Nephrology
American Society of Nephrology: Kidney Week 2011
Serum Uric Acid Emerging as Sensitive Risk Factor for Cardiovascular Disease, Renal Disease, and Death
Philadelphia – Elevated serum uric acid (SUA) is an important treatable biomarker for renal and cardiovascular (CV) disease, according to data presented at Kidney Week 2011. Elevated SUA was associated with progressive renal disease, increasing rates of CV events, and mortality. These associations persist after controlling for co-morbidities. In one study, the mortality risk climbed even higher in patients with both elevated SUA and gout. Data presented here support screening for elevated SUA and implementing effective intervention when levels are elevated.
Serum Uric Acid a Useful Biomarker
Treatment for symptomatic elevations in serum uric acid (SUA) is standard practice, but new evidence consolidates a link between SUA and progressive end-organ dysfunction even in asymptomatic patients. A large body of data, enriched by four new studies presented during Kidney Week 2011, indicates that elevated SUA is a useful biomarker and a potentially treatable risk factor for renal dysfunction, cardiovascular (CV) events, and death.
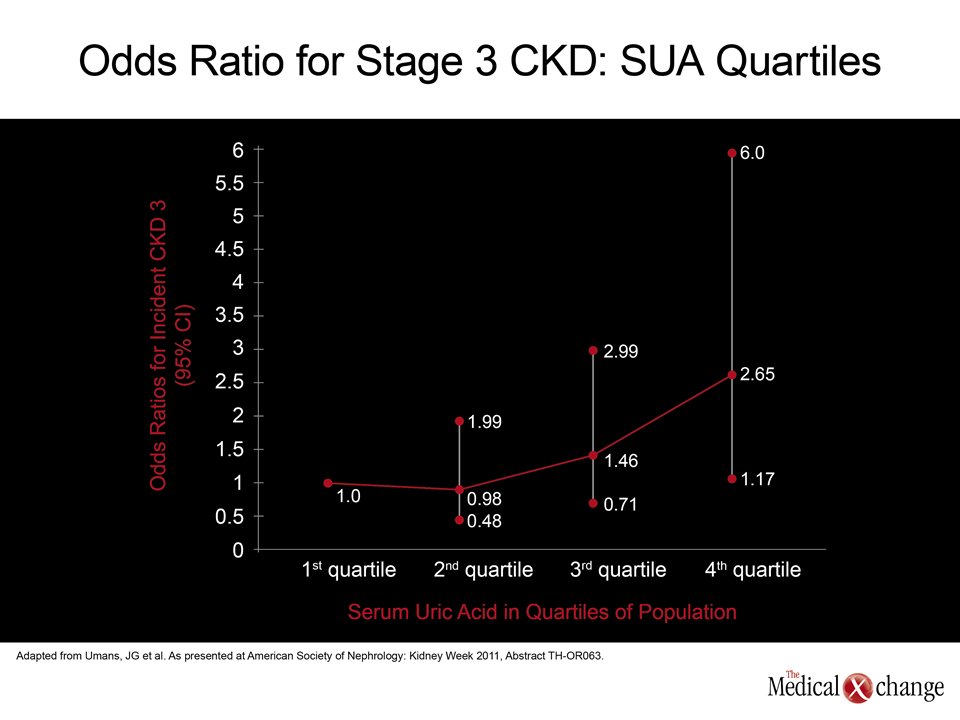
“Recent data suggest incremental changes in SUA may be more sensitive than serum creatinine in detecting increasing impairment in kidney function.”
“Hyperuricemia has been associated with chronic kidney disease (CKD) and with hypertension. It is also common in the metabolic syndrome. “Recent data suggest incremental changes in SUA may be more sensitive than serum creatinine in detecting increasing impairment in kidney function,” reported Dr. Jason G. Umans, PhD, MedStar Health Research Institute, Georgetown-Howard Universities Center for Clinical and Translational Science, Washington, DC. A study led by Dr. Umans was designed specifically to evaluate the prognostic value of elevated SUA for CKD. A five-year follow-up was conducted in 2,896 participants without hyperalbuminuria or significant decline in renal function at baseline. The group was recruited from the Strong Heart Family Study, which is following 3,665 American aboriginal adults. This population, with a 23% incidence of diabetes mellitus (DM), a 57% incidence of obesity (BMI >30), and a 33% incidence of hypertension, is frequently evaluated for modifiable risk factors because of their high rates of CV risk. When stratified by SUA quartile, the odds ratio (OR) for stage 3 CKD was more than twice as high in the highest SUA quartile when compared to the lowest. While it is true that this group also had the highest incidences of obesity and DM, elevated SUA remained an independent risk factor after controlling for these factors, according to Dr. Umans (Fig. 1). In another trial, mortality was the endpoint. In this study, 80 elderly patients who were clinically stable but had a high rate of CV risk factors, including hypertension (83%) and diabetes (35%), were placed into two groups: those with higher-than-median SUA (>5.85 mg/dL), or those with lower-than-median (<5.85 mg/dL). When compared for rates of death, the differences were striking.
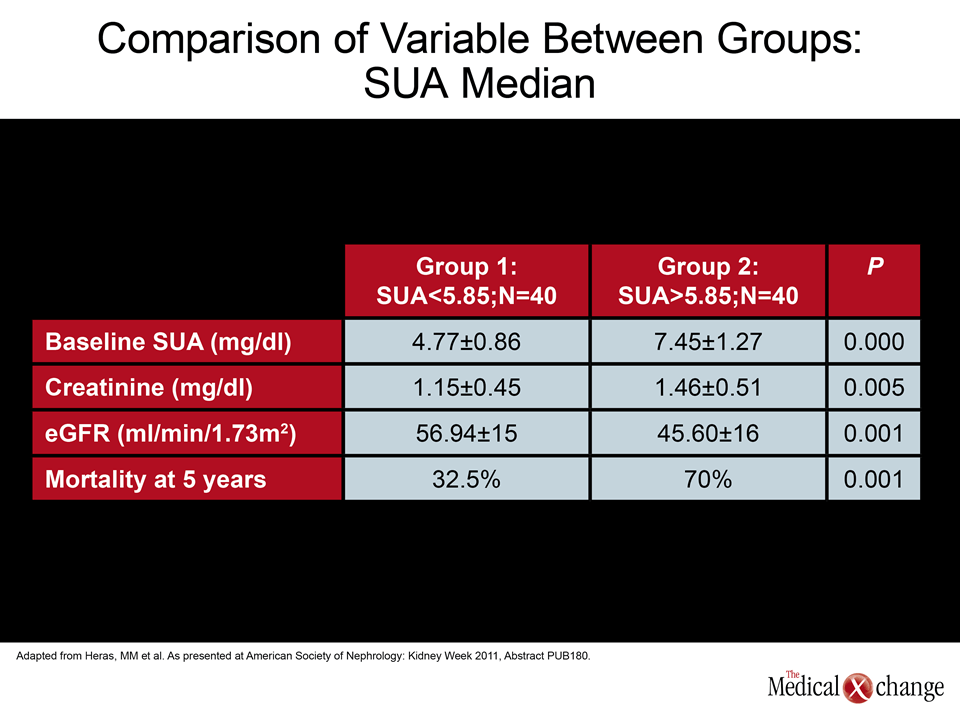
“The mortality in the group with the higher-than-median SUA had more than double the mortality.”
“The mortality in the group with the higher-than-median SUA had more than double the mortality [70% vs. 32.5%; P=0.001].” In a logistic regression analysis that included age, gender, Charlson index, history of heart failure, serum creatinine, eGFR, and SUA, only age and SUA were independently associated with mortality,” reported Dr. Manuel M. Heras, Department of Nephrology, General Hospital, Segovia, Spain (Table 1). Mortality was also evaluated in a much larger U.S. cohort of 15,773 subjects over the age of 20 who were drawn from the third National Health and Nutrition Examination Study. In this population, considered representative of U.S. adults, SUA and physician-diagnosed gout were assessed in the context of renal function stratified by eGFR 90 ml/min. Total mortality and CV mortality were then evaluated relative to both SUA and eGFR over time. In a 10-year follow-up, the total mortality in this population was 9.7%, and CV mortality accounted for nearly half (4.4%). Gout was associated with a significant 30% increase (OR 1.3, 95% CI 1.03-1.65) in risk of total mortality and a 50% increase in CV mortality (OR 1.5, 95% CI 1.08-2.07) after adjusting for age and known CV risk factors. However, this risk increase was seen only in those patients with eGFR <90 ml/min (the two groups with the lowest renal function). In addition, the risk of total mortality climbed 12%, and the risk of CV mortality by 10%, for every 1 mg/dL increase in SUA in those patients with eGFR <90 ml/min (Fig. 2).
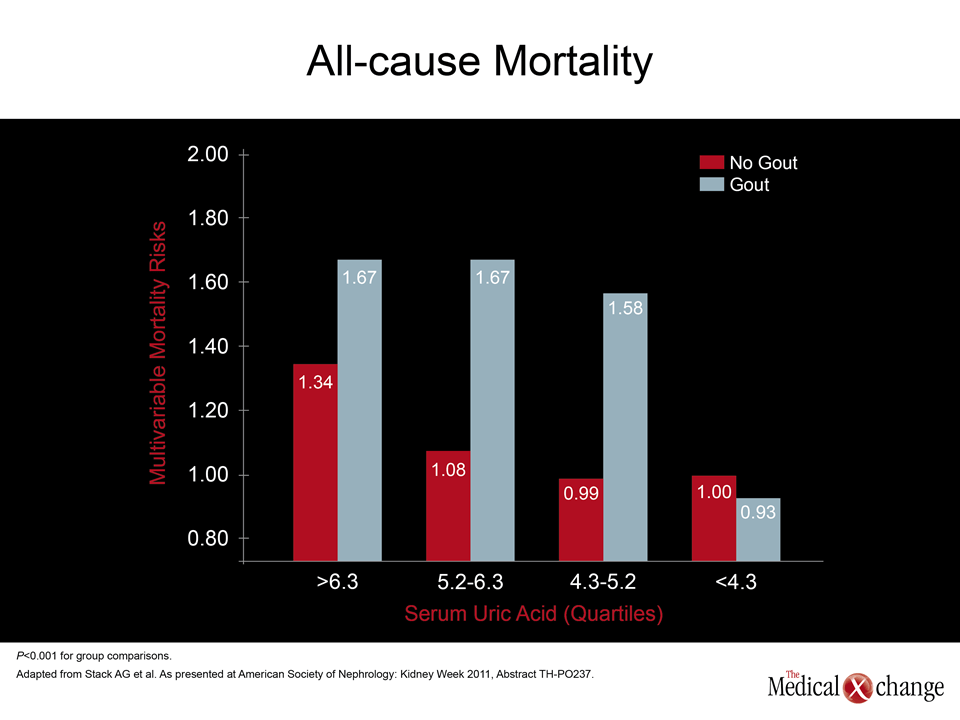
“When we looked at the presence of gout in relationship to quartiles of SUA, we saw large increases in the risk of all-cause mortality.”
“When we looked at the presence of gout in relationship to quartiles of SUA, we saw large increases in the risk of all-cause mortality,” reported Dr. Austin G. Stack, Regional Kidney Center, Letterkenny General Hospital, Donegal, Ireland. While gout and hyperuricemia were independent risk factors for increased mortality, “the risks were greatest in those patients with elevated SUA who also had gout.” In a fourth study, conducted in Japan, the relationship between eGFR and SUA was evaluated in 16,796 patients whose values were measured twice over a 10-year period. After adjusting for age, gender, and baseline eGFR, a tight relationship was observed between SUA and eGFR so that change in either direction (lower or higher) was tracked by change in the other variable. According to the lead investigator, Dr. Kunitoshi Iseki, University Hospital of the Ryukyus, Okinawa, Japan, SUA is not only a good surrogate for renal function but “these results suggest that maintaining a normal range of SUA is important for maintaining a normal level of eGFR.”
Conclusion
Based on emerging data, prevention of hyperuricemia has immediate implications for preventing renal disease and a large potential for reducing CV events and mortality, both of which are closely linked with renal impairment. Ultimately, the data associating elevated SUA with elevated total mortality provides the most compelling evidence that high-risk patients should be routinely screened for uric acid levels and placed on treatment if levels are elevated.