HIV
21st International AIDS Conference (AIDS 2016)
High Rates of Adherence: New Opportunities for Indefinite HIV Control
Durban – Simplified HIV therapy built on integrase inhibitors was a dominant theme among clinical advances presented at AIDS 2016. Two sets of data stood out. In one, a phase 3 trial demonstrated that a once-daily, 1200-mg dose of raltegravir provides the same 48-week viral suppression as a twice-daily, 400-mg dose. In the other, a phase 2b trial provided initial support for sustained efficacy from an injectable regimen when combined with an experimental integrase inhibitor.
The phase 3 study, called the ONCEMRK trial, brings forward a new formulation of raltegravir, which has long been the anchor of triple-drug regimens. In the multinational, randomized trial, the once-daily 1200-mg dose and the twice-daily 400-mg dose were administered with the NRTIs tenofovir and emtricitabine (TDF/FTC).
Once-Daily Dose Matches Twice-Daily
“The ONCEMRK trial was a non-inferiority head-to-head comparison,” reported the lead investigator, Dr. Pedro Cahn, Chief of the Infectious Disease Unit, Juan A. Fernandez Hospital, Buenos Aires, Argentina. A past president of the International AIDS Society (IAS), Dr. Cahn said, “the 1200-mg, once-daily dose demonstrated potent and non-inferior efficacy compared to the twice daily dose.” He also reported no significant differences in safety.
“The 1200-mg, once-daily dose [of raltegravir] demonstrated potent and non-inferior efficacy compared to the twice daily dose.”
In this double-blind trial, 797 treatment-naïve HIV patients were randomized to the once-daily or twice-daily formulations of raltegravir, each administered along with TDF/FTC. The mean CD4 count at entry was 415 cells/mm3 and the mean viral load was vRNA 4.6 log10 copies. Patients with hepatitis B or C co-infection were admitted. The mean age was 35 years. The primary endpoint was vRNA <40 copies/mL at week 48.
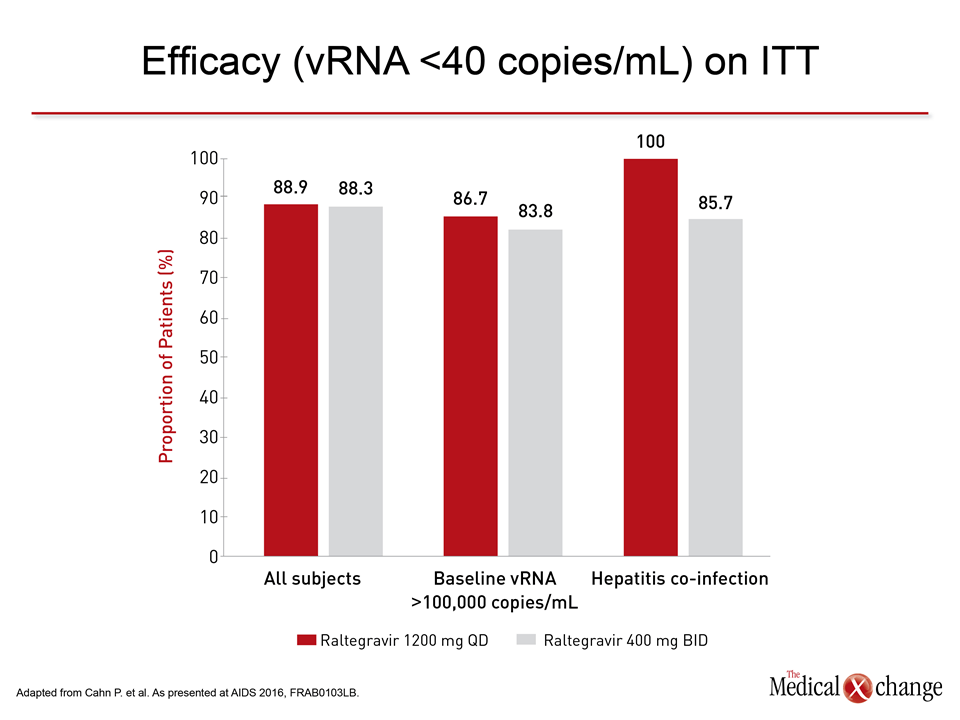
Viral load declined rapidly in both groups with >50% of patients achieving complete viral suppression, defined as vRNA <40 copies, by week 4. By week 48, this level of viral suppression was achieved in 88.9% and 88.3% in those randomized to the once-daily, 1200-mg and twice-daily 400 mg doses of raltegravir, respectively.
Viral Suppression Consistent in Subgroups
“When an analysis was performed to compare relative efficacy for the two regimens according to baseline viral load, presence of hepatitis co-infection, or other predefined characteristics, the rates of viral suppression remained comparable,” Dr. Cahn reported (Fig. 1). He also noted that the rate and degree of immunologic recovery as measured by CD4 counts was similar in the two groups.
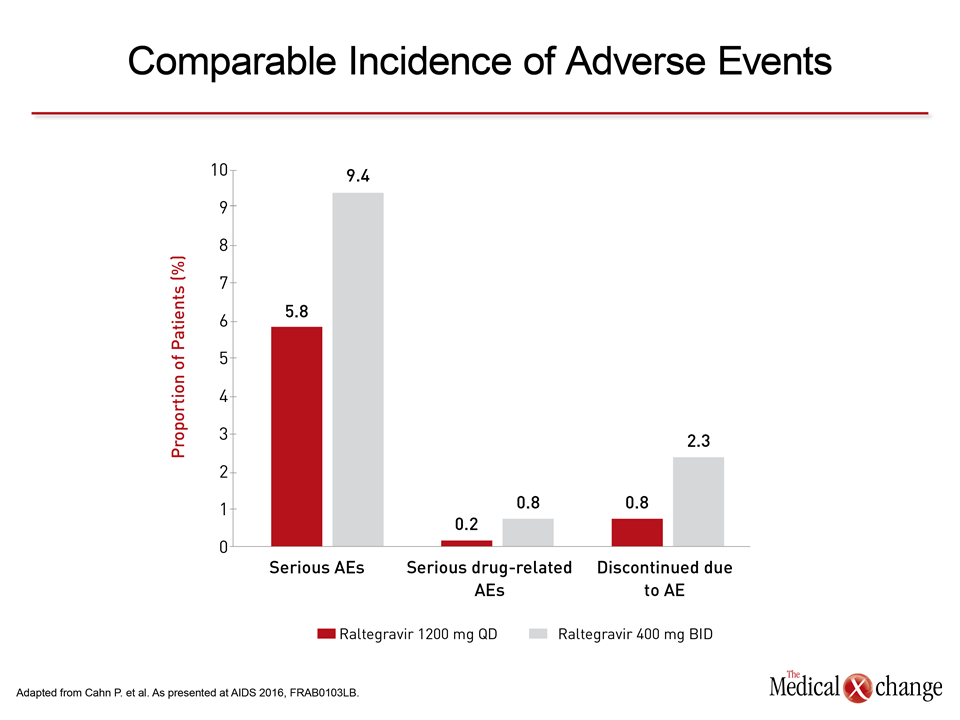
Both doses of raltegravir were well tolerated with no significant differences observed in the types or rates of adverse events (AEs) over the course of the study. Serious AEs of any kind were observed in 5.8% of those randomized to the once-daily and 9.4% of those randomized to the twice-daily doses, but drug-related serious AEs, such as allergic reactions, were less common, and discontinuation due to an AE occurred in 0.8% of the once-daily group and 2.3% of the twice-daily group (Fig. 2).
There is a large body of literature that has associated once-daily regimens in the treatment of HIV with improved adherence, including a meta-analysis that collated data from 19 studies (Nachega JB et al. Clin Infect Dis 2014;58:1297-1307). Given the evidence from this phase 3 trial that the efficacy and safety of the once-daily, 1200-mg dose of raltegravir is at least comparable to that of the proven and widely used twice-daily formulation, regulatory approval is considered imminent.
Injectable Integrase Inhibitor Pursued
It is too early to judge the potential clinical role of an injectable integrase inhibitor, but the 48-week results of a phase 2b study with cabotegravir, an experimental drug in this class, was promising. In this open-label, multicenter trial called LATTE-2, 286 treatment-naïve patients were randomized in a 2:2:1 ratio to one of three arms. These were, respectively, an every-four week (Q4) intramuscular (IM) injection of cabotegravir plus a long-acting formulation of the NNRTI rilpivirine (CAB/RIL), an every eight-week injection of CAB/RIL, or an oral regimen of CAB plus abacavir and lamivudine (ABC/3TC).
At 48 weeks, the primary endpoint of vRNA <50 copies was achieved by 91% of the Q4 CAB/RIL group, 92% of the Q8 CAB/RIL group, and 89% of the CAB/ABC/3TC group. Grade 1 or 2 injection site pain was reported by almost all patients in both groups receiving IM injections, but the pain was generally mild and resolved within a week. There were no serious drug-related AEs in any group. It is notable that patients generally expressed greater satisfaction with IM over oral therapy.
“Monthly dosing [of intramuscular cabotegravir] resulted in a modestly lower rate of virologic non-response or failure.”
“Monthly dosing resulted in a modestly lower rate of virologic non-response or failure,” reported the lead investigator Dr. David Margolis, Director of Clinical Development at ViiV Healthcare, Durham, North Carolina. As opposed to less than 1% in the Q4 CAB/RIL arm, virologic non-response and failure occurred in 7% of the Q8 CAB/RIL arm. Dr. Margolis reported that future development of the injectable CAB/RIL combination is to be pursued with the Q4 formulation.
Conclusion
Integrase inhibitors are widely preferred over protease inhibitors (PIs) and NNRTIs as anchor therapies in triple-drug HIV combinations because of their efficacy, high barrier to resistance, and tolerability. New data with once-daily raltegravir and an injectable experimental agent document efforts to make these regimens even simpler for indefinite and perhaps lifetime HIV control.