cardiology
European Society of Cardiology (ESC) Congress 2016
PCSK9 Inhibitors Required to Reach LDL-C Goals in Many High-risk Patients
Rome – To reach new low-density lipoprotein cholesterol (LDL-C) targets of <1.8 mmol/L or a >50% reduction from baseline in high-risk patients, PCSK9 inhibition may frequently be the only option, according to data presented at the ESC 2016 meeting. It is now clear that many of those at highest risk of a cardiovascular (CV) event, such as those with established CV disease or familial hypercholesterolemia (FH), are not optimally protected even when maximum doses of statins, ezetimibe, and other oral therapies are acceptably tolerated.
PCSK9 Inhibition Often Required for Goals
“We are moving toward personalized risk assessment to better guide patients about their likelihood of an event and the options for prevention,” observed Dr. Jennifer Robinson, Professor of Epidemiology, University of Iowa, Iowa City. According to Dr. Robinson, many third-party payers in the United States require a trial of high-intensity statins plus ezetimibe before reimbursing a PCSK9 inhibitor, but a substantial proportion of these high-risk patients qualify and will need a PCSK9 inhibitor to lower CV risk.
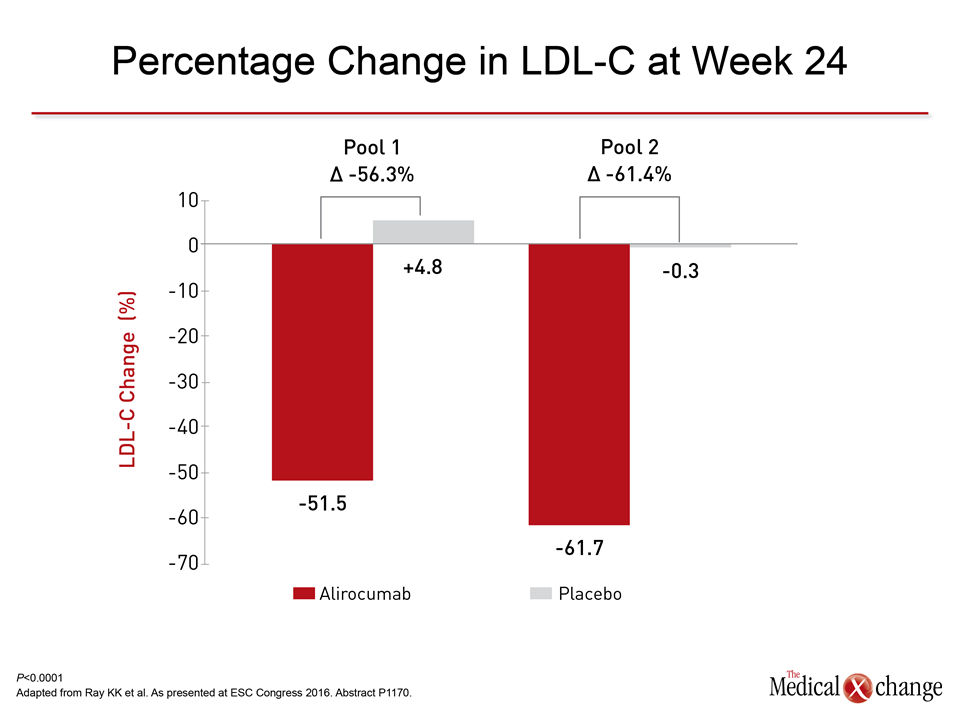
The evidence that PCSK9 inhibition is effective for reaching goals in high-risk patients is overwhelming. In one set of high-risk patients participating in the ODYSSEY alirocumab trials program, the average reduction in LDL-C for the 150 mg dose administered every 2 weeks was 61.7% at 24 weeks. For the 75 mg dose on the same schedule, the average reduction was 51.5% (Fig. 1), according to Dr. Kausik K. Ray, Professor of Public Health, Imperial College, London.
Patients were entered into this analysis if they had a history of multiple CV events in a single vascular bed or who had established CV disease in more than one vascular bed. The reductions (both P<0.0001 versus placebo) were achieved on a background of maximally-tolerated statins with or without ezetimibe or other oral lipid-lowering therapy. These are patients with substantial residual risk of a CV event even when treated to LDL-C goals of <1.8 mmol/L.
LDL-C Guideline Goals Evolving
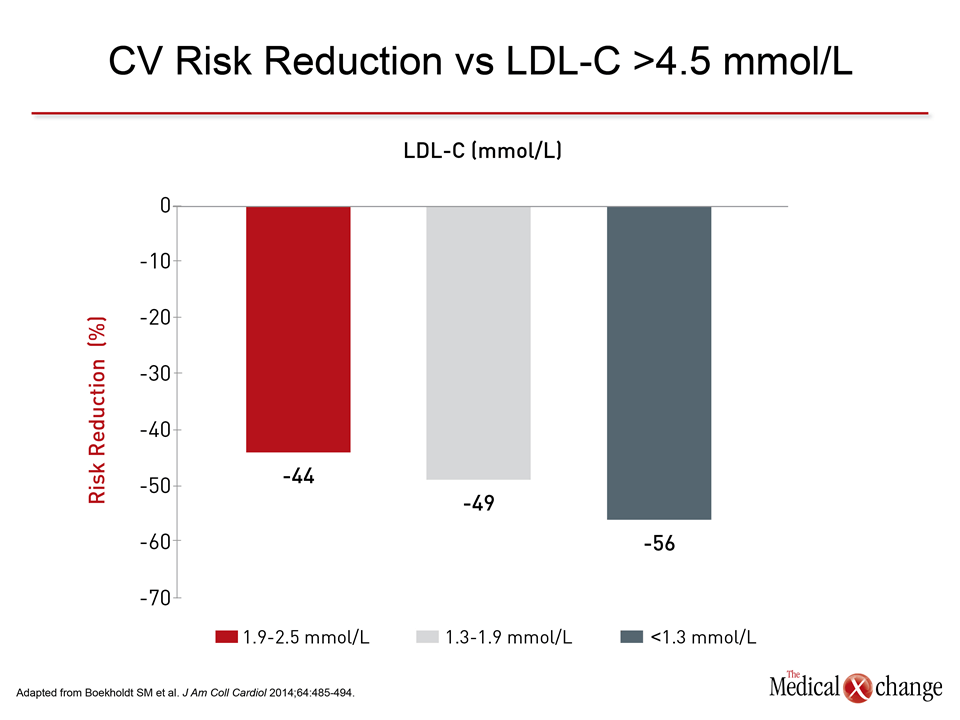
“In very high-risk patients, very low LDL-C levels—much lower than now reflected in many guidelines—are associated with even greater protection.”
“In very high-risk patients, very low LDL-C levels—much lower than now reflected in many guidelines—are associated with even greater protection,” said Dr. Ray, citing a series of studies that have found relative risk reductions at LDL-C levels extending to 1.0 mmol/L. In one study, which found that 40% of patients on high-dose statins do not reach LDL-C <1.8 mmol/L, the reduction in the risk of a CV event climbed from 49% in those who reached LDL-C of <1.95 mmol/L to 66% among those achieving LDL-C <1.25 mmol/L (Boekholdt SM et al. J Am Coll Cardiol 2014;64:485-494).
Such findings are being reflected in revised guidelines, including those soon to be published in Canada (Anderson TJ et al. Can J Cardiol 2016, in press). The new Canadian guidelines specify more aggressive LDL-C lowering in those at highest risk, such as those with established coronary disease. The targets are being defined as 50% reduction from baseline in LDL-C.
There is a strong potential that even lower LDL-C levels will confer greater incremental protection against CV events. In the Cholesterol Treatment Trialists’ (CTT) Collaborators meta-analysis, each 1.0 mmol/L decline in LDL-C was associated with a 21% reduction in CV risk without any LDL-C level at which there was no further benefit (CTT Collaborators. Lancet 2012;380:581-590). However, a substantial proportion of high-risk patients will require a PCSK9 inhibitor even at a target of <1.8 mmol/L, according to an analysis of 83,440 patients with atherosclerotic cardiovascular disease (ASCVD) entered into a US research database.
Goals on Oral Therapy Often Missed
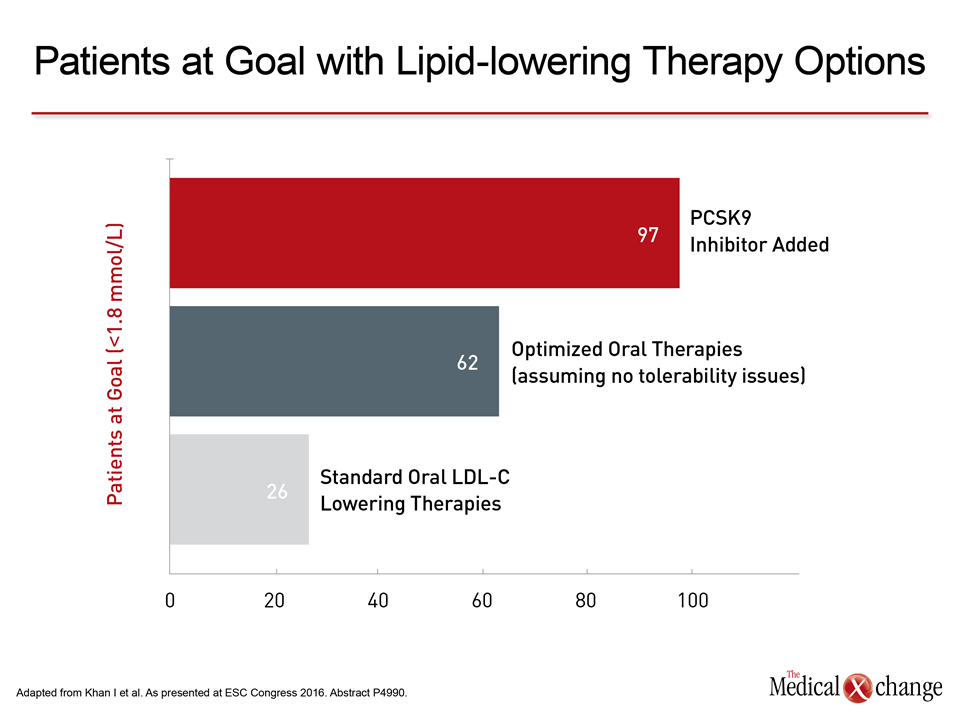
“Assuming no tolerability issues, opportunities exist for only about 62% of patients to achieve the LDL-C goal of <1.8 mmol/L through intensification of oral therapy.”
“Assuming no tolerability issues, opportunities exist for only about 62% of patients to achieve the LDL-C goal of <1.8 mmol/L through intensification of oral therapy,” reported a team of investigators that included Dr. Christopher P. Cannon, Senior Physician, Brigham and Women’s Hospital, Boston, MA. With the addition of a PCSK9 inhibitor, 97% of patients were projected to reach LDL-C <1.8 mmol/L.
In the ODYSSEY trials with alirocumab and the OSLER trials with evolocumab, which is the other currently approved PCSK9 inhibitor, the average on-treatment LDL-C levels typically achieved with agents in this class are <1.25 mmol/L. Such levels are safe, according to data pooled from 14 studies in the ODYSSEY trials program. Focusing on those with the lowest LDL-C levels, the senior author, Dr. Robinson, reported no significant difference in any treatment-emergent side effects when those with a LDL-C level of <0.39 mmol/L were compared to those with higher LDL-C levels. Data included patients on alirocumab for up to 104 weeks.
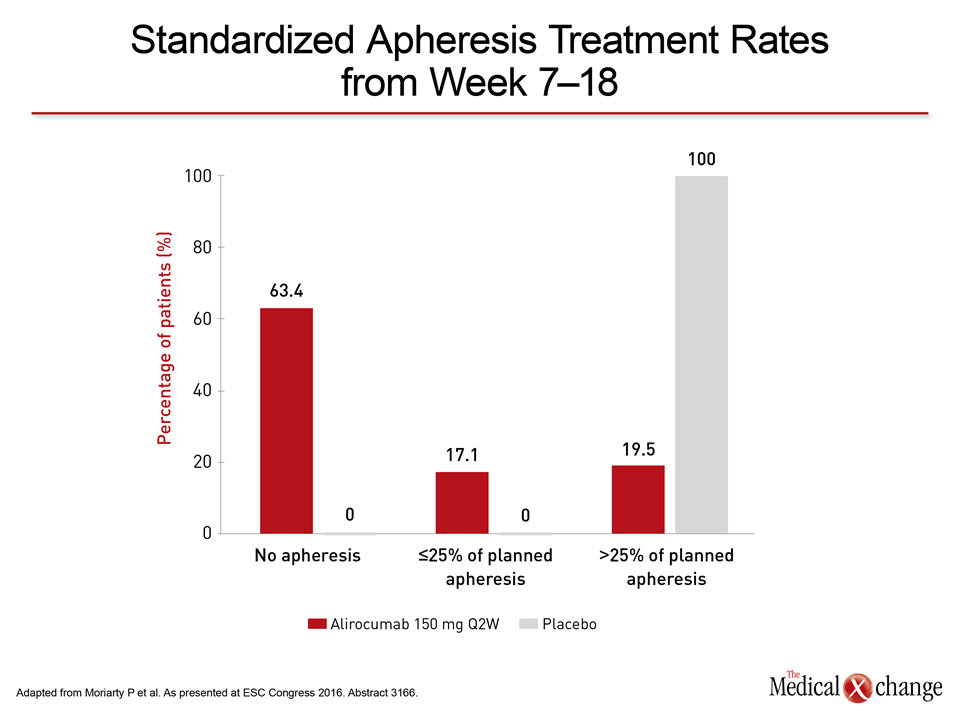
The potency of the PCSK9 inhibitors is particularly well illustrated in FH patients. In a new FH study from the ODYSSEY trials program, called ESCAPE, 92% of patients with heterozygous FH (HeFH) reduced apheresis treatments based on LDL-C reductions (versus 14.3% in the placebo arm), and 63.4% eliminated apheresis altogether, according to Dr. Patrick M. Moriarty, Director of Clinical Pharmacology, University of Kansas, Kansas City (Fig. 2). For HeFH, Dr. Moriarty called the treatment effect of alirocumab in the ESCAPE trial “a major breakthrough.”
Conclusion
Overall, the data presented at ESC 2016 indicate that PCSK9 inhibition for many high-risk patients is essential to meet rigorous LDL-C targets. Ongoing studies with these agents are expected to play a major role in redefining the parameters of CV risk reduction.