Respirology
European Respiratory Society (ERS) International Congress 2016
New Data Emphasize the Therapeutic Value of Biologics in Control of Severe Eosinophilic Asthma
London – Data presented at the 2016 ERS Congress reinforce the premise that biologics have a central role in the control of the severe eosinophilic asthma phenotype. These studies include phase 3 data with a new monoclonal antibody (MAb) targeting the interleukin-5 (IL-5) receptor, new analyses of an already approved IL-5 inhibitor in a refractory population, and a paediatric study of the first approved biologic for asthma, which is targeted at immunoglobulin E (IgE). All of these agents have been associated with significant reductions in rate of exacerbations relative to placebo. Biologics targeting other mediators and pathways of eosinophil activation are expected, although a newly completed phase 3 study with a MAb targeting interleukin-13 (IL-13) was negative.
Severe Eosinophilic Asthma Phenotype
The challenge of severe eosinophilic asthma is illustrated by the IDEAL study, which gathered data on resource utilization. In this study, the mean incidence of severe exacerbations per year (3.2 vs. 1.2) and the proportion requiring one or more hospitalizations (23% vs. 9%) were more than two times greater in the 137 patients with severe eosinophilic asthma compared to 533 patients with other severe phenotypes. In all cases, severity was defined as disease requiring high doses of inhaled corticosteroid with a second controller and/or systemic corticosteroid. “Of patients with eosinophilic asthma, there is a subset that is not being controlled on the standard therapies, and these are the ones consuming a disproportional share of healthcare resources,” reported the multicenter team of authors from the IDEAL study (Müllerová H et al. ERS 2016, PA4217).
Data Presented at the ERS Congress
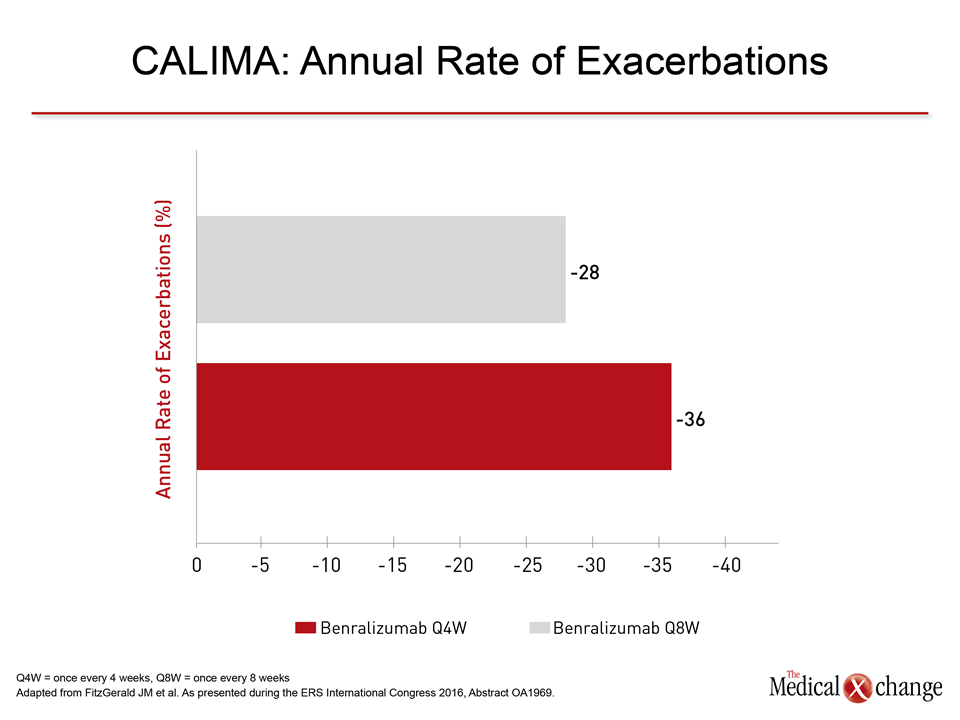
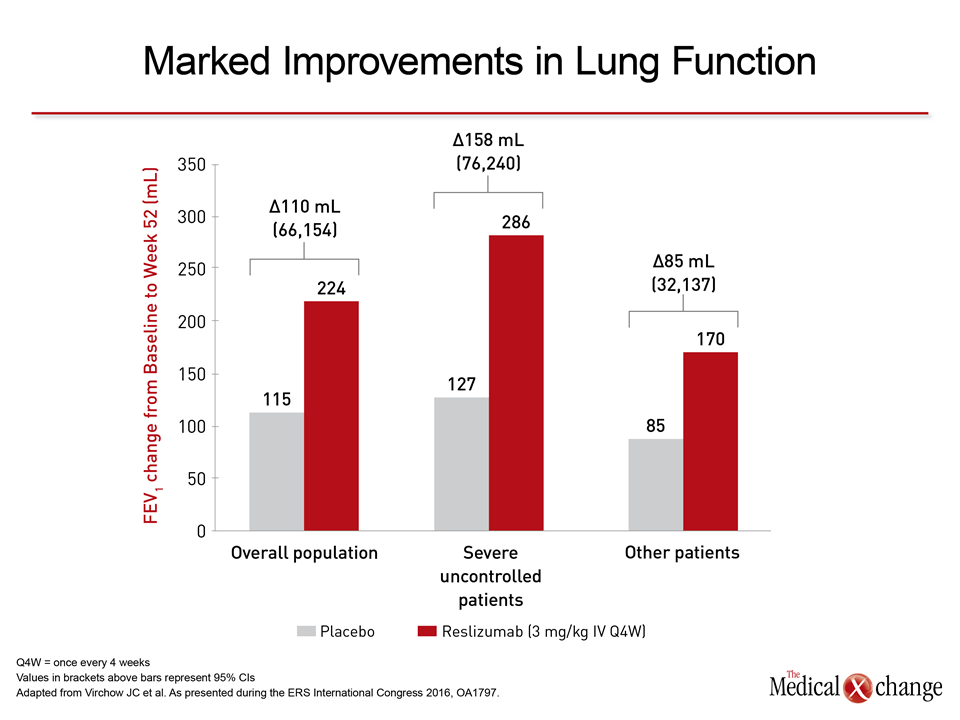
The interest in biologics is driven by the inadequacy of standard therapies for severe eosinophilic asthma. At the ERS meeting, two phase 3 trials with benralizumab, the MAb targeting IL-5 receptor, were presented. If approved, as anticipated by the phase 3 data, it will join mepolizumab and reslizumab, the two currently approved IL-5 inhibitors, as well as a third biologic, the IgE-targeted omalizumab. In the two similarly designed phase 3 trials with benralizumab, called SIRROCO and CALIMA, patients with severe, uncontrolled asthma (≥2 exacerbations in the prior year while on high-dose corticosteroids) were randomized to one of two schedules (30 mg every 4 or 8 weeks) or placebo. There were 1,205 patients randomized in SIROCCO (Bleecker, EJ et al. ERS 2016, Abstract OA4832) and 1,306 patients randomized in CALIMA (FitzGerald JM et al. ERS 2016, Abstract OA1969). The primary endpoint was reduction in the rate of exacerbations. In CALIMA, the IL-5 receptor inhibitor benralizumab was associated with a 36% reduction in the rate of exacerbations relative to placebo (P=0.0018) on the every 4-week schedule and 28% reduction (P=0.0188) on the every 8-week schedule (Fig. 1). In SIROCCO, these relative reductions were 45% (P<0.0001) and 51% (P<0.0001) for the same two arms, respectively. Positive results with several key secondary outcomes reinforced the main result. For example, benralizumab provided a significant improvement in lung function as measured by FEV1 in both studies. Improvements in symptoms on benralizumab, as measured with the Asthma Control Questionnaire (ACQ-6) were significant relative to placebo in the CALIMA trial among patients with elevated eosinophils at baseline. This was true also in the SIROCCO trial but only for those randomized to the every-4-week, not the every-8-week, schedule. On the Asthma Quality of life (AQLQ) instrument, the advantage for benralizumab relative to placebo reached significance only for those with elevated eosinophils receiving the every-8-week schedule in both trials. As observed in previous studies with MAbs targeting IL-5, benralizumab was well tolerated. In both studies, the rates of serious adverse events were actually lower for both benralizumab arms relative to placebo. No new data were presented at the 2016 ERS on mepolizumab, but post-hoc analyses were presented for the other approved IL-5 inhibitor, reslizumab, and the anti-IgE agent omalizumab. The new data on reslizumab were drawn from 306 patients participating in the phase 3 trials who met the joint American Thoracic Society/ERS definition of refractory asthma, which requires persistent symptoms despite continuous or near continuous oral corticosteroids (Virchow, JC et al. ERS 2016, OA1797). When the change in rate of exacerbations in this refractory population was compared to that observed overall in the phase 3 program, the magnitude of the advantage for reslizumab over placebo was greater, according to Dr. J. Christian Virchow, Head, Department of Pulmonology, University of Rostock, Germany (Fig. 2). The relative improvements for reslizumab to placebo in lung function, as measured by change in FEV1 from baseline to week 52, quality of life, as measured with the Asthma Quality of Life Questionnaire (AQLQ), and asthma symptom control, as measured with the Asthma Symptom Utility Index (ASUI), were also greater in the refractory subgroup of patients relative to the overall population. Omalizumab was the first biologic made available for control of asthma. Although not necessarily reserved for the eosinophilic phenotype, this treatment also lowers eosinophil levels (Walford HH, Doherty TA. J Asthma Allergy 2014;7:53-65). New data at the ERS confirmed efficacy in children (Abusamra R et al. ERS 2016, PA1238). In this study, conducted in patients aged 6 to 18 years, the mean number of exacerbations over the year of treatment fell to 1.6 from the 6.7 (P<0.0001) recorded in the year prior to the study. According to the lead author, Dr. Rania Abusamra, Kings College Hospital, London, UK, the favourable toxicity profile encourages studies in even younger patients with therapy-resistant disease. IL-13, which is implicated in several pathogenic processes that drive asthma, is an attractive target for the development of new biologics (Corren J. Curr Allergy Asthma Rep 2013;13:415-20), but two-phase 3 trials presented at the ERS meeting with the IL-13 inhibitor lebrikizumab proved disappointing (Hanania N et al. ERS 2016, Abstract OA1975). In the similarly designed phase 3 trials, LAVOLTA I and II, the results were discordant, according to the principal investigator Dr. Nicola A. Hanania, Baylor College of Medicine, Houston. In LAVOLTA I, both of the lebrikizumab doses (37.5 mg and 125 mg) significantly reduced the exacerbation rate relative to placebo in defined as biomarker-high patients, which included a blood eosinophil count ≥300 μg/L, but only the lower dose showed significant benefit in the biomarker-low group. In LAVOLTA II, neither dose showed efficacy.
Conclusion
In severe asthma patients with the eosinophilic phenotype who are uncontrolled with standard asthma therapies, biologics are assuming a central role in treatment. Data from ERS 2016 provide an update about the efficacy and clinical role of these agents.