Expert Review
Cardiovascular Disease: Expert Review and Commentary from Published Literature
Bringing Patients with Type 2 Diabetes to LDL-C Goals
Robert A. Hegele, MD, FRCPC, FACP, FAHA, FCAHS
Martha G. Blackburn Chair in Cardiovascular Research and Canada Research Chair
Robarts Research Institute, University of Western Ontario, London, Ontario
Reiterated in the 2013 Canadian Diabetes Association (CDA) guidelines, the primary goal for low-density lipoprotein cholesterol (LDL-C) in patients with type 2 diabetes mellitus (T2DM) is ≤2.0 mmol/L.(1) Even though LDL-C levels are often only modestly elevated in T2DM patients,(2) the same strict LDL-C target applies as in other high-risk patients without T2DM, including those who have had a previous cardiovascular event.(3) In patients with T2DM, the first-line therapy for reaching LDL-C goals is typically an HMG CoA reductase inhibitor (statin). The second-line agents, used adjunctively, or in the case of intolerance, as a substitutefor statins, are listed in the CDA guidelines alphabetically as bile acid sequestrants, a cholesterol absorption inhibitor, fibrates and nicotinic acid formulations. Each second-line drug has its own particular benefits and shortcomings. The second-line lipid-modifying agents may help patients with T2DM reach LDL-C targets, but their use should be individualized based on the anticipated benefit derived from their specific therapeutic profiles.
Background
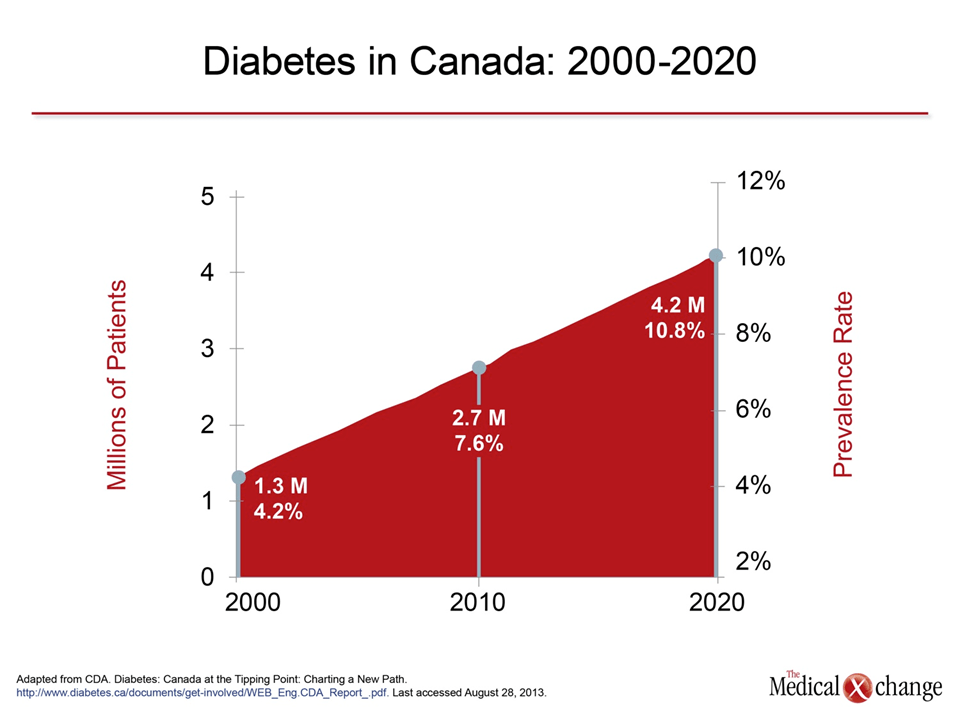
In most industrialized countries, including Canada, increasing rates of obesity together with an aging population have contributed to a steep rise in the incidence and prevalence of diabetes, mainly type 2 diabetes (T2DM) (Fig. 1).(4) with T2DM, relative to non-diabetic individuals, have more than double the risk of major adverse cardiovascular disease (CVD) outcomes, including myocardial infarction (MI) and stroke.(5) Since CVD is by far the most important cause of death in T2DM,(6) and since projected T2DM rates will continue to increase, there is a pressing need to intervene aggressively upon CVD risk factors in these patients. The large reductions in CVD risk achieved by patients with T2DM who reach low-density lipoprotein cholesterol (LDL-C) targets are comparable to those observed in other high-risk populations. For instance, in a meta-analysis of 26 randomized lipid-lowering trials with data on more than 170,000 individuals, each 1.0 mmol/L reduction in LDL-C was associated with a ~21% reduction in CVD events across risk groups independent of the baseline LDL-C.(7) Reduction of LDL-C in patients with T2DM may reduce CVD risk to an even greater degree. For instance, in the Collaborative Atorvastatin Diabetes Study (CARDS), the first statin trial conducted specifically in patients with T2DM, treatment with atorvastatin 10 mg reduced LDL-C from a mean baseline level of 3.1 to 2.0 mmol/L, and reduced CVD events by 37%.(8)
In a survey from 2011 of more than 22,000 outpatients with diabetes on statins in Canada and Europe, slightly more than 40% were not at target LDL-C levels.
In patients with T2DM, subgroup analyses that stratified patients according to baseline LDL-C levels indicated consistent relative reductions in CVD risk with LDL-C lowering, irrespective of baseline LDL-C levels.(9) The Canadian Cardiovascular Society (CCS) and Canadian Diabetes Association (CDA) are thus consistent with respect to the recommended target LDL-C ≤2.0 mmol/L in patients with T2DM (with alternate targets of non-HDL-C <2.6 mmol/L and apo B <0.8 g/L if LDL-C is not reported or unavailable).(1,3) An important clarification in the new guidelines is that a diabetic patient of either type is considered to be at high-risk if: 1) diabetes has been present for >15 years; or 2) the patient’s age is >40 years. There is also emerging evidence that reducing LDL-C even lower than 2.0 mmol/L may yield additional benefits;(7)this issue will be resolved definitively by studies to be published soon. But even at current target LDL-C levels, there is a large unmet need for many Canadian patients with T2DM. For instance, in a survey from 2011 of more than 22,000 outpatients with diabetes on statins in Canada and Europe, slightly more than 40% were not at target LDL-C levels.(10) This calls for more assertive treatment and for a wider range of treatment options in T2DM patients at high CVD risk.
Statins and Adjunctive Therapies
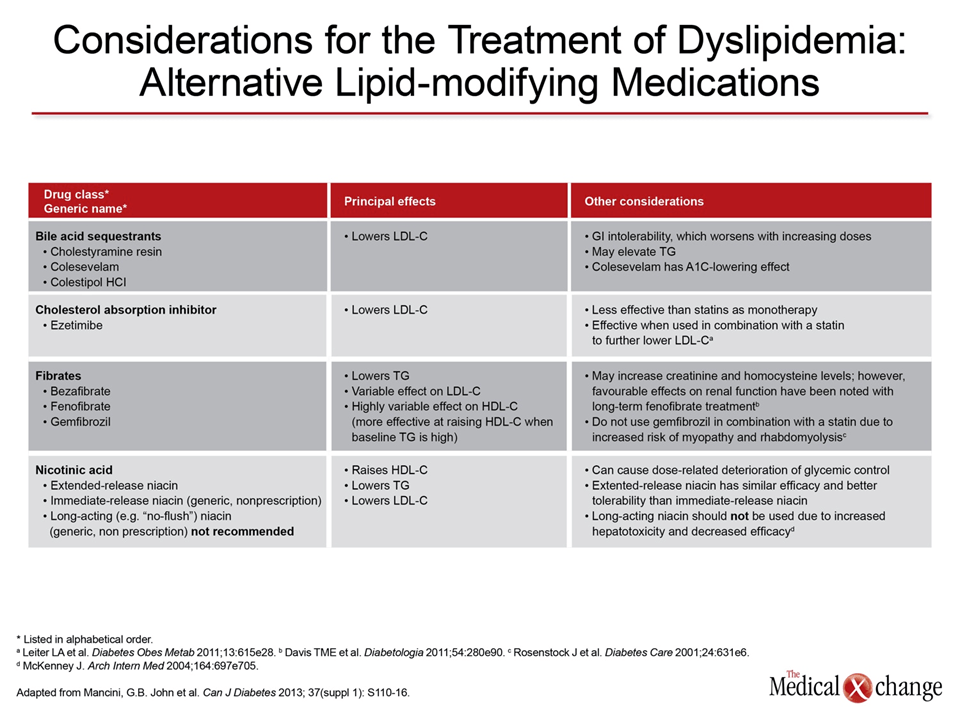
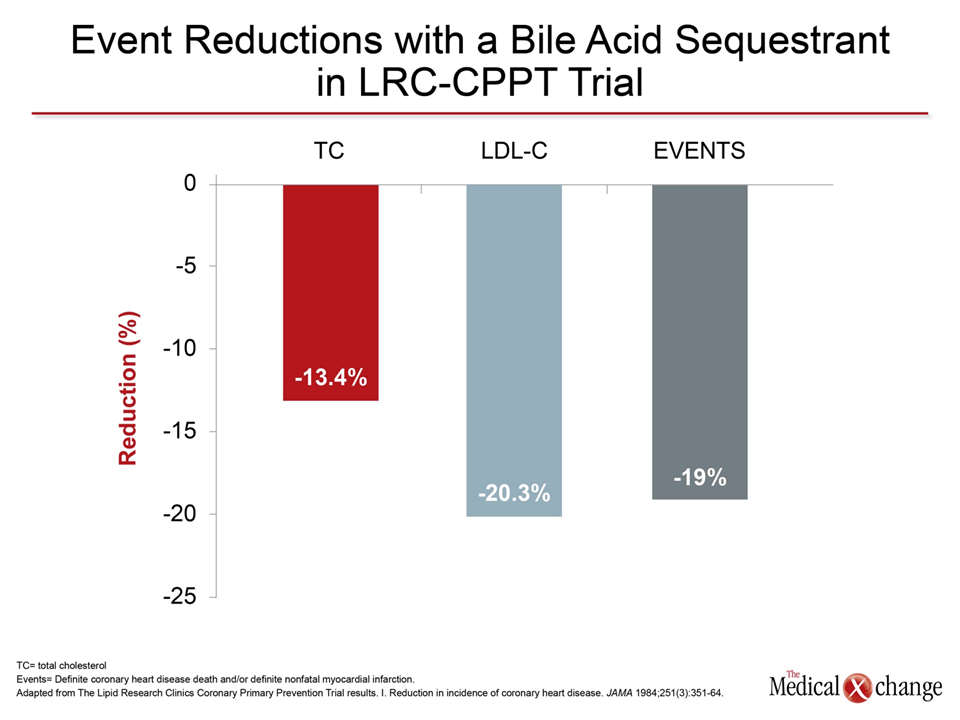
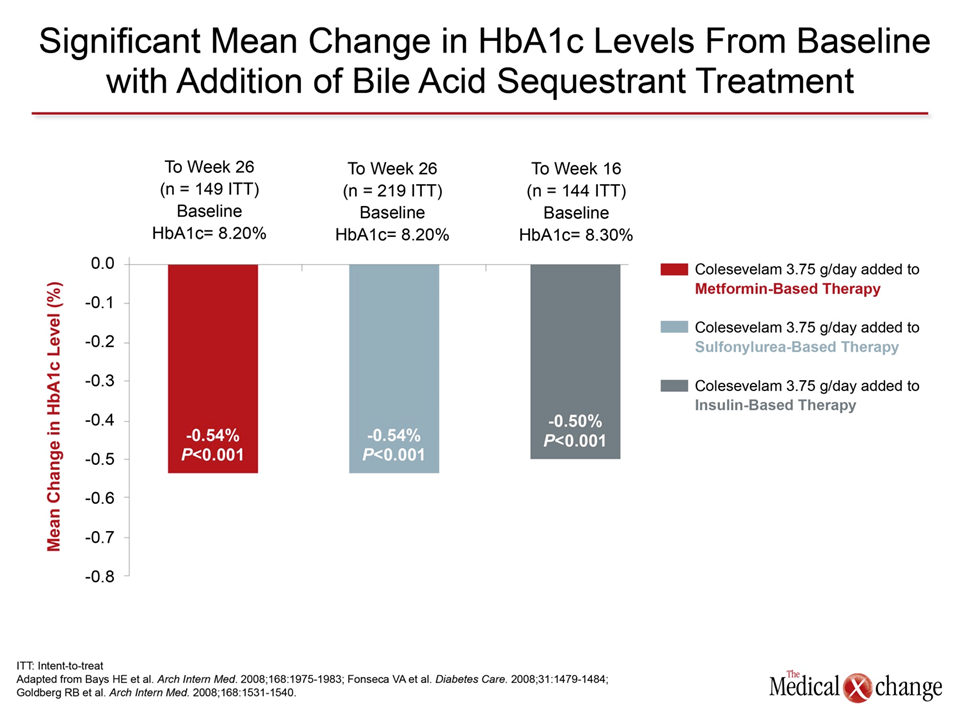
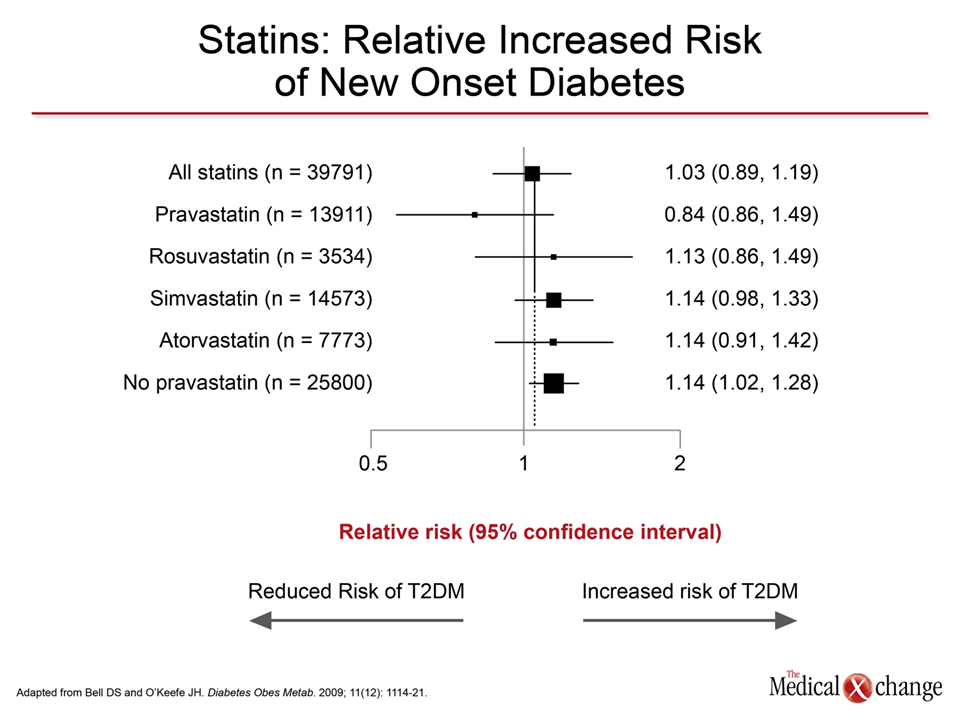
Target LDL-C reductions are reached in patients with T2DM, like others, through a multi-dimensional CVD risk reduction strategy. Lifestyle modifications, such as a healthy diet, maintaining ideal body weight and exercise, are the foundation of treatment for T2DM, although these interventions offer only a modest immediate effect on LDL-C.(11) Amongst pharmacological agents, statins provide the greatest relative reductions in LDL-C. But despite the positive impact of statins on CVD management, some patients have issues with statin intolerance, while others fail to reach LDL-C targets despite taking appropriate doses. Although serious adverse events from statins are rare,(12) community-based studies indicate that annoying muscle symptoms are experienced by 10% to 15% of statin-treated patients; these appear to be dose-related.(13) Alternative lipid-modifying therapies listed in the 2013 CDA guidelines (Table 1) can play an essential role not only in CVD risk reduction in statin-intolerant individuals, but may also allow some patients to continue better-tolerated low-dose statin therapy, while simultaneously enabling them to attain target LDL-C levels. For the goal of lowering LDL-C in patients with T2DM in particular, bile acid sequestrants deserve attention. Used widely for LDL-C reductions and CVD risk management before the introduction of statins, bile acid sequestrants were among the first lipid-modifying agents to demonstrate CVD risk reduction in a randomized trial.(14) Specifically, in the Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT), published almost 30 years ago, the older bile acid sequestrant cholestyramine was shown to reduce LDL-C by 20%, total cholesterol by 13%, and CV death and MI by 19% (Fig. 2). Recent randomized event trials with other second-line agents added to baseline statin therapy, such as niacin for secondary prevention in the AIM-HIGH (15) and HPS2-THRIVE trials, (16) or fenofibrate for T2DM patients in the ACCORD trial,(17) have failed to show significant reductions in event rates, although ezetimibe plus a statin did achieve a reduction in major atherosclerotic events in patients with renal dysfunction.(18) Bile acid sequestrants typically lower LDL-C by about 15% to 20% when used in standard dosages as monotherapy.(19) Due to an independent mechanism of action, similar relative reductions are achieved on top of statins when bile acid sequestrants are used adjunctively.(20) In the treatment of LDL-C in T2DM, the bile acid sequestrant colesevelam has the additional advantage of improving glycemic control. In a series of placebo-controlled studies, HbA1c levels were reduced by a consistent 0.5% when colesevelam combined with metformin,(21) a sulfonylurea,(22) or insulin (Fig. 3) compared to placebo combined with these treatments.(23) The favourable effect on HbA1c is particularly important considering the recent appreciation of the modest but negative influence of statins on several measures of glycemic control, including HbA1c and development of new-onset diabetes.(24) Originally documented with rosuvastatin, the slightly increased risk of worsened glycemia appears to be shared amongst most members of the statin class (Fig. 4). Of course, this adverse effect should pose no impediment to the use of statins, given their major CVD benefit in patients with T2DM.(25) The potential for colesevelam to protect against or delay development of T2DM in patients with metabolic syndrome and insulin resistance is intriguing but is so far unproven.(26) Several potential disadvantages of bile acid sequestrants have been largely circumvented by the introduction of colesevelam in a tablet formulation, particularly the steps required for preparation and the adverse taste of the powder formulations. Colesevelam does not undergo intestinal absorption, thereby greatly reducing the risk of adverse events.(27) Side effects, including constipation and other adverse events affecting the gastrointestinal tract, are typically reported at rates only slightly above those of placebo.(28) However, bile acid sequestrants may not be the optimal choice for reducing LDL-C in all individuals with T2DM, particularly those with concomitant moderate to severe hypertriglyceridemia (defined as TG >3.0 mmol/L). Because bile acid sequestrants can raise triglyceride levels, alternative agents, such as fibrates or niacin, may be more appropriate in hypertriglyceridemic individuals. Of these adjunctive lipid-modifying agents, fenofibrate is particularly attractive in patients with T2DM because of recent evidence that this agent may reduce the microvascular complications of T2DM, such as neuropathy and retinopathy,(29-30) by an effect independent of its effects on lipids. Fibrates reduce TG levels in patients with hypertriglyceridemia and also increase LDL particle size, which is felt to further reduce the risk of atherosclerotic end points.(31) While fenofibrate and bezafibrate are usually well tolerated in combination with a statin; gemfibrozil is not recommended for use in combination with statins because of an increased risk of rhabdomyolysis.(32)
Beyond LDL-C
Addressing lipid markers other than LDL-C, as outlined in the CDA 2013 guidelines, is challenging due to the incomplete evidence of clinical benefits of altering these markers specifically and independent of LDL-C. While substantial epidemiologic evidence supports the clinical relevance of such secondary lipid markers as HDL-C, apo A-1, Lp(a), very low density lipoprotein (VLDL), and total cholesterol-to-HDL-C ratio for predicting future risk of a CVD event, there is inconsistent prospective evidence to confirm that active pharmacological treatment of these risk markers alters CVD outcomes. Indeed, negative results with several trials attempting to treat beyond LDL-C, such as ACCORD, which compared simvastatin plus fenofibrate or placebo in T2DM patients,(33) and AIM-HIGH and HPS2-THRIVE, which compared statin plus niacin or placebo in high-risk patients, is a key reason to re-focus efforts to control LDL-C (and its related biomarkers non-HDL-C and apo B) ahead of the other lipid risk markers.
Among high-risk groups of patients, those with T2DM in particular may benefit from concerted efforts to bring all risk factors to goal. In addition, risk factors appear to be additive. Failure to treat to evidence-based targets suggests a missed opportunity to lower risk of major events.
Control of LDL-C in patients with T2DM should not be considered adequate unless the treatment goal of ≤2.0 mmol/L has been reached. Obviously, in patients with T2DM, other major risk factors, such as hypertension or hyperglycaemia, should be treated with equal rigor and adherence to targets recommended by national guidelines. Among high-risk groups of patients, those with T2DM in particular may benefit from concerted efforts to bring all risk factors to goal. In addition, risk factors appear to be additive. Failure to treat to evidence-based targets suggests a missed opportunity to lower risk of major events.
Summary
Assertive control of lipids in patients with T2DM is an essential step to prevent CVD events, which are by far the most significant cause of death and disability in these individuals. Statins are the most effective treatment, and remain first-line therapy despite their limitations. But only a portion of patients with T2DM can reach guideline targets on statins alone at doses that are acceptably tolerated. In addition, statins sometimes can have a mild counterproductive effect on glucose control. Among the alternative or adjunctive treatments to statins, bile acid sequestrants, and colesevelam in particular, may increase the likelihood that T2DM patients with normal TG levels will achieve and remain at LDL-C treatment goals and may experience concomitant improvement in HbA1c.
References
1. Canadian Diabetes Association Clinical Practice Guidelines. 2013. (Accessed August 19, 2013, at http://guidelines.diabetes.ca/Browse/Chapter24.) 2. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106(25):3143-421. 3. Anderson TJ, Gregoire J, Hegele RA, et al. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2013;29(2):151-67. 4. CDA. Diabetes: Canada at the Tipping Point: Charting a New Path. http://www.diabetes.ca/documents/get-involved/WEB_Eng.CDA_Report_.pdf Last accessed August 28, 2013. 5. Almdal T, Scharling H, Jensen JS, Vestergaard H. The independent effect of type 2 diabetes mellitus on ischemic heart disease, stroke, and death: a population-based study of 13,000 men and women with 20 years of follow-up. Arch Intern Med 2004;164(13):1422-6. 6. Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care 2005;28(9):2130-5. 7. Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010;376(9753):1670-81. 8. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364(9435):685-96. 9. Collins R, Armitage J, Parish S, Sleigh P, Peto R. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003;361(9374):2005-16. 10. Leiter LA, Lundman P, da Silva PM, Drexel H, Junger C, Gitt AK. Persistent lipid abnormalities in statin-treated patients with diabetes mellitus in Europe and Canada: results of the Dyslipidaemia International Study. Diabet Med 2011;28(11):1343-51. 11. Rees K, Dyakova M, Ward K, Thorogood M, Brunner E. Dietary advice for reducing cardiovascular risk. Cochrane Database Syst Rev 2013;3:CD002128. 12. Davidson MH, Clark JA, Glass LM, Kanumalla A. Statin safety: an appraisal from the adverse event reporting system. Am J Cardiol 2006;97(8A):32C-43C. 13. Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients–the PRIMO study. Cardiovasc Drugs Ther 2005;19(6):403-14. 14. The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251(3):351-64. 15. AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011;365:2255-67 16. HPS2-THRIVE Collaborative Group. HSP2-THRIVE randomized placebo-controlled trial in 25,673 high-risk patients of ER niacin/laropiprant: trial design, pre-specified muscle and liver outcomes, and reasons for stopping study treatment. Eur Heart J 2013;34:1279-91 17. ACCORD Study Group. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med 2010;362:1563-74 18. Baigent C, Landray MJ, Reith C, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet 2011;377(9784):2181-92. 19. Corsini A, Windler E, Farnier M. Colesevelam hydrochloride: usefulness of a specifically engineered bile acid sequestrant for lowering LDL-cholesterol. Eur J Cardiovasc Prev Rehabil 2009;16(1):1-9. 20. Hunninghake D, Insull W, Jr., Toth P, Davidson D, Donovan JM, Burke SK. Coadministration of colesevelam hydrochloride with atorvastatin lowers LDL cholesterol additively. Atherosclerosis 2001;158(2):407-16. 21. Bays HE, Goldberg RB, Truitt KE, Jones MR. Colesevelam hydrochloride therapy in patients with type 2 diabetes mellitus treated with metformin: glucose and lipid effects. Arch Intern Med 2008;168(18):1975-83. 22. Fonseca VA, Rosenstock J, Wang AC, Truitt KE, Jones MR. Colesevelam HCl improves glycemic control and reduces LDL cholesterol in patients with inadequately controlled type 2 diabetes on sulfonylurea-based therapy. Diabetes Care 2008;31(8):1479-84. 23. Goldberg RB, Fonseca VA, Truitt KE, Jones MR. Efficacy and safety of colesevelam in patients with type 2 diabetes mellitus and inadequate glycemic control receiving insulin-based therapy. Arch Intern Med 2008;168(14):1531-40. 24. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010;375(9716):735-42. 25. Bell DS, O’Keefe JH. Rediscovering bile acid sequestrants. Diabetes Obes Metab 2009;11(12):1114-21. 26. Staels B, Kuipers F. Bile acid sequestrants and the treatment of type 2 diabetes mellitus. Drugs 2007;67(10):1383-92. 27. Bays H, Jones PH. Colesevelam hydrochloride: reducing atherosclerotic coronary heart disease risk factors. Vasc Health Risk Manag 2007;3(5):733-42. 28. Bays HE, Goldberg RB. The ‘forgotten’ bile acid sequestrants: is now a good time to remember? Am J Ther 2007;14(6):567-80. 29. Davis TM, Ting R, Best JD, et al. Effects of fenofibrate on renal function in patients with type 2 diabetes mellitus: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study. Diabetologia 2011;54(2):280-90. 30. Chew EY, Ambrosius WT, Davis MD, et al. Effects of medical therapies on retinopathy progression in type 2 diabetes. N Engl J Med 2010;363(3):233-44. 31. Vakkilainen J, Steiner G, Ansquer JC, Perttunen-Nio H, Taskinen MR. Fenofibrate lowers plasma triglycerides and increases LDL particle diameter in subjects with type 2 diabetes. Diabetes Care 2002;25(3):627-8. 32. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult – 2009 recommendations. Can J Cardiol 2009;25(10):567-79. 33. Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med 2010;362(17):1563-74.
Bringing Patients with Type 2 Diabetes to LDL-C Goals
Reiterated in the 2013 Canadian Diabetes Association (CDA) guidelines, the primary goal for low-density lipoprotein cholesterol (LDL-C) in patients with type 2 diabetes mellitus (T2DM) is ≤2.0 mmol/L.(1) Even though LDL-C levels are often only modestly elevated in T2DM patients,(2) the same strict LDL-C target applies as in other high-risk patients without T2DM, including those who have had a previous cardiovascular event.(3) In patients with T2DM, the first-line therapy for reaching LDL-C goals is typically an HMG CoA reductase inhibitor (statin). The second-line agents, used adjunctively, or in the case of intolerance, as a substitutefor statins, are listed in the CDA guidelines alphabetically as bile acid sequestrants, a cholesterol absorption inhibitor, fibrates and nicotinic acid formulations. Each second-line drug has its own particular benefits and shortcomings. The second-line lipid-modifying agents may help patients with T2DM reach LDL-C targets, but their use should be individualized based on the anticipated benefit derived from their specific therapeutic profiles.
Show review