cardiology
American Heart Association Scientific Sessions 2016
Upward PCSK9 Inhibitor Dose Titration Uncommonly Required to Reach Goal in Challenging Patients
New Orleans – When treated with a PCSK9 inhibitor, nearly 60% of patients with familial hypercholesterolemia (FH) achieve adequate and sustained control of low-density lipoprotein cholesterol (LDL-C) at the starting dose, according to an analysis of open-label study. The efficacy of the initial dose in this high-risk population, considered one of the most challenging, was drawn from a real-world extension study presented at the 2016 AHA Scientific Sessions. In the context of other PCSK9 data presented at the AHA regarding safety as well as the effects of these agents on lipids other than LDL-C, the FH study underscores that the role of PCSK9 inhibitors is controlling LDL-C in patients inadequately managed on statins alone.
Low Dose PCSK9 Inhibition Often Sufficient
Bringing patients with FH to LDL-C goals has provided PCSK9 inhibitors with a clear demonstration of unprecedented efficacy of LDL-C lowering. This is because statins, whether alone or in combination with other traditional lipid-lowering agents, bring only a minority of FH patients to LDL-C levels required for optimal cardiovascular (CV) risk reduction. A recent real-world study with the PSCK9 inhibitor alirocumab expands evidence that these agents are fulfilling an unmet need even at the initial dose.
“The bottom line from this open-label extension is that the starting dose works for most people outside of a protocol-driven trial.”
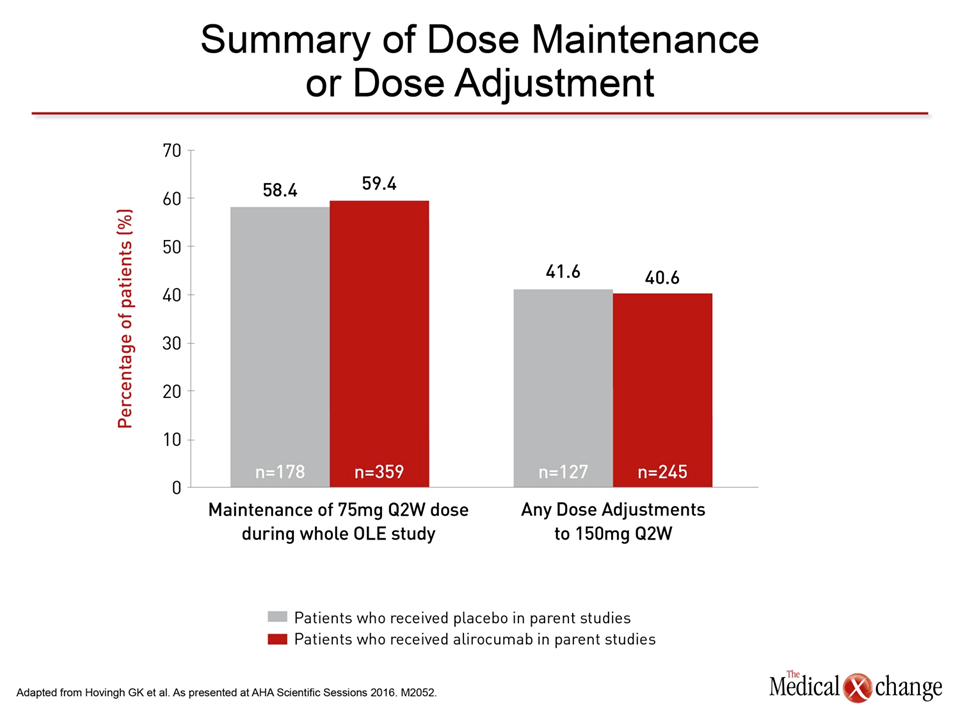
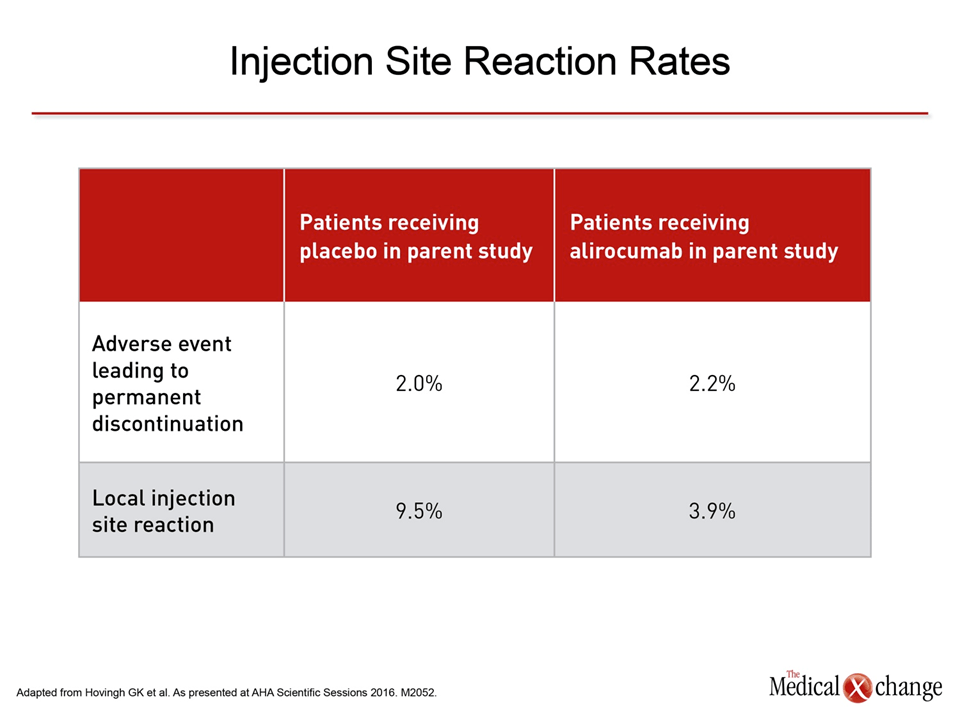
“The bottom line from this open-label extension is that the starting dose works for most people outside of a protocol-driven trial,” reported Dr. John Guyton, Duke University Medical Center, Durham, North Carolina. “This was a study conducted in patients who really needed a lot of cholesterol lowering,” he added. Yet, “59% who started on the 75 mg dose stayed on the 75 mg dose, and 64% who stayed on this lower dose achieved an LDL less than 70 mg/dl [<1.8 mmol/L].” In this open-label extension study, called ODYSSEY OLE (Hovingh GK et al. AHA 2016, M2502), the objective was to evaluate dosing strategies among clinicians who did not have to adhere to trial-driven protocols. The 909 heterozygous FH (HeFH) patients who participated were entered into this extension from centers in Canada, Europe and the United States. They had earlier participated in ODYSSEY FH I, ODYSSEY FH II, or ODYSSEY LONG-TERM (OLT), which were the phase 3 alirocumab trials that included FH patients. Baseline LDL-C levels varied, but the median LDL-C among patients on placebo in the randomized trials before enrolling in ODYSSEY OLE were near or above 4.0 mmol/L. Participants were started on 75 mg alirocumab administered every 2 weeks, irrespective of dose adjustment. On the basis of their clinical judgment, treating physicians could increase the alirocumab dose to 150 mg every 2 weeks. Whether patients had received placebo or alirocumab in the randomized trial prior to entering ODYSSEY OLE, the proportion that remained on the starting dose over the median 73 weeks of follow-up was similar (Fig. 1). Treatment discontinuations for an adverse event were uncommon. Of these adverse events, injection site reactions (ISR), reported by 5.4%, were by far the most frequently reported. However, Dr. Guyton pointed out that the ISR rates were substantially lower in OLE among those patients previously treated with alirocumab (Fig. 2).
“The rate of adverse events in the open label extension was very low.”
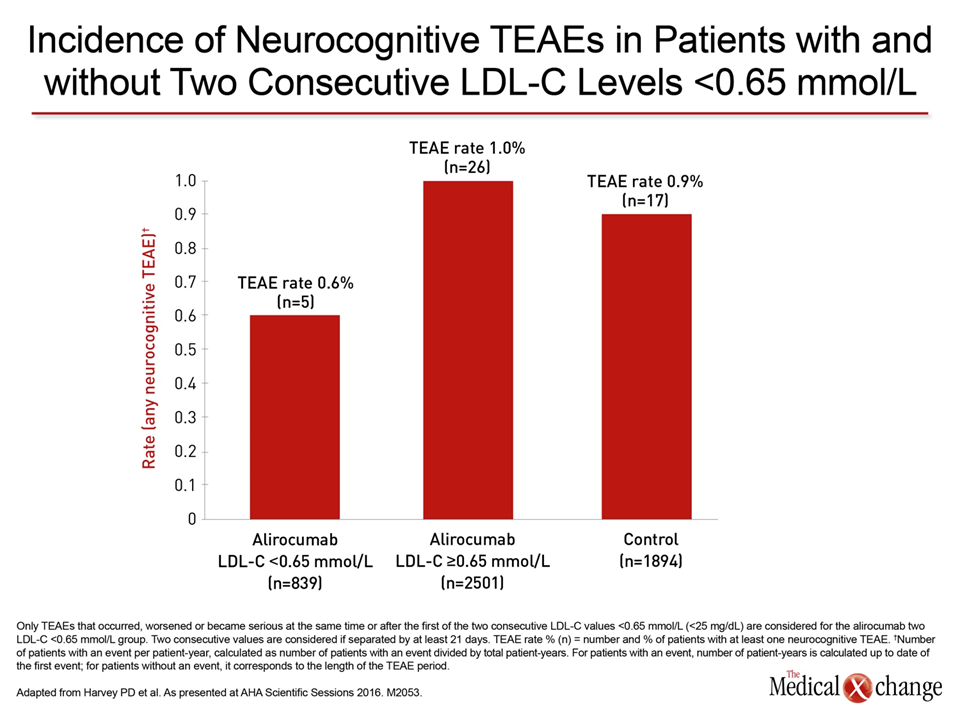
“The rate of adverse events in the open label extension was very low,” Dr. Guyton said. Although he acknowledged that there was no placebo group for comparison, the safety and tolerability is consistent with the phase 3 trials both in FH patients and in others who have participated in the phase 3 investigations with alirocumab or other PCSK9 inhibitors, such as evolocumab, which has also been granted regulatory approval. Several studies looking more deeply into adverse events in the large trial programs have yielded the same conclusion. In a separate study looking specifically at rates of neurocognitive adverse events in 4616 patients who participated in placebo-controlled trials with alirocumab, the rates were 0.9% and 0.7% for alirocumab and placebo, respectively (Harvey PD et al. AHA 2016, M2053). There was no trend for significance. In this analysis, which included 3340 patients randomized to alirocumab and 1276 randomized to placebo in phase II or III trials, patients were treated for up to 104 weeks. The rates of neurocognitive adverse events were compared between alirocumab and placebo groups as well as among patients who achieved a LDL-C <0.65 mmol/L. LDL-C levels this low were achieved in 839 alirocumab patients. There were no trends for significance between rates of neurocognitive events in any group evaluated although rates were numerically lower in patients who achieved very low levels of LDL-C, according to the principal investigator, Dr. Philip D. Harvey, University of Miami Miller School of Medicine, Florida (Fig. 3).
Diabetics and Non-Diabetics Respond Similarly
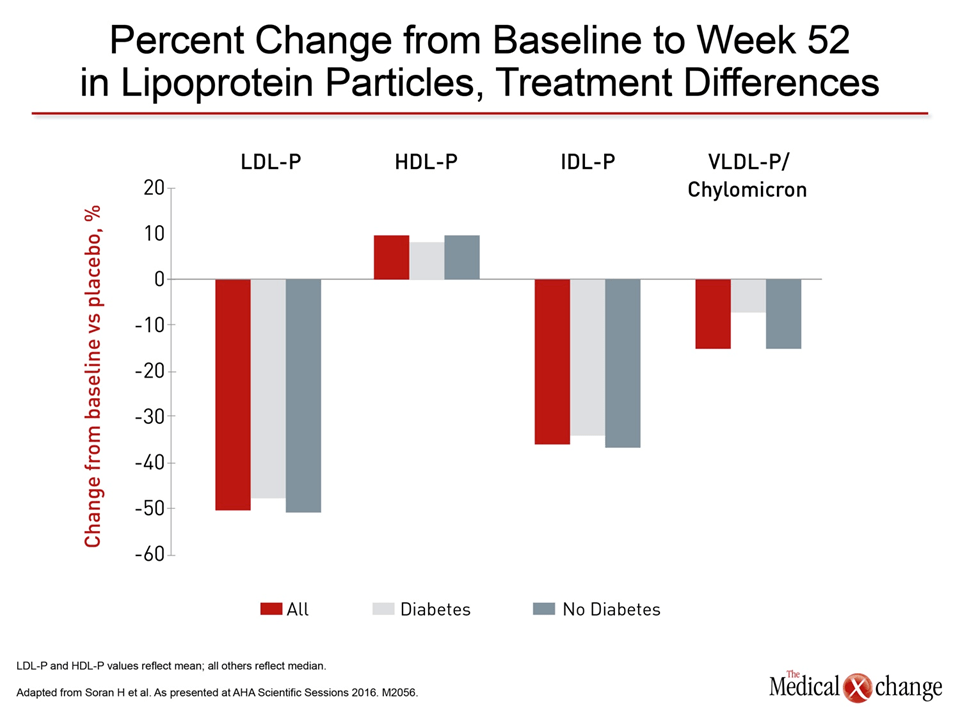
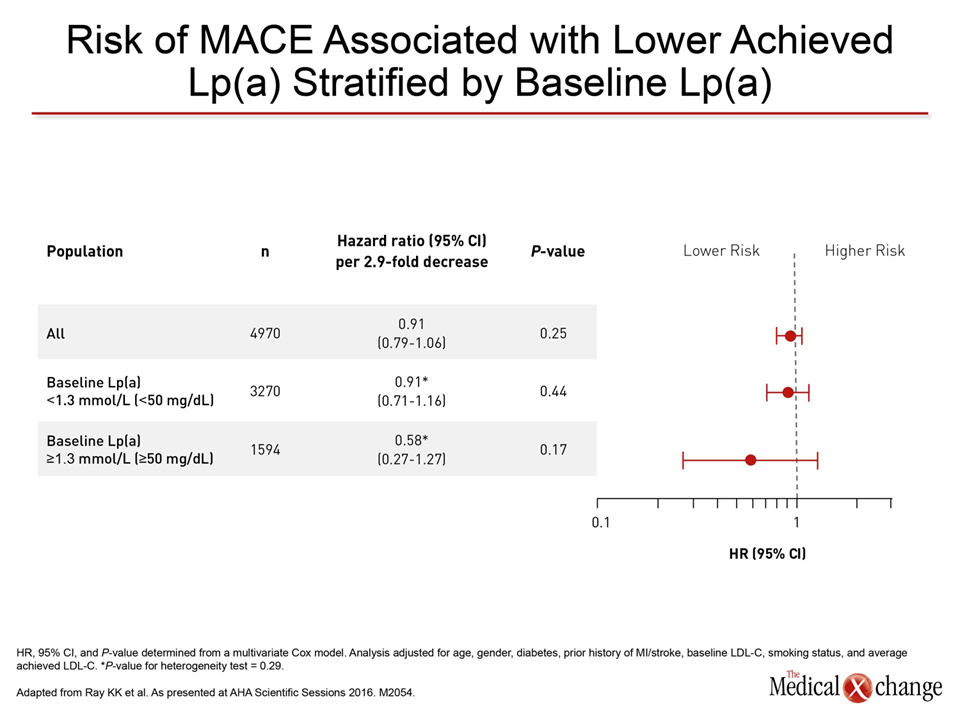
In new data on evolocumab at this year’s AHA meeting, the focus was not on safety but on the activity of this PCSK9 inhibitor on atherogenic lipoprotein particle concentrations in patients with diabetes compared to those without (Soran H et al. AHA 2016, M2506). Emerging data suggesting that the PCSK9 inhibitors favorably influence other cholesterol-related risk factors have prompted studies with both evolocumab and alirocumab. In the study of evolocumab, presented by Dr. Handrean Soran, Division of Cardiology, Central Manchester University Hospital, UK, there was no difference between patients with and without diabetes, but evolocumab was associated with significant improvements in the lipoprotein profile of both. “In this post-hoc analysis using nuclear magnetic resonance (NMR) spectroscopy, there were improvements in atherogenic lipoprotein particle concentrations that included reductions in chylomicrons, VLDL (very low density lipoproteins), LDL, and IDL (intermediate density lipoproteins), as well as an increase in HDL (high density lipoprotein) whether or not patients had diabetes,” Dr. Soran reported (Fig. 4). In a study evaluating the effects of alirocumab on Lp(a) among patients participating in controlled trials, the reductions were substantial, but further analysis suggested that when these reductions were evaluated in the context of major adverse CV events (MACE), they did not appear to have an effect independent of LDL-C (Ray KK et al. AHA 2016, M2054).
Lp(a) Reduction Has Modest Risk Effect
“As soon as you take LDL into account, the reduction in Lp(a) does not seem to matter.”
“If you look at Lp(a) reduction without taking into account LDL, there is a suggestion of benefit, but as soon as you take LDL into account, the reduction in Lp(a) does not seem to matter,” explained Dr. Kausik K. Ray, School of Public Health, Imperial College, London, UK. Data were gathered for this study from patients participating in 10 phase 3 ODYSSEY trials. There were 104 MACE events, defined as death from coronary heart disease (CHD), myocardial infarction (MI), ischemic stroke, or unstable angina requiring hospitalization over the course of follow-up. Independent of LDL-C lowering, alirocumab was associated with a median 25.6% reduction in Lp(a) from baseline. In an analysis unadjusted for on-treatment LDL-C, the reduction in Lp(a) was associated with a 11% reduction in the risk of MACE (HR 0.89, 95% CI, 0.77 – 1.03), but the 95% confidence intervals exceeded those required to demonstrate statistical significance, according to Dr. Ray. Overall, those with higher baseline Lp(a) levels (>1.3 mmol/L) had numerically lower hazard ratio than lower baseline Lp(a) after treatment with alirocumab (HR 0.58 vs. 0.91), but neither reduction achieved statistical significance (Fig. 5). “The limitations of this study include the fact that median Lp(a) levels were not particularly elevated among patients in this analysis, and there was a small number of MACE events,” Dr. Ray reported. While this was an “ad-hoc, hypothesis-generating” evaluation, “the ongoing ODYSSEY OUTCOMES study is specifically designed to evaluate the impact of lipid lowering with alirocumab on MACE and will evaluate these events in the context of reductions in Lp(a) as well as LDL-C.” The ODYSSEY OUTCOMES trial is scheduled for completion in 2017.
Summary
The experience with PCSK9 inhibitors outside of clinical trials has permitted confirmation that durable lipid lowering can be achieved with the starting dose in most FH patients, a challenging population. These data expand the evidence that PCSK9 inhibitors fulfill an unmet need for lipid control in patients unable to reach guideline goals on statins alone. With accumulating data, there is growing reassurance about the safety of PCSK9 inhibition overall as well as for the safety of achieving very low (<0.65 mmol/L) LDL-C levels. Although favorable effects on other lipid subfractions have been associated with PCSK9 inhibitors, data so far suggest that most benefit is derived from the profound LDL-C reductions provided by agents in this class.