Oncology
American Society of Clinical Oncology (ASCO) 2026 Annual Meeting
Fixed Combination of Checkpoint Inhibitors Maintain PFS and OS Advantage at 5 Years
Chicago –In a newly completed 5-year analysis of a global melanoma trial, the fixed-dose combination of nivolumab and relatlimab is still yielding a numerical overall survival (OS) advantage relative to nivolumab alone. The greater progression-free survival (PFS) on nivolumab and relatlimab was already significantly greater by 12 months after randomization. At 5 years, it remains significantly greater even after accounting for subsequent therapies. In terms of safety and tolerability, the rates of grade 3 or higher toxicities and discontinuations were only modestly elevated with the dual checkpoint inhibitor combination relative to nivolumab monotherapy.
The advantage of combining two checkpoint inhibitors was apparent when outcomes from this trial, called RELATIVITY-047, were first reported four years ago in the New England Journal of Medicine. In the trial, 714 patients with histologically confirmed unresectable stage III or IV melanoma were randomized in a 1:1 fashion to nivolumab + relatlimab or nivolumab alone.
Key Advantages Maintained after 3 and 5 Years of Follow-up
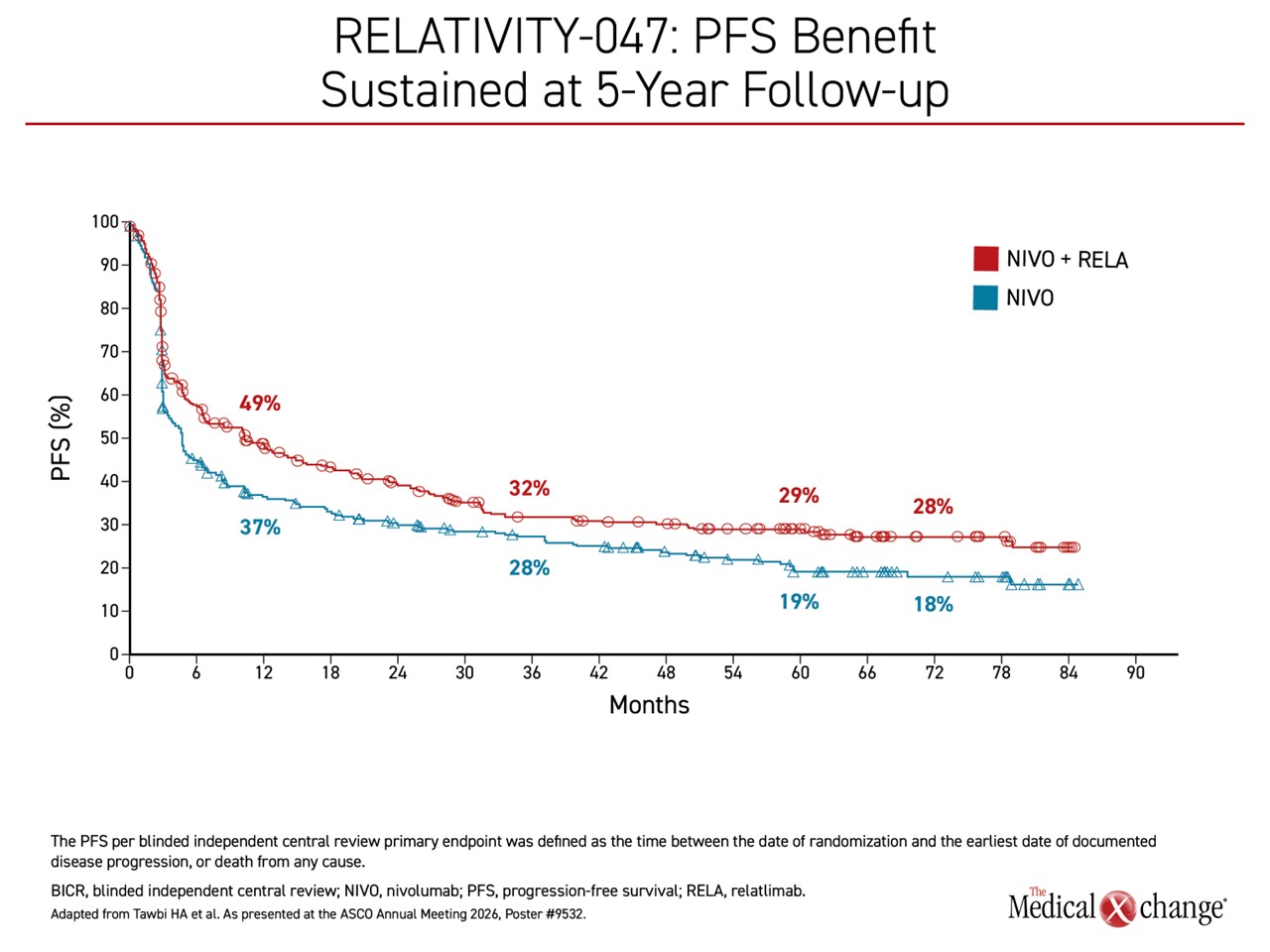
At 12 months the hazard ratio (HR) for the primary PFS outcome for the experimental arm relative to nivolumab monotherapy was already highly significant (HR 0.75; P=.006). Now, after 5 years, the relative advantage is almost unchanged (HR 0.77; 95% CI, 0.65 – 0.92) (Figure 1). There was a strong trend for an OS advantage for the combination relative to nivolumab alone by 3 years (HR 0.80; 95% CI 0.66 – 0.99) and this has been maintained at 5 years (HR 0.78; 95% CI 0.64 – 0.95).
The long-term outcomes, presented at the 2026 annual meeting of ASCO, “confirm the durable and clinically meaningful benefit” of combining the checkpoint inhibitors in previously untreated metastatic or unresectable melanoma, reported Dr. Hussein A. Tawbi, Principal Investigator of the RELATIVITY-047 trial and Professor in the Department of Melanoma Medical Oncology at the University of Texas MD Anderson Cancer Center in Houston.
“The long-term outcomes confirm the durable and clinically meaningful benefit of combining checkpoint inhibitors.”
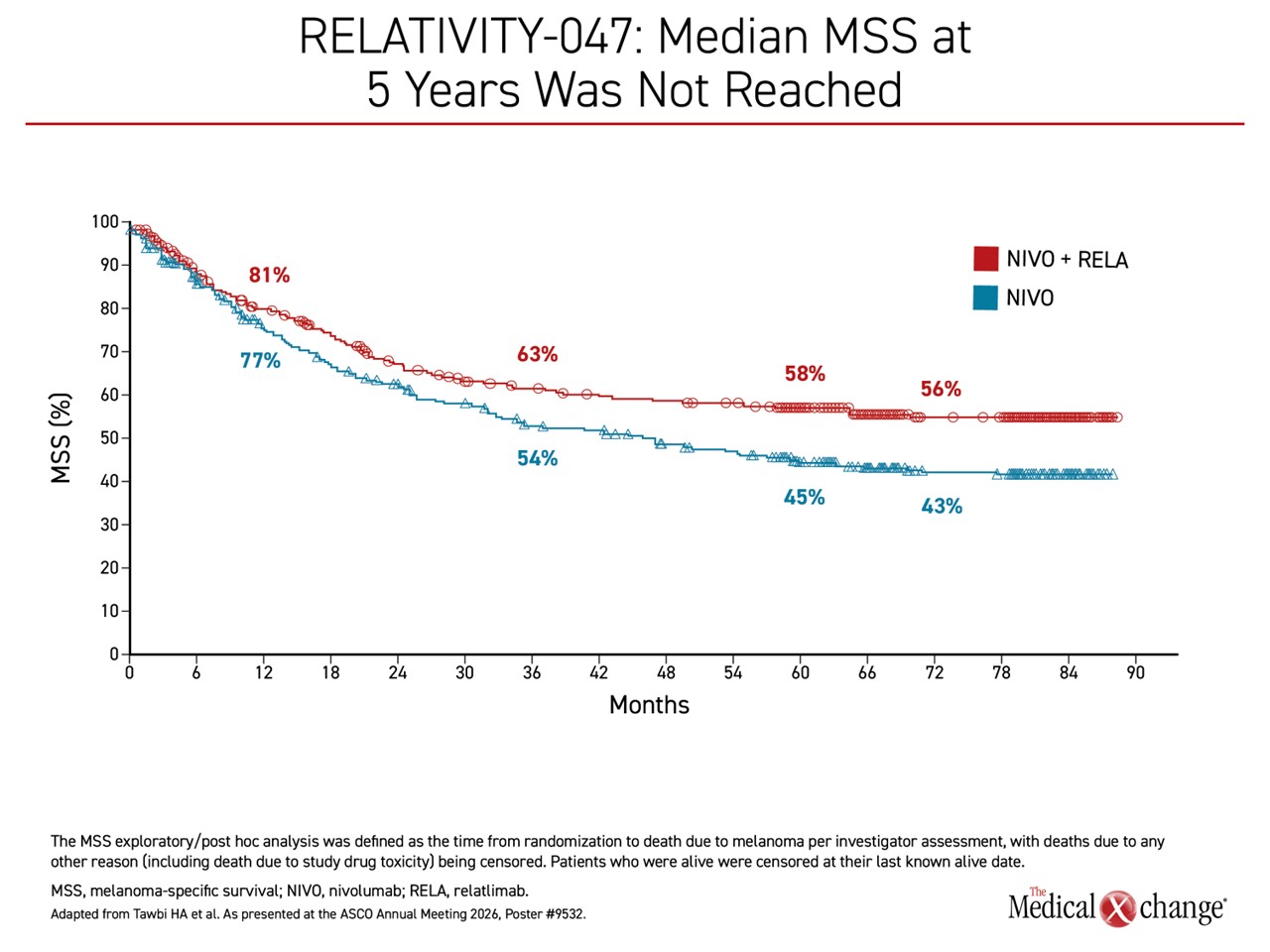
Equally supportive of the greater antitumour effect of the fixed-dose combination, the advantage for melanoma-specific survival (MSS) grew over time. The absolute difference at 12 months, favouring the combination was 4%. It reached nearly 10% at 3 years (HR 0.75; 95% CI, 0.64 – 0.94). By 5 years, the median MSS in the nivolumab + relatlimab arm has still not been reached versus 46.9 months in the nivolumab monotherapy arm (HR 0.71; 95% CI, 0.57 – 0.88) (Figure 2).
For an exclusive interview with Dr. Thiago Pimentel Muniz on the impact to clinical practice, click here
Overall, “we report the largest absolute differences in the landmark endpoints of PFS, OS, and MSS” between treatment strategies for metastatic and unresectable melanoma at 5 years, Dr. Tawbi reported.
Synergy of Dual Checkpoint Inhibition Supported
Nivolumab, is a programmed death 1 (PD-1) checkpoint inhibitor that was introduced to routine use in 2015. Relatlimab is a first-in-class inhibitor of the lymphocyte activation gene 3 (LAG-3) checkpoint, which, like PD-1, inhibits tumour-infiltrating lymphocytes (TILs) from targeting malignant cells. Dr. Tawbi explained that PD-1 and LAG-3, although independent inhibitors of TILs, are often co-expressed. The synergistic effect of inhibiting both types of checkpoints in experimental models provided the impetus for the clinical studies that led to the 2023 approval of nivolumab + relatlimab for advanced melanoma in Canada.
The nivolumab + relatlimab combination was subsequently listed as a preferred first-line therapy for metastatic or unresectable melanoma in several guidelines, including those issued by the National Comprehensive Cancer Network.
Despite the established role of this fixed-dose combination, the 5-year results have provided an important opportunity to confirm an extended benefit in the context of numerous pre-planned secondary outcomes and exploratory analyses. This includes response rates among subgroups, such as those stratified by immune checkpoint ligand expression at baseline, response and survival following second-line therapies. The 5-year safety data also inform its utility in routine practice.
Benefit Observed Regardless of Programmed Death-ligand 1 (PD-L1) Expression
Of 5-year findings, PD-L1 expression ≥1% did not predict benefit or absence of benefit for the combination relative to nivolumab alone. Although the greater median PFS of the dual checkpoint inhibitors (18.0 vs. 14.7 months) did not reach statistical significance over long-term follow-up among those with ≥1% PD-L1 level, it was highly significant for those with lower PD-L1 expression (<1%). In this latter group, the median PFS (6.7 vs. 3.0 months; HR 0.66; 95% CI, 0.53 – 0.83) was more than doubled (Figure 3).
Similarly, the risk of death as expressed by the median OS (38.3 vs. 25.4 months) was also significantly reduced (HR 0.76; 95 % CI, 0.60 – 0.98) as was the risk of melanoma-specific death as expressed by MSS (not reached vs. 35.4 months; HR 0.69; 95% CI, 0.52 – 0.91) among those with PD-L1 expression <1%. In those with PD-L1 expression ≥1%, the curves for both outcomes separated at about 36 months and remained so over follow-up to date. The risk reductions for OS (HR 0.81; 95% CI 0.46 – 1.15) and MSS (HR 0.75; 95% CI 0.59 – 1.11) in patients with PD-L1 ≥1% fell short of significance but were consistent with overall results.
An analysis of cluster of differentiation 8 (CD8) T-cell subsets found the greatest separation in the OS curves among those with PD-L1 ≥1% and low levels of PD-1+ CD8+ T cells and among those with PD-L1 ≥1% and high levels of LAG-3+ CD8+ T cells. The difference was smaller in those with the opposite characteristics (PD-L1 ≥1% but high levels of PD-1+ CD8+ T cells and PD-L1 ≥1% with low levels of LAG-3+ CD8+ T cells), but there was a numerical advantage for the nivolumab + relatlimab combination relative to nivolumab monotherapy for all groups.
Improved Overall Survival Regardless of Second-line Therapy Following Progression
At 48 months, whether by PFS or OS, outcomes from the start of second-line therapy were substantially better for those who received nivolumab + relatlimab first-line. PFS on second-line therapy with nivolumab + ipilimumab was more than double on those who first received dual checkpoint inhibition (8.4 vs. 3.1 months). When measured from start of second-line therapy, OS was longer in the group randomized at the start of the trial to the fixed-dose combination (not reached vs. 21.6 months).
PFS at 48 months was greater for the combination after any second-line therapy. These were 42% versus 10% after nivolumab + ipilimumab, 11% versus 0% after ipilimumab, and 34% versus 12% after BRAF/MEK inhibitors. For OS, a similar marked advantage for first-line treatment with the fixed-dose combination was seen for nivolumab + ipilimumab (71% vs. 27%), ipilimumab alone (22% vs. 12%) and BRAF/MEK inhibitors (32% vs. 18%).
The median time to the next treatment following the start of a second-line therapy was also numerically higher in the group initially randomized to the fixed-dose combination relative to nivolumab monotherapy for both nivolumab + ipilimumab (8.4 vs. 5.4 months) and the BRAF/MEK inhibitor combination (12.4 vs. 10.8 months), whereas no such trend was observed for ipilimumab monotherapy (4.2 vs 5.3 months).
For OS at 48 months, the same consistent advantage was observed among those initially randomized to nivolumab + relatlimab after second-line nivolumab + ipilimumab (71% vs. 27%), ipilimumab monotherapy (22% vs. 12%) and BRAF/MEK inhibitors (32% vs. 18%).
Prolonged Time to Development of New Brain Lesions
Nivolumab + relatlimab is known to cross the blood-brain barrier, which is likely to explain the lower rate of lesions on this therapy than nivolumab alone in the central nervous system (CNS) among patients without CNS metastases at baseline (4.6% vs. 7.5%). Time to formation of new lesions (10.9 vs. 7.6 months) was also longer in the group receiving dual checkpoint inhibitors.
Safety Remains Consistent Over Time
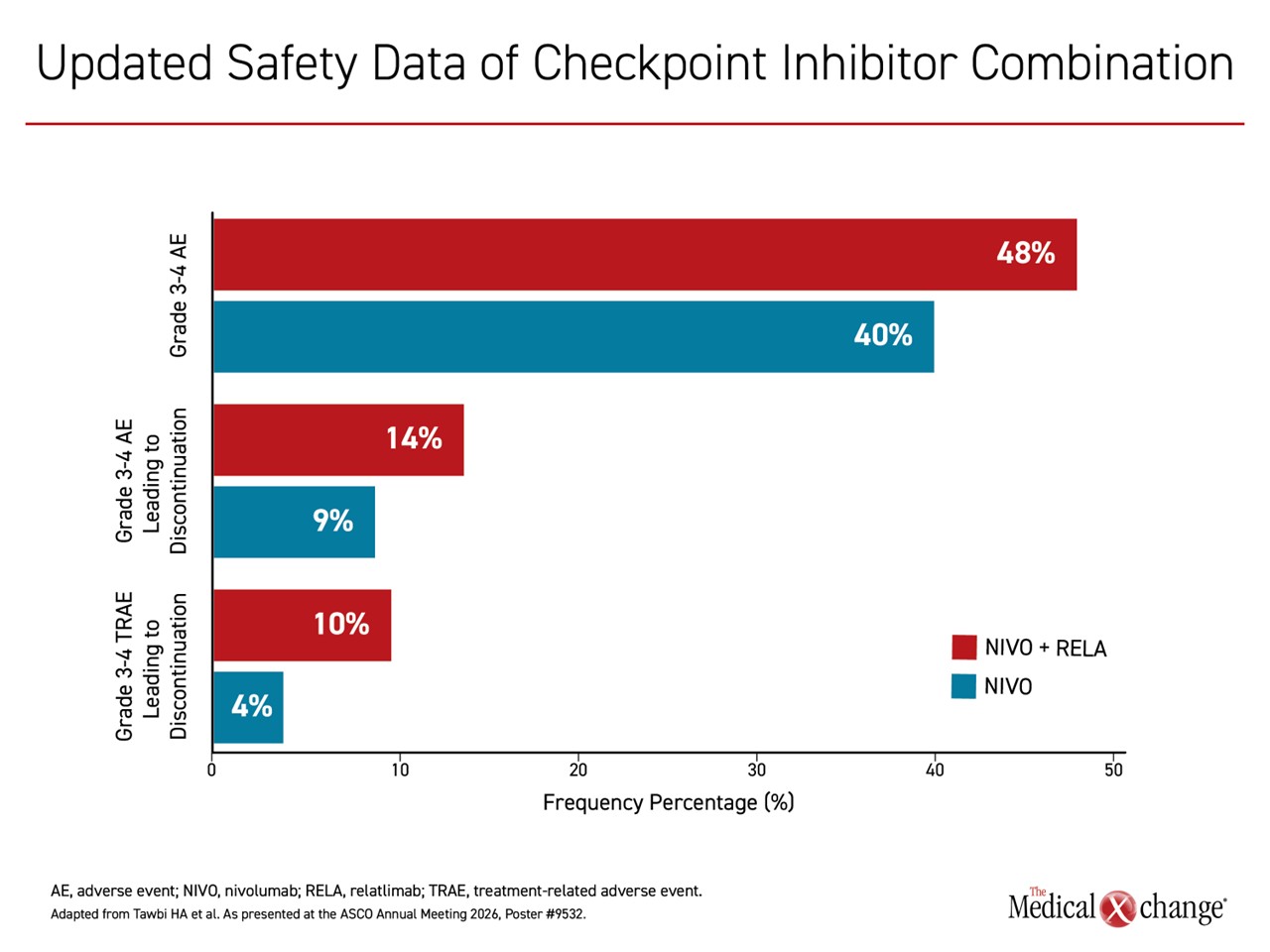
No new adverse events considered to be related to the initial treatment assignment were reported in this most recent follow-up, but, as reported previously, adverse events were more common in the first years of therapy among those randomized to the fixed-dose combination of checkpoint inhibitors. The rate of any adverse events considered to be treatment related was higher (85% vs. 74%) even if the difference in grade 3 or higher adverse events was more modest (23% vs. 12%). The proportion of any treatment-related adverse events leading to discontinuation was 18% vs. 10%. For grade 3 or higher treatment-related adverse events, the rates were 10% and 4%, respectively (Figure 4).
“The safety remained consistent with prior reports.”
The six deaths in RELATIVITY-047 occurred early in the trial. The 4 deaths in the nivolumab + relatlimab arm were described as one case of hemophagocytic lymphohistiocytosis, one case of acute edema of the lung, one case of pneumonitis, and one case of multiorgan failure. The two deaths in the nivolumab monotherapy arm involved one case of sepsis and myocarditis and one case of pneumonia.
The concept of employing dual checkpoint inhibitors to improve an antitumour effect over one alone was pioneered with nivolumab plus the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor ipilimumab. There have been no large randomized trials to compare these two checkpoint inhibitor combinations in melanoma, but Dr. Tawbi noted that there are no comparable long-term benefits relative to a checkpoint inhibitor monotherapy with the nivolumab + ipilimumab combination.
Conclusion
Checkpoint inhibitors have dramatically improved the likelihood of extended survival in patients with metastatic or unresectable melanoma, but 5-year outcomes show that combining inhibitors of different checkpoints can provide meaningful improvements in response and subsequent PFS, OS, and MSS in long-term follow-up. The extended survival with nivolumab + relatlimab was preserved over nivolumab monotherapy regardless of second-line therapy, and outcomes were generally superior across subgroups, including those defined by PD-L1 expression. The results are expected to strengthen the current status of nivolumab + relatlimab as a preferred first-line therapy in advanced melanoma.