hematology
58th American Society of Hematology (ASH) Annual Meeting and Exposition
Progress in Myelofibrosis: Early Use of Targeted Therapy May Extend Life Expectancy
San Diego – For myelofibrosis (MF), early treatment is likely to extend a previously-reported survival benefit with a targeted therapy, according to one of a series of studies at the 2016 ASH annual meeting that outlined progress in the management of this disease. These included two large and detailed analyses of the long-term safety and efficacy of a Janus kinase (JAK) inhibitor in the treatment of myelofibrosis, an early phase study of JAK inhibition prior to hematopoietic cell transplantation (HCT), and a study with an experimental multi-kinase inhibitor showing activity in MF patients with low baseline platelet counts.
JAK Signaling is Pivotal in MF
Evidence that activation of the JAK signaling pathway plays a central pathogenic role in MF culminated in pivotal COMFORT I and II phase 3 studies with a therapy targeted at this signaling pathway. In these studies, published nearly 5 years ago (Harrison C et al. N Engl J Med 2012; 366:787-798 and 799-807the JAK inhibitor ruxolitinib was associated with prolonged overall survival (OS) in addition to improvement in splenomegaly, MF symptoms, and quality of life. Two new studies from the same set of data presented at the 2016 ASH meeting suggest that earlier treatment may build on that OS benefit. In one, an exploratory analysis, outcomes in patients who initiated ruxolitinib prior to developing anemia were compared to those who had anemia at baseline (Gupta Vet al. ASH 2016, abstract 3118). Anemia was defined as any red blood cell transfusion within 12 weeks of study entry or hemoglobin (Hb) <10 g/dL. According to this analysis, there was a greater likelihood of transfusion independence at 24 weeks if treatment was started before anemia. In turn, transfusion independence at 24 weeks was associated with improved OS in follow-up out to 5 years. “Previously demonstrated poor outcomes with anemia combined with the transfusion and OS results in this study suggest that patients with MF may achieve better outcomes with earlier ruxolitinib treatment,” reported the lead author of this analysis, Dr. Vikas Gupta, Princess Margaret Cancer Centre, Toronto, Ontario. Specifically, there appears to be an advantage from initiating treatment before anemia occurs.
Limited Options Prior to Ruxolitinib
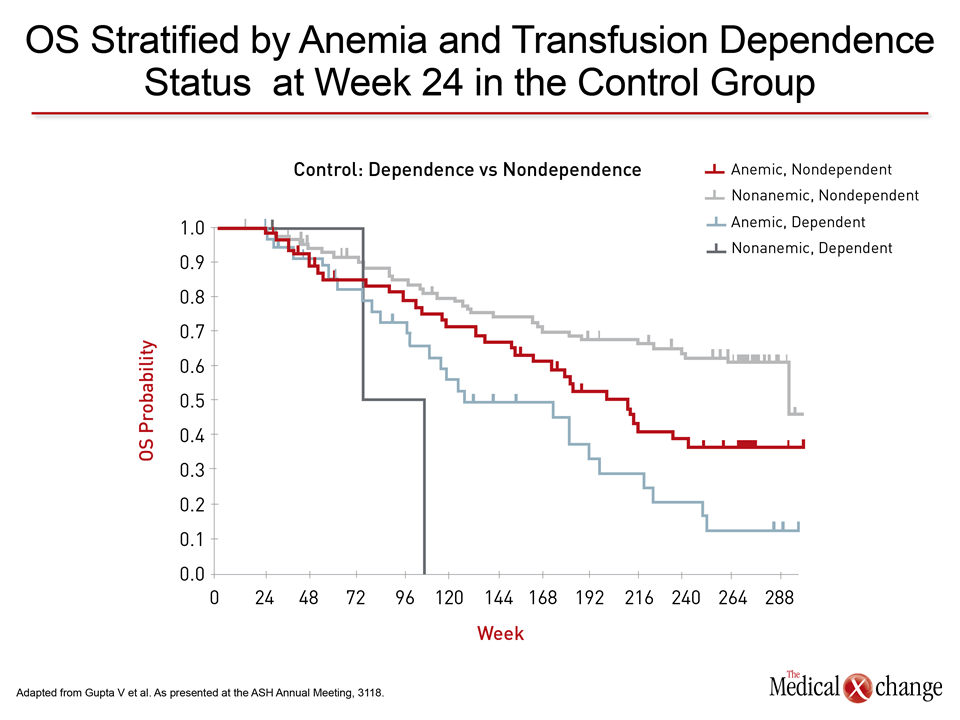
Prior to ruxolitinib, patients who were not candidates for a potentially curative HCT had few options for symptom control or for halting a progressive and ultimately terminal disease process. With advancing anemia, thrombocytopenia, and leukopenia, MF produces fatigue, weight loss, bone pain, cachexia, abdominal pain, and weakness. The COMFORT trials demonstrated that JAK inhibition can control symptoms and extend survival in intermediate- or high-risk MF relative to placebo or best available therapy (BAT), but the optimal time to initiate this therapy has been an area of active investigation. In data drawn from the exploratory analysis, patients who were nonanemic at baseline were more likely to remain transfusion-independent at week 24. Although nearly a fifth of patients who were anemic at baseline and treated with ruxolitinib were transfusion-independent at week 24, the more important finding was that ruxolitinib treatment prevented the adverse effect on transfusion dependence at week 24. “Transfusion requirement [at week 24] had little impact on clinical outcomes or treatment discontinuation within the ruxolitinib group but was associated with reduced OS and worsened MFSAF TSS [MF Symptom Assessment Form Total Symptom Scores] in the control group,” Dr. Gupta explained.
Overall Survival Improves with Anemia Control
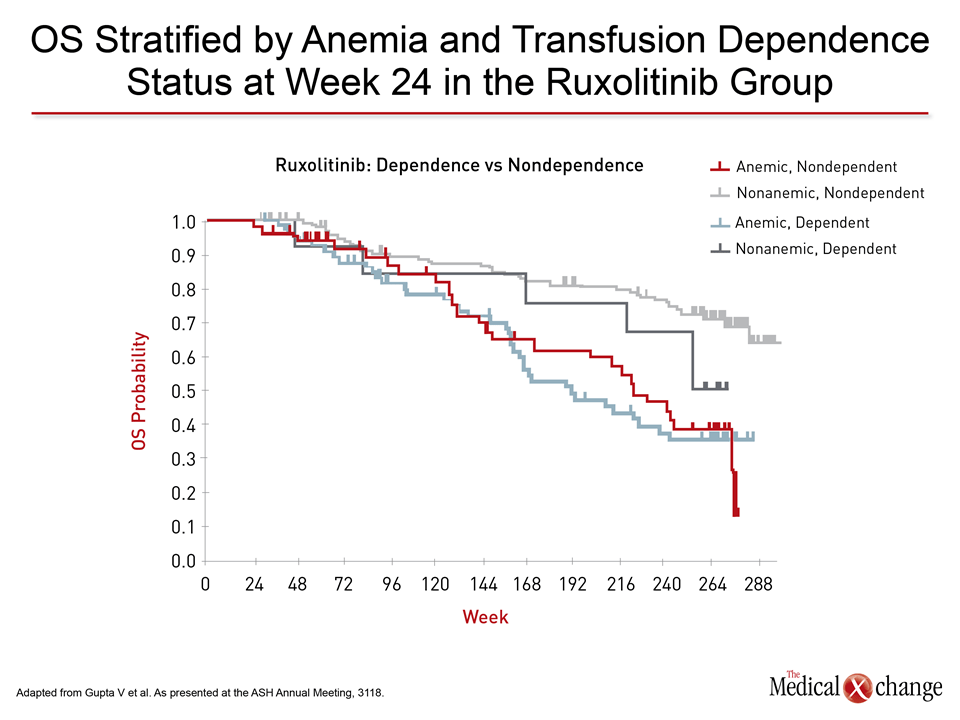
In addition, “median OS was significantly longer in the ruxolitinib group compared with the control group even for patients who were transfusion-dependent at week 24,” Dr. Gupta reported (Fig. 1A) (Fig. 1B). Overall, the median durations of OS in patients with anemia at baseline were 191 weeks versus 127 weeks for ruxolitinib and placebo, respectively. For non-anemic patients, median OS has not been reached in the ruxolitinib arms versus 90 weeks for baseline non-anemic patients (P=0.0014 overall favoring ruxolitinib).
“Median OS was significantly longer in the ruxolitinib group compared with the control group even for patients who were transfusion-dependent at week 24.”
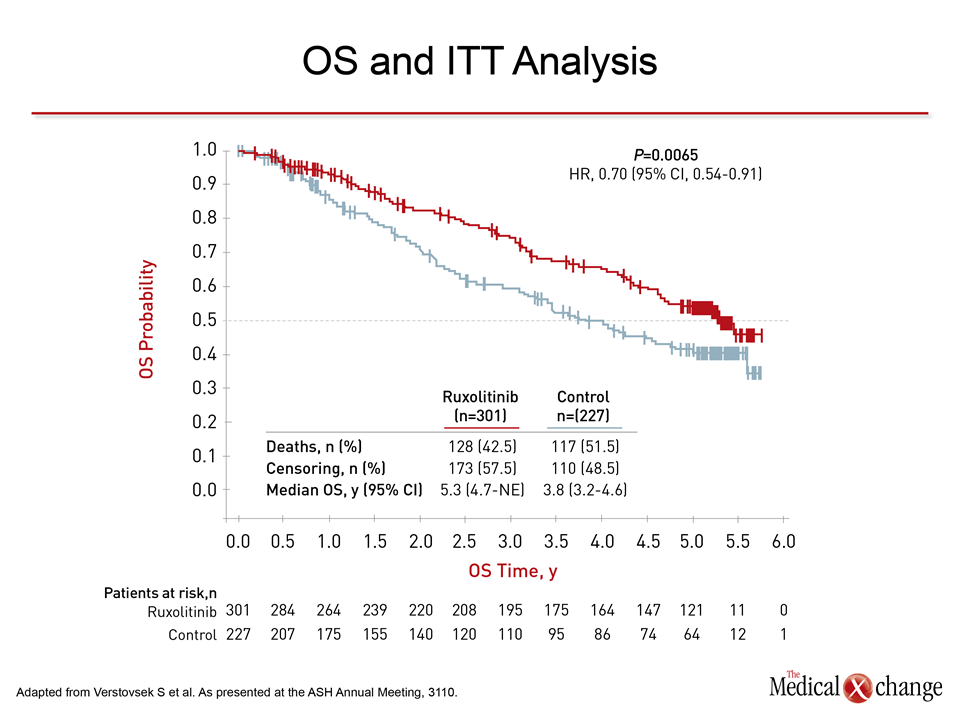
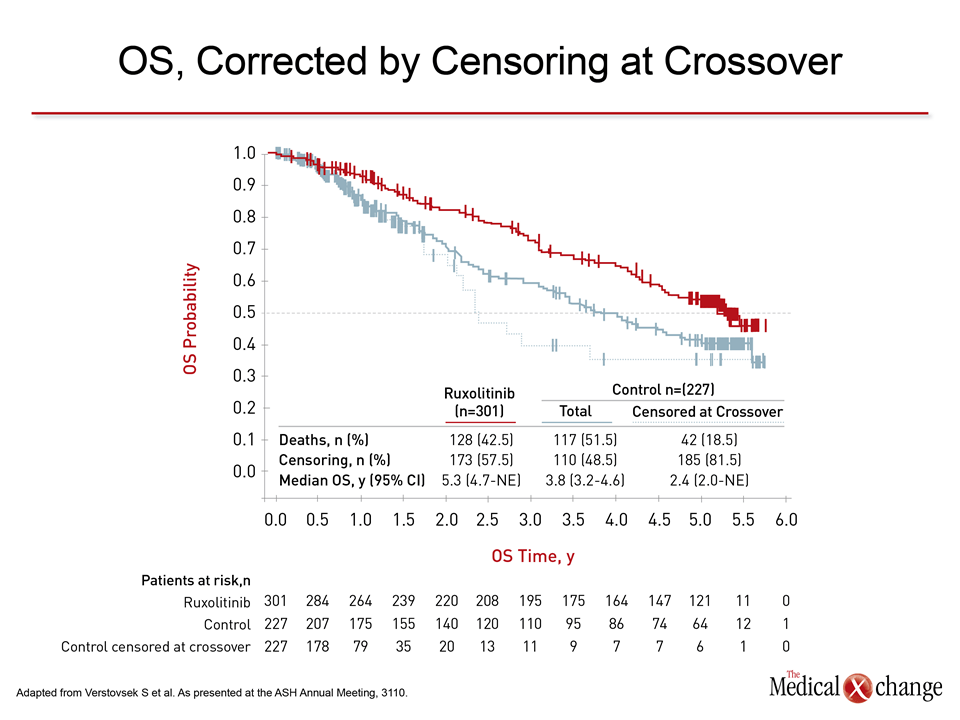
A separate intention-to-treat analysis of pooled data from the COMFORT studies generated the same conclusion (Verstovsek S et al. ASH 2016, abstract 3110). In the on-going analysis, 42.5% of those in the ruxolitinib group versus 51.5% of those randomized to a control group (placebo in COMFORT I and BAT in COMFORT 2) were alive at 5 years. Expressed as a hazard ratio (HR), ruxolitinib provided a 30% reduction in the risk of death (HR 0.70; P=0.0065) (Fig. 2). This advantage persists despite crossovers. In COMFORT I, control patients could receive ruxolitinib at the time of ≥25% increase in spleen volume. In COMFORT II, control patients were required to cross over to ruxolitinib when the study was unblinded. When OS was calculated censoring patients at the time of cross over, the reduction in risk of death climbed to 47% (HR 0.53; P=0.0013). Moreover, when comparing patients originally randomized to ruxolitinib to those who crossed over to ruxolitinib after correcting for the crossover with the rank-preserving structural failure time (RPSFT) method, the reduction in risk of death climbed to 65% (HR 0.35; P value not calculated for this exploratory analysis) (Fig. 3).
Earlier Treatment Linked to OS Advantage
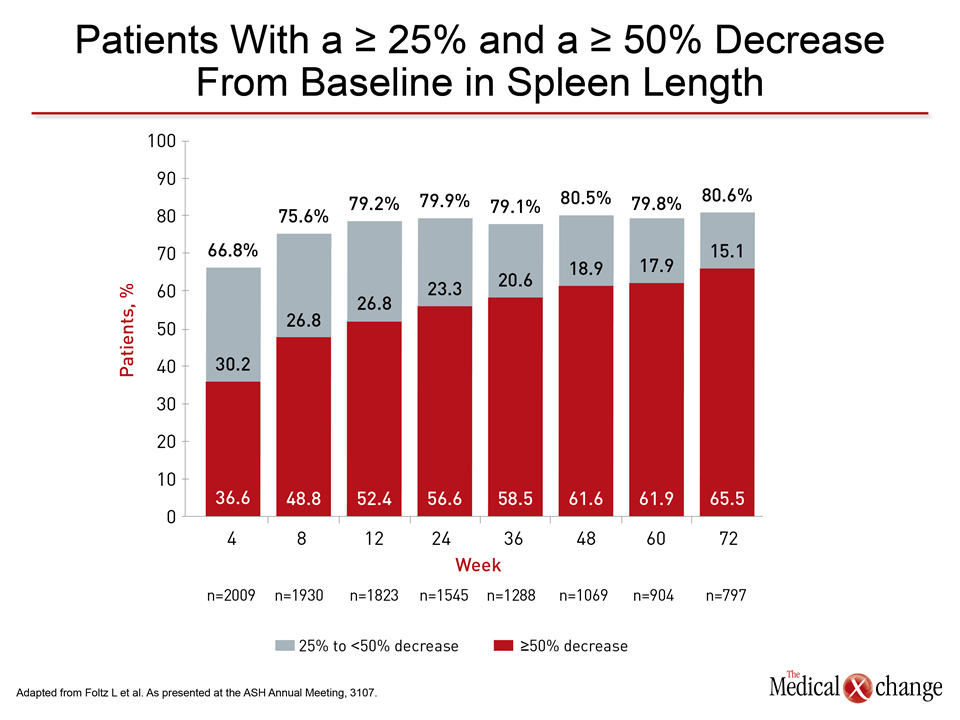
“These findings suggest that earlier treatment with ruxolitinib may improve the survival advantage for patients with MF,” reported the lead author of this analysis and the principal investigator of COMFORT I, Dr. Srdan Verstovsek, University of Texas M.D. Anderson Cancer Center, Houston. Supporting treatment at an early stage, he further noted a greater relative mortality benefit from ruxolitinib in those with intermediate- relative to high-risk MF (HR 2.55; P=0.0003). Yet, benefits in patients defined as high-risk by the International Prognostic Scoring System (IPSS) were large. The median OS in this population was 2.8 years, which significantly and substantially exceeds the 2.3 years in historical controls. At ASH, the safety and efficacy of ruxolitinib was provided additional support by a large expanded access study called JUMP (Foltz L et al. ASH 2016, abstract 3107). The goal of JUMP, which accrued data on 2233 patients in 26 countries including Canada, was to evaluate ruxolitinib outside of the confines of a phase 3 trial. “Clinically meaningful improvements in symptoms were seen as early as 4 weeks after the start of treatment and were maintained over time,” reported Dr. Lynda Foltz, St. Paul’s Hospital, University of British Columbia, Vancouver. As for spleen size, another metric for MF control, reductions climbed from baseline over the first 12 weeks and remained stable in follow-up out to 72 weeks (Fig. 4).
Hematologic Toxicities Manageable
In JUMP, as in the phase 3 trials, grade 3 or higher anemia (34.1%) and thrombocytopenia (16.3%) were common, but these “rarely led to treatment discontinuation,” Dr. Foltz reported. No non-hematologic events occurred at grade 3 or higher severity in more than 3% of patients. Even the most common non-hematologic adverse events, which included pyrexia (15.6%), asthenia (14.9%), and diarrhea (12.0%), occurred in modest frequencies. Infections were observed, including sepsis in 1.3% of patients, but only 2.8% of patients discontinued therapy due to infection. “Basically, these data confirm what was seen in the COMFORT trials,” Dr. Foltz reported. “Ruxolitinib was well tolerated and most patients experienced reductions in symptoms and splenomegaly.”
“In the expanded access study, “ruxolitinib was well tolerated and most patients experienced reductions in symptoms and splenomegaly.”
These data, however, do not directly answer the question of when ruxolitinib should be initiated. Asked specifically about the optimal time to start ruxolitinib in the course of MF, Dr. Foltz indicated that this cannot now be determined on the basis of objective data but involves a benefit-to-risk calculation based on patient-specific factors.
New Directions in MF Treatment
Other data on the treatment of MF that were presented at the ASH annual meeting suggest new directions of study in MF. In one study, JAK inhibition was evaluated as a strategy for improving the clinical parameters of MF candidates for HCT (Gupta V et al. ASH 2016, abstract 1126). In another, an experimental targeted agent called pacritinib was evaluated in MF patients with a low platelet count (Mascarenhas J et al. ASH 2016, LBA-5). In the trial of JAK inhibition for HCT candidates, ruxolitinib was administered for 56 days prior to initiating the conditioning regimen for transplant. The objective of this phase 2, multicenter study was to test the feasibility of reducing spleen size and inflammatory cytokine expression in an effort to improve performance status and favorably influence HCT outcome. Ruxolitinib was tapered and then discontinued before the conditioning regimen was initiated. Separate analyses were performed on those patients scheduled to receive an unrelated versus a related donor graft. In the unrelated donor arm, all 14 proceeded to transplant. Although there were 2 graft failures and 2 deaths within 100 days, ruxolitinib was associated with palpable reductions in spleen size, and there did not appear to be any adverse impact on post-HCT outcomes in this population, according to Dr. Gupta, who was also the principal investigator of this study. Conversely, the related donor graft arm of 7 patients was stopped prematurely. A predefined protocol rule for stopping was reached when two patients failed to proceed to transplant and a third patient had a graft failure. However, this early experience suggests that ruxolitinib can be tapered safely prior to the conditioning regimen. Dr. Gupta cautioned that ruxolitinib is not likely to be a standard pre-transplant approach in all MF patients scheduled for an unrelated donor HCT, but he suggested that further studies are warranted to assess whether this strategy offers an opportunity to improve outcomes.
Data from Halted Phase 3 Study
The pacritinib study, which is an inhibitor of JAK2, FLT3, IRAK1, and CSF1R, was presented as part of the Late-Breaking Abstracts Program. Enrollment in this phase 3 study, called PERSIST-2, was limited to MF patients with a baseline platelet count ≤100,000/μL. Data were presented on the first 311 patients enrolled before the study was stopped due to a clinical hold placed on pacritinib by the U.S. Food and Drug Administration (FDA). This action was prompted by unexpected vascular complications, including an intracranial hemorrhage and cardiac arrest, observed in PERSIST-1. In the PERSIST-2 follow-up to date, pacritinib was not associated with an increased risk of vascular events relative to BAT, according to the principal investigator Dr. John O. Mascarenhas, Icahn Mount Sinai School of Medicine, New York City, New York. Rather, the agent has so far been associated with acceptable toxicity, and it achieved a spleen volume reduction (SVR) of ≥35% relative to BAT (18% vs. 3%; P=0.001), although no OS benefit was observed.
“In my humble opinion, pacritinib is an effective drug in MF that deserves further evaluation.”
Noting that PERSIST-2 is the first trial to show a clinical benefit from a targeted agent in MF patients with the degree of thrombocytopenia required for entry, Dr. Mascarenhas said, “In my humble opinion, pacritinib is an effective drug in MF that deserves further evaluation.” It is unclear how the new data will affect further pacritinib development.
Summary
JAK inhibition has transformed the prognosis of MF, which, if untreated, is associated with a median survival of just 4 years in those with intermediate-risk disease and just 2 years in high-risk patients. Long-term outcome from the COMFORT trials, which confirmed improved OS, and the expanded access JUMP study, which confirmed acceptable safety and tolerability, establish ruxolitinib as a standard of care. While the proportion of candidates for potentially curative HCT remains small, efforts to treat MF earlier and to expand treatment options by targeting additional pathogenic pathways may further improve outcomes in patients with this disease.