented in brief at the American Thoracic Society (ATS) International Conference 2016 and simultaneously published in the New England Journal of Medicine (Wedzicha JA et al; May 15 epub ahead of print). COPD patients with a history of exacerbations were randomized to a fixed-dose, once-daily combination of the LABA indacaterol plus the LAMA glycopyrronium (IND/GLY) or a fixed dose twice-daily combination of the LABA salmeterol plus the ICS fluticasone (SFC). For the primary endpoint of exacerbations at 52 weeks, IND/GLY provided an 11% relative reduction (P=0.003) (Fig. 1). IND/GLY was also favored over SFC for such secondary outcomes as rate of moderate to severe exacerbations (17%), time to first exacerbation, and time to first severe exacerbation. In addition, the bronchodilator combination was associated with a significantly lower rate of pneumonia (3.2% vs. 4.8%; P=0.017), improved lung function at the end of 52 weeks, and a consistent advantage over SFC when the study population was stratified for eosinophil count greater or less than 2%.
“This study takes us back to our roots by placing the emphasis in COPD back on bronchodilation.”
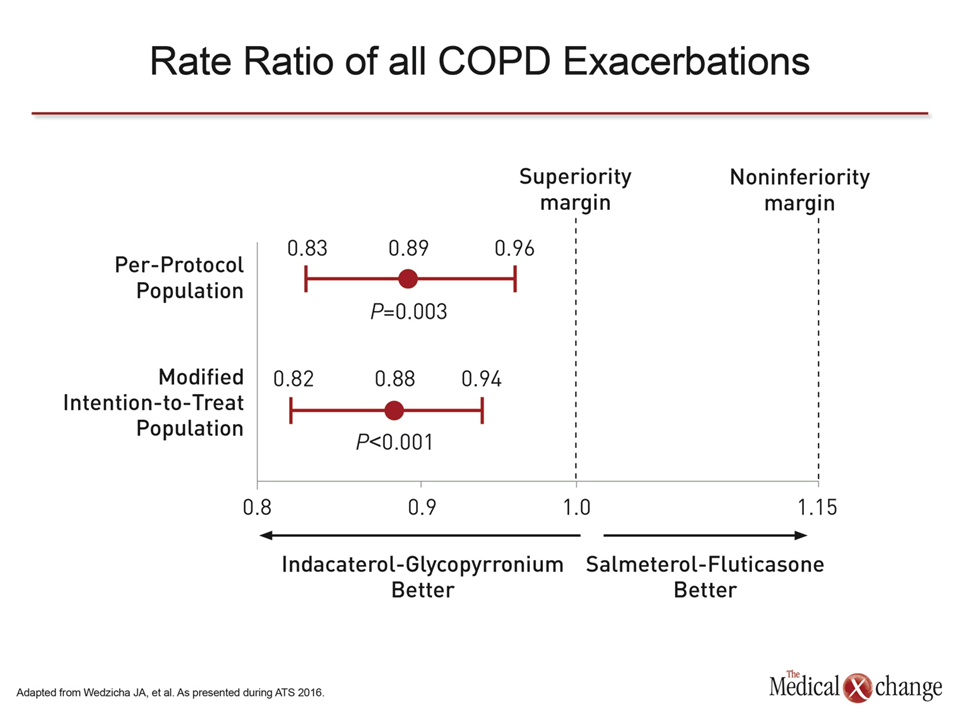
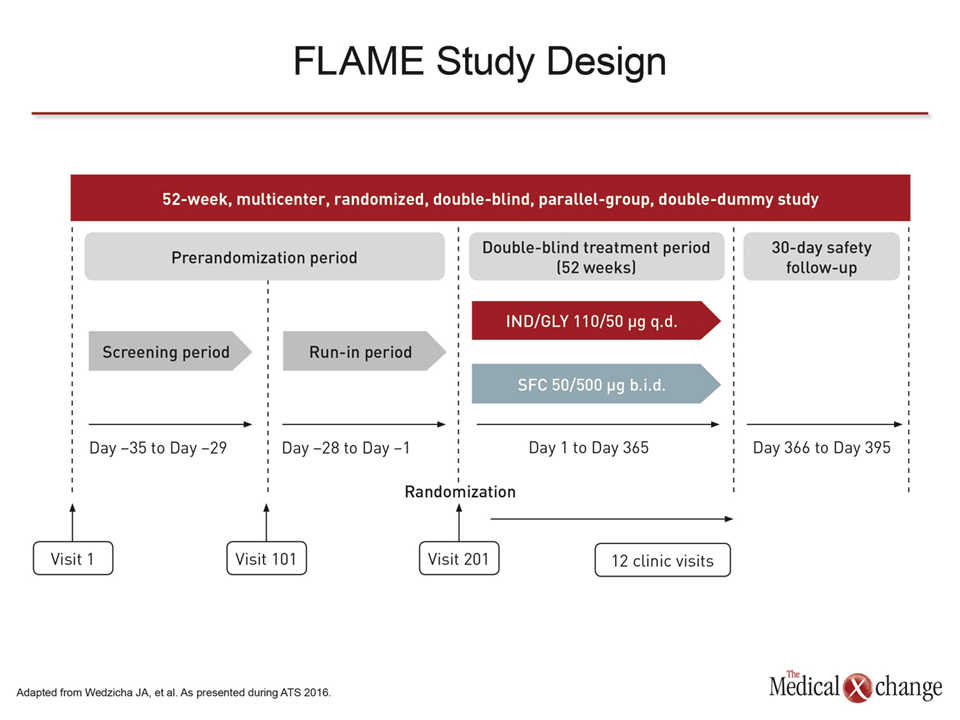
“This study takes us back to our roots by placing the emphasis in COPD back on bronchodilation,” commented Dr. Kenneth R. Chapman, Director, Asthma and Airway Centre, University Health Network, Toronto. A co-author of FLAME, Dr. Chapman noted that although the ICS component of combination therapy is fundamental to control of asthma, the anti-inflammatory activity of ICS in COPD has never been well established independent of bronchodilation. The head-to-head FLAME study now establishes “that the frequent exacerbator does better on a LABA/LAMA than SFC.” In FLAME, the key eligibility criterion was one or more COPD exacerbations requiring antibiotics, systemic corticosteroids, or hospitalization in the previous 12 months. Patients were required to be at least 40 years of age and to have grade 2 or higher COPD on the Medical Research Council scale. Other criteria, such as a FEV1 of at least 25% but less than 60%, were consistent with other COPD studies. Patients were randomized at 356 sites in 43 countries including Canada. The once-daily inhaler in the experimental arm contained 110 mcg of IND and 50 mcg of GLY. In the control arm, the twice-daily inhaler contained 50 mcg of salmeterol and 500 mcg of fluticasone. Initiated as a non-inferiority comparison, the FLAME trial design permitted superiority to be evaluated under prespecified criteria. At the end of 52 weeks, the advantage of IND/GLY over SFC triggered this superiority evaluation. A highly significant and similar advantage for IND/GLY relative to SFC for the primary endpoint was observed on both modified intention-to-treat (mITT) or per protocol analyses (Fig. 2).
Subgroup Analyses
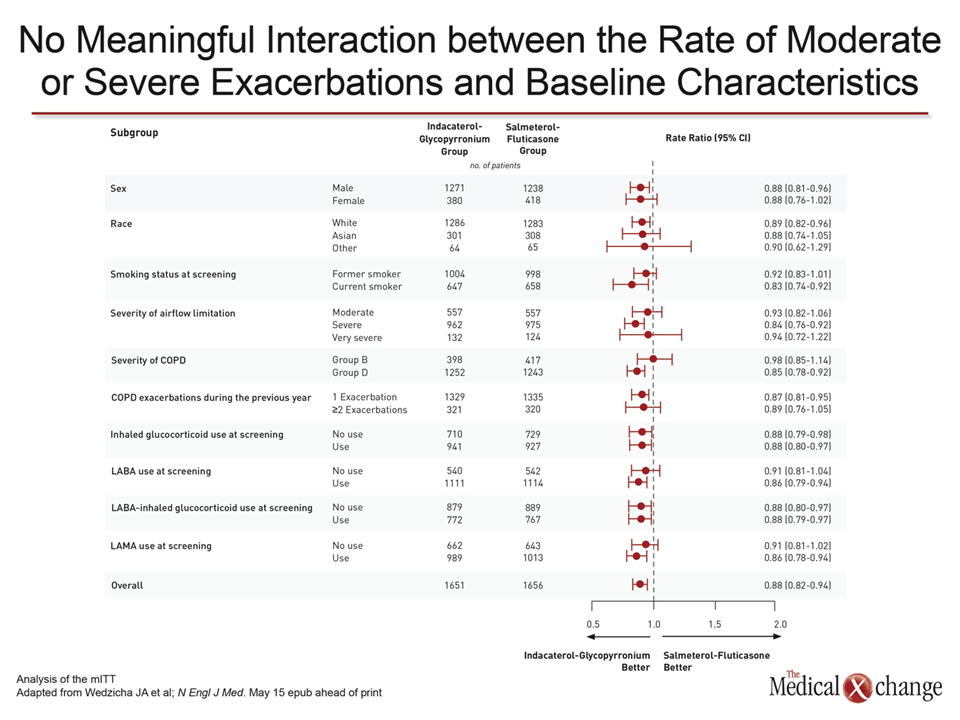
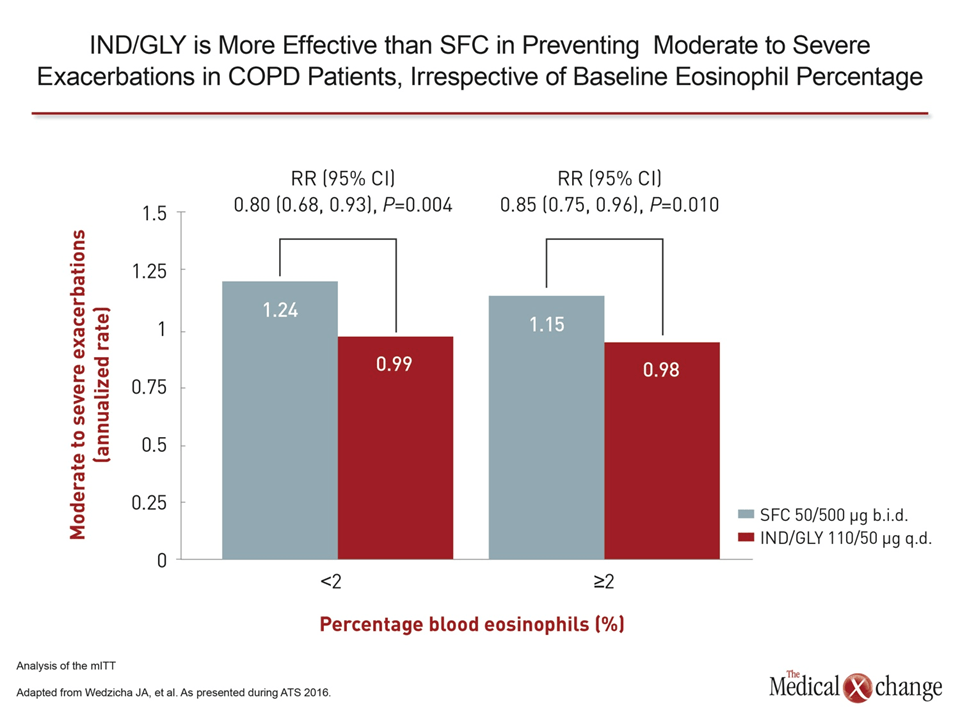
Looking across subgroups defined by age, smoking status, severity of airflow limitation, severity of COPD, previous exposure to ICS or other COPD treatments, and one versus 2 or more exacerbations prior to study entry, the reduction in the rate of exacerbations remained numerically superior for IND/GLY relative to SFC (Fig. 3). At the time that FLAME was designed more than 5 years ago, eosinophilia was not yet considered a potentially important variable for prognosis or response to COPD treatment. However, in the context of several recently-published studies suggesting that LABA/ICS combination inhalers perform better in patients with elevated eosinophil counts, typically defined as blood levels of ≥2%, the authors of FLAME stratified patients by this measure prior to unblinding. As a result, FLAME became the first study to prospectively compare COPD treatments by this variable, according to Dr. Wedzicha. Again, the relative benefit of IND/GLY was comparable in those with higher or lower eosinophil counts, providing the basis for concluding that there is not a COPD population with an inflammatory subtype more responsive to therapy including ICS. The advantage of IND/GLY over SFC for every endpoint evaluated and across a series of subgroup analyses led Dr. Wedzicha to conclude that FLAME generated “some of the most consistent data I have ever seen in a COPD trial.”
The Incidence of Adverse Events
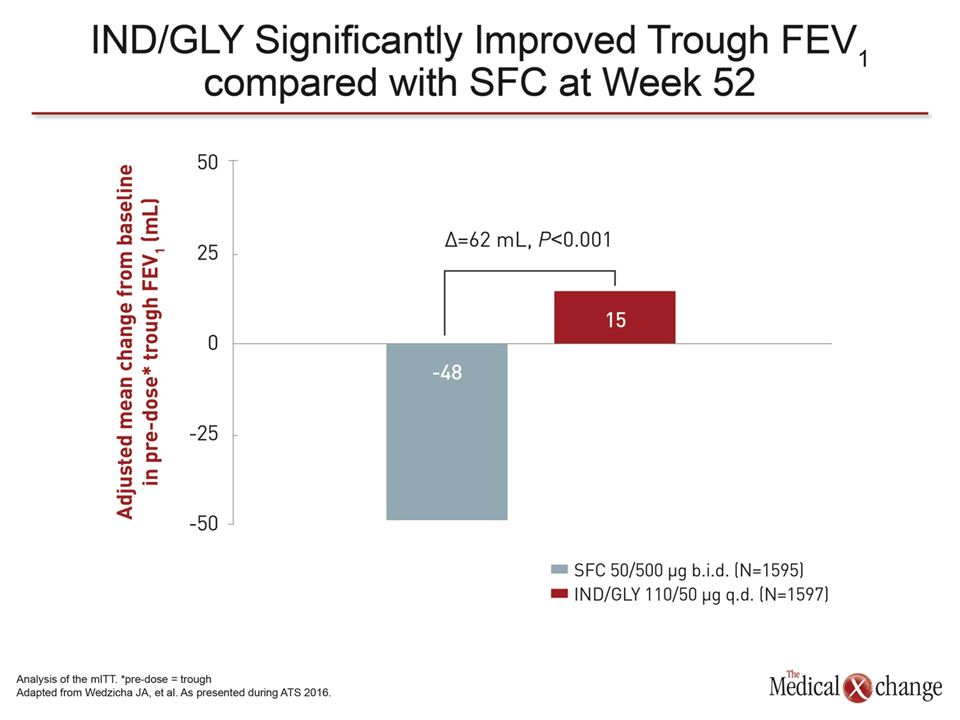
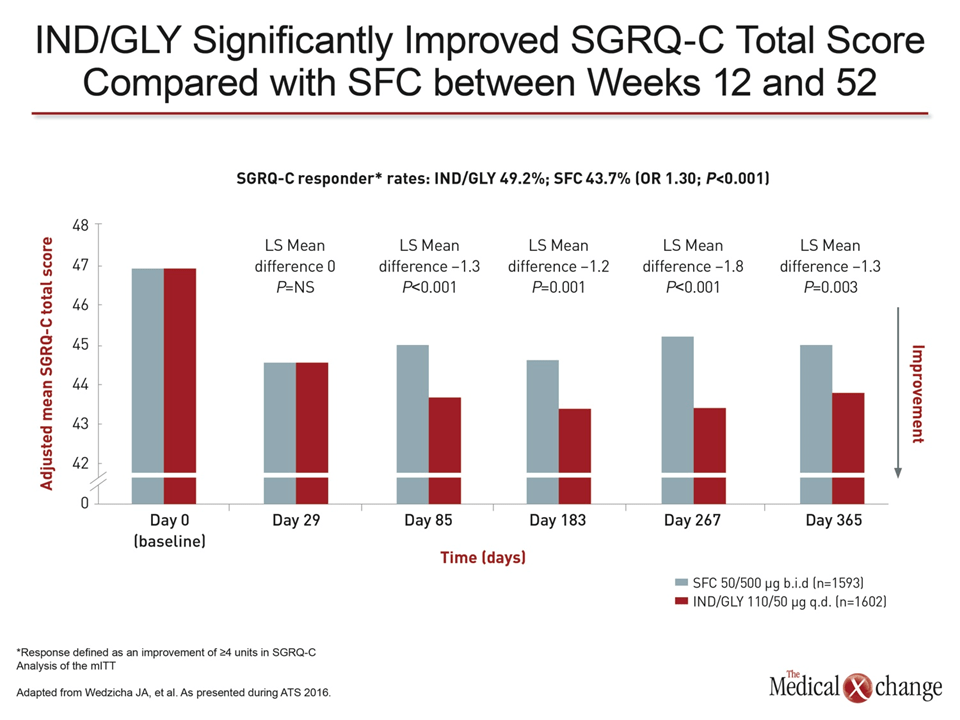
Both treatments were similarly well tolerated. Of rates of specific adverse events other than pneumonia, none differed significantly in the two groups. The rate of oral candidiasis was lower in the IND/GLY group (1.2% vs. 4.8%), but this did not reach statistical significance. The proportion of patients who discontinued for an adverse event in the IND/GLY and SFC groups were comparable for adverse events (7.5% and 8.5%, respectively) and serious adverse events (5.1% and 5.2%, respectively). In addition to the relative reduction in the rate of exacerbations, IND/GLY but not SFC was associated with improvement in lung function from baseline at the end of 52 weeks as measured with FEV1 (Fig. 4). In the context of this and the other benefits observed in FLAME, this may explain the improvement in the St. George’s Respiratory Questionnaire for COPD (SGRQ-C), an instrument for evaluating quality of life. The statistically significant advantage for IND/GLY was consistent overall and at every time point measured from week 12 to 52 (Fig. 5). “A regimen free of inhaled corticosteroids is likely to be better accepted by patients,” Dr. Chapman commented. “Many patients prefer to avoid these drugs because of the concern of side effects.” He called the inclusion of ICS in COPD regimens a “hidden reason for non-compliance.”
What are the Next Steps?
Several current guidelines, such as those provided by the Global Initiative for COPD (GOLD), recommend either LAMA alone or a combination of LABA/ICS as first choice maintenance therapy for patients at risk for recurrent exacerbations. While FLAME provides level 1 evidence that a LABA/LAMA combination is more effective than an ICS-containing combination to prevent exacerbations, several experts agreed that more data are needed to determine when to switch from a single bronchodilator to a combination and what further step is reasonable when patients are inadequately controlled on a dual bronchodilator regimen.
Conclusion
“Is there a benefit of steroids on top of a dual bronchodilator? We do not have that study.”
“Is there a benefit of steroids on top of a dual bronchodilator? We do not have that study,” observed Dr. Chapman. Although he conceded that clinicians are likely to consider adding an ICS agent to dual bronchodilation for a triple-therapy approach to improve control in patients with recurrent exacerbations, he reemphasized that FLAME suggests more studies are needed to reevaluate the contribution of therapies targeted at the inflammatory component of COPD. He suggested that the results of FLAME raise the question of whether ICS is the best strategy to control this form of COPD-related pathology. This same point was made by Dr. Wedzicha, who suggested that new approaches to treating the inflammation of COPD represent “a major unmet need,” calling for the study of new targets in the inflammatory pathway.