Cardiology
National Lipid Association (NLA) 2016 Scientific Sessions
Efficacy and Safety of PCSK9 Inhibitors Now Measured In Years with No Change in Scale of Clinical Benefit
New Orleans – New evidence presented at the NLA 2016 Scientific Sessions demonstrated that PCSK9 inhibitors provide unprecedented control of low-density lipoprotein cholesterol (LDL-C) for as long as patients remain on therapy. After 2 years of follow-up in a phase 3 trial, the reduction in LDL-C with a PCSK9 inhibitor was comparable to those first reported after 24 weeks. In this large multicenter, randomized study, which enrolled patients at high risk of cardiovascular (CV) events, the type and rate of adverse events at 2 years remained low and comparable to rates reported at any earlier time point.
ODYSSEY COMBO II Trial Data
“In high-risk patients, the reductions in LDL-C have been maintained through 2 years of follow-up using a flexible dosing strategy based on the degree of LDL-C lowering. As long as patients remain on therapy, there continues to be good control of LDL-C,” reported Dr. Mahfouz El Shahawy, Cardiovascular Center of Sarasota, Florida. He based this statement on data from the ODYSSEY COMBO II trial, which he presented at this year’s NLA meeting. Other phase 3 studies with the PCSK9 inhibitor alirocumab, such as ODYSSEY LONG TERM, have produced comparable results.
“As long as patients remain on therapy [alirocumab], there continues to be good control of LDL-C.”
Patients were eligible for enrollment in ODYSSEY COMBO II if they had hypercholesterolemia uncontrolled on maximally-tolerated statins and established coronary heart disease (CHD) or a CHD risk equivalent. These risk equivalents included moderate chronic kidney disease, diabetes mellitus plus at least 2 additional risk factors, peripheral artery disease (PAD) or a history of ischemic stroke.
Eligible patients were randomized in a 2:1 ratio to receive subcutaneous (SC) alirocumab plus an oral placebo or oral ezetimibe plus a placebo injection every 2 weeks. Patients in both arms of the trial were allowed to remain on the maximally-tolerated statins or other lipid-lowering agents they were taking at baseline. The initial dose of alirocumab was 75 mg but a dose increase to 150 mg was permitted at week 12. Only 18.4% of patients were moved to the higher dose.
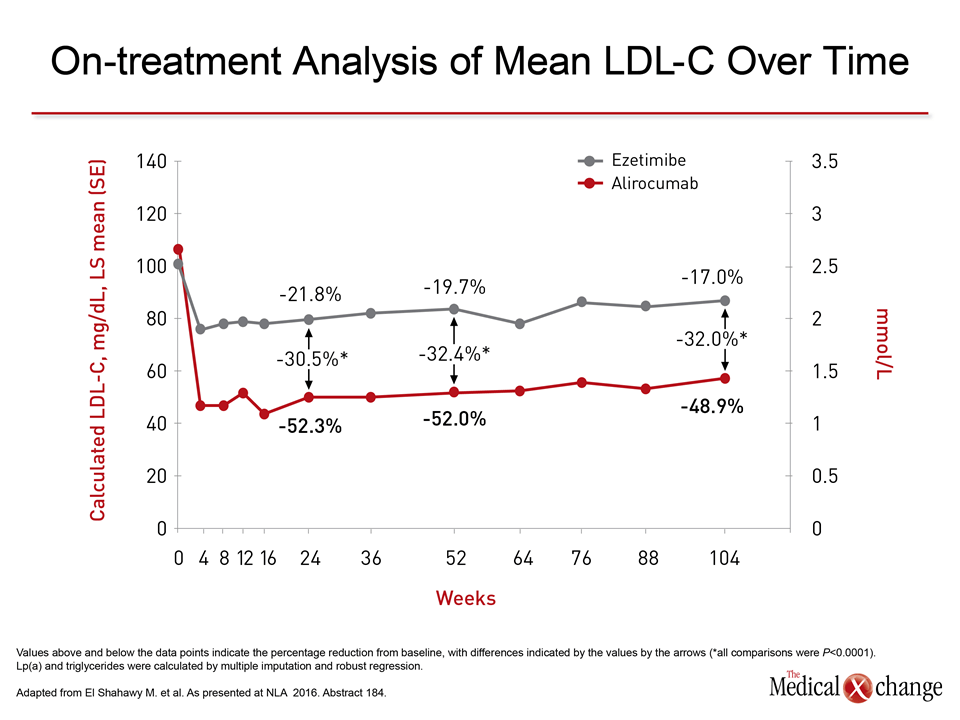
Representing the final analysis, the 104-week data of the ODYSSEY COMBO II presented here by Dr. El Shahawy demonstrate no clinically meaningful change over time in either the lipid-lowering efficacy of alirocumab or the safety profile. In on-treatment LDL-C reductions, the advantage of alirocumab over ezetimibe in these high-risk patients was essentially unchanged at 104 weeks (-32%) relative to 24 weeks (30.5%) or 1 year (32.4%) (Fig. 1).
The PCSK9 inhibitor alirocumab also provided about a 25% reduction relative to ezetimibe for Apo B, Lp(a), and non-high density lipoprotein cholesterol (HDL-C) at all time points. HDL-C was increased by alirocumab relative to ezetimibe by about 9% at all time points.
Safety Signals
Well tolerated at both 24 weeks and 1 year, alirocumab did not produce any new safety signals with extended follow-up. This included specific analysis of a broad array of adverse events of interest, such as ophthalmologic events, hepatic disorders, neurocognitive disorders, or allergic reactions. In a post-hoc analysis comparing rates of treatment-emergent adverse events reported through week 56 to those reported from week 56 through week 112, there were again no differences of note.
“Through week 56, alirocumab-treated patients had a slightly higher rate of local injection-site reactions relative to those randomized to ezetimibe [2.5% vs. 0.8%], but the incidence was slightly lower in the alirocumab group between weeks 56 and 112 [0.2% vs. 0.5%),” Dr. El Shahawy reported.
Getting High-risk Patients Closer to Treatment Goal
Perhaps the most important result of the trial was the greater relative ability of alirocumab than ezetimibe to get high-risk patients to treatment goal. On top of optimal statin therapy, 72.6% of those randomized to alirocumab versus 40.1% of those randomized to ezetimibe had LDL-C <1.8 mmol/L at week 104.
No equivalent data were presented at the 2016 NLA on evolocumab, another PCSK9 inhibitor that has provided high rates of LDL-C lowering relative to statins alone, but there were real-world data presented on the activity of both alirocumab and evolocumab outside of a clinical trial. In this prospective, observational experience at a pharmacist-managed lipid clinic, 49 patients with diabetes mellitus uncontrolled on statins alone were initiated on 75 mg of alirocumab or 140 mg of evolocumab administered every 2 weeks.
In a real-world observational experience PCSK9 inhibitor therapy was “associated with significant, intensive, and predictable reductions in atherogenic cholesterol.
Consistent with ODYSSEY COMBO II and other PCSK9 trials, these therapies were “associated with significant, intensive, and predictable reductions in atherogenic cholesterol,” reported Dr. Matthew D. Stryker, Albany College of Pharmacy and Health Sciences, Albany, New York.
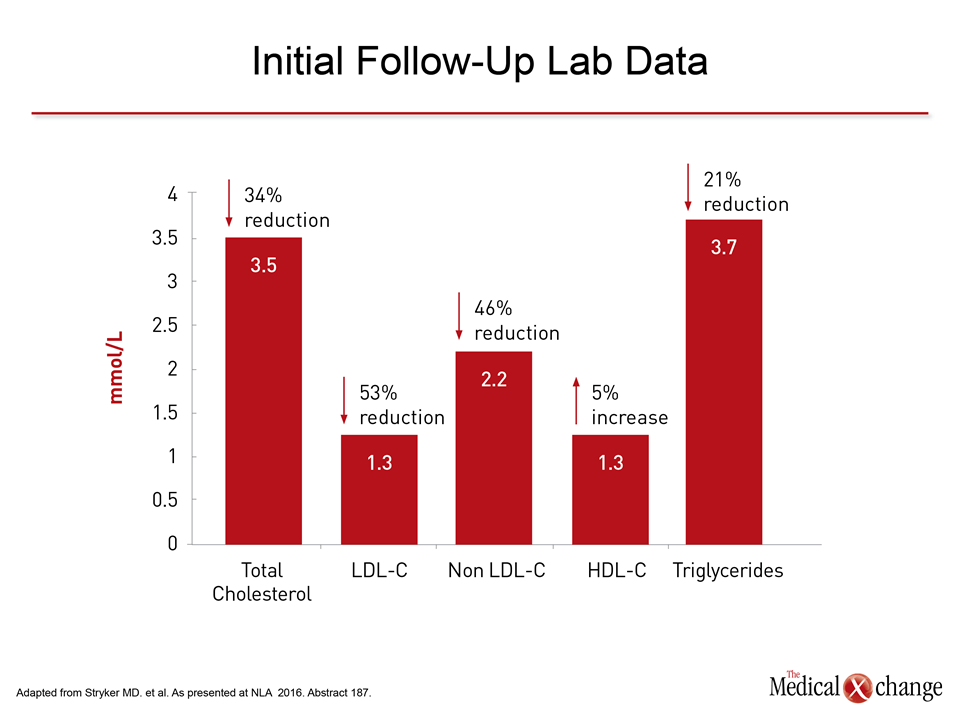
Specifically, the reduction in LDL-C was about 55% from baseline with alirocumab and evolocumab with no significant differences observed between them. This allowed a substantial proportion to reach guideline goals, but Dr. Stryker also emphasized the reductions in other lipid parameters particularly relevant to patients with diabetes (Fig. 2).
“Importantly, the use of this class of medications demonstrated a significant reduction in both LDL-C and non-HDL-C [53% and 46%, respectively, both P<0.001 relative to baseline], each of which is considered to be atherogenic and primary targets for anti-lipid therapy in high risk patients,” Dr. Stryker reported.
Although 13 patients attributed one or more side effects to their medication, only five discontinued therapy. There was no consistency in these adverse events, which included one case each of muscle aches and abdominal pain. Neither has been commonly observed in the large clinical trials with PCSK9 inhibitors.
Conclusion
The unprecedented LDL-C lowering achieved with PCSK9 inhibitors is well established, but such data as those from ODYSSEY COMBO II provide compelling evidence that the efficacy is provided indefinitely with a safety and tolerability profile that is typically unchanged over time.