Expert Review
Urinary Tract Infections: Expert Review and Commentary from Published Literature
Reducing UTIs Associated with Urethral Procedures: Concepts and Strategies
Jun Kawakami, MD, FRCSC
Southern Alberta Institute of Urology, Calgary, Alberta
Urinary tract infections (UTIs) are a common iatrogenic complication of diagnostic and therapeutic procedures involving urethral manipulation, such as catheterization or cystoscopy. Due to the potential for UTIs to incur additional healthcare costs, adversely affect outcome, and diminish patient satisfaction, steps to reduce risk are warranted in both males and females. Simple steps surrounding the performance of endourethral procedures, such as employing antimicrobial prophylaxis and minimizing injury and trauma to the urethral endothelium through lubricants and anaesthesia, offer opportunities to reduce the risk of infection over that provided by standard infection control practice alone. Many of these steps are well known but applied inconsistently. In performing diagnostic or therapeutic procedures involving the urethra, rigorously implemented UTI risk reduction assures high standards of quality of care.
Background
In Canada and elsewhere, urinary tract infections (UTIs) are recognized as the single most common infection acquired in the course of healthcare.1 In studies conducted in the United States, UTIs represent 40% of nosocomial infections.2 Although most healthcare-associated UTIs are asymptomatic,3 particularly those acquired in an acute care facility, these pose an important risk of significant complications, including urethral inflammation, strictures, and urolithiasis.4 Infection can affect tissue in any part of the urinary tract, including the bladder and kidneys, requiring prolonged and costly courses of antibiotics.5 Approximately 20% of potentially fatal nosocomial bacteremias arise from a UTI.6
Although most healthcare-associated UTIs are asymptomatic, these pose an important risk of significant complications, including urethral inflammation, strictures, and urolithiasis.
More urgent and comprehensive strategies to avoid UTIs should be considered a priority. Due to the frequency of asymptomatic UTIs and the risk of invasive pathogens and extensive involvement when diagnosis is delayed, effective methods of prophylaxis represent the best opportunity to reduce complications, costs, and patient discomfort. When performing a procedure involving urethra, there are two keys steps: infection control and minimizing injury and trauma to the vulnerable urethral epithelium. Of procedures capable of precipitating healthcare-associated UTIs, urethral catheterization is the most commonly performed and implicated. These devices, commonly called Foley catheters, which pass through the urethra to drain the bladder, are employed in up to 25% of patients at some point during an acute hospitalization.7 In one recent survey of 183 acute care hospitals, the rate of hospital-acquired infections in catheterized patients was nearly double that of patients without a device (39.2% vs. 22.9%; P<0.001).8 The risk of catheter-associated (CA) bacteriuria is time related with an estimated incidence ranging from 3% to 9% per day.9,10 UTIs also appear more likely to involve the bladder, kidney, or other structures when prolonged. In an autopsy study conducted among patients who died in a long-term care facility, the prevalence of chronic pyelonephritis was 10% among those catheterized for >90 days and 0% for those catheterized <90 days in the last year of their life (P=0.02).11 The morbidity from a healthcare-related UTI induces a high cost. In acute care facilities, the increase in average length of stay for community acquired UTI (CA-UTI) ranges from 0.4 days in asymptomatic patients to 2 days in those with symptoms.12 Due to the frequency of this complication, these prolonged stays impose a substantial increase in the cost of management.13 The increased cost of care is accompanied by a diminished quality of life in those who develop symptoms.14 Nosocomial UTIs produced by other procedures involving the urethra are likely to impose similar morbidity, providing a rationale for developing formal strategies to reduce UTI risk from any cause.
Mechanism
Even in otherwise healthy individuals, UTIs are common when the balance of resident microorganisms important to preventing infection is lost.15 As a result, the substantial risks of infection from procedures that involve manipulation of the urethra are not surprising. Although the healthy urinary tract is normally sterile,16 the epithelium of the urethral lumen is highly vulnerable to injury, setting the stage for pathogen adherence and invasion. Moreover, vulnerability to infection from urethral manipulation is exacerbated by the proximity of the urethral orifice to perianal and perivaginal colonies of microorganisms.17 In those seeking healthcare, this vulnerability may be further exacerbated by a diminished immune response secondary to the underlying illness. Healthcare-acquired UTIs are uncommon in the absence of invasive procedures that involve the urethra, providing a focus for efforts to reduce this complication. The mechanisms of these infections, and therefore the opportunities for prevention, are straightforward. Resident bacteria on the skin and within the urethral lumen have the potential to be disturbed by invasive procedures, and the risk of devices carrying an inoculum of bacteria into the urethral lumen is underscored by the pathogens typically isolated. Consistent with the ability of otherwise benign bacteria to become invasive when placed in environments where natural mechanisms of inhibition are lost,18 approximately two thirds of bacteria associated with CA-UTIs can be traced to an extraluminal origin.19
Invasive procedures have the potential to disrupt the otherwise highly effective innate immune defenses at work in the urinary tract.
Furthermore, invasive procedures have the potential to disrupt the otherwise highly effective innate immune defenses at work in the urinary tract. These defenses serve to prevent bacteria and other microorganisms from the initial steps of infection, such as adherence to epithelial cells, through expression of antimicrobial chemokines and upregulation of phagocytes. 20 When devices irritate the epithelium, the transition to an adaptive immune response, which features upregulation of inflammatory signaling, may be better suited to responding to an existing infection than preventing an infection from occurring. Due to these factors, any diagnostic or therapeutic procedure that involves penetration of the urethra incurs a potential infection risk. This includes insertion of cystoscopes, catheters, or other devices employed in the evaluation or treatment of conditions involving the urinary tract. For indwelling catheters, the risks are multiplied. Initially and over time, the catheter entry point at the urethral meatus provides a route for migration of pathogens into the urethra.21 In addition, biofilm that develops on catheters provides a medium for growth.22 Biofilm, which inhibits the effect of antimicrobial agents,23 also fosters resistant infections due to the ability of colonizing bacteria to effectively communicate genetic information during localized growth.24 These differences in the patterns of contamination and growth explain why CA-UTI pathogens associated with biofilm are often more virulent than those isolated from UTIs stemming from other sources. These mechanisms provide clear targets for prevention. In addition to sterile technique, the urethral epithelium must be protected from injury and stress. One step is to use lubricants to reduce friction as catheters, cystoscopes, or other instruments are inserted. Another is to provide anesthesia to reduce pain responses and stimulation of inflammatory mediators. The goal is not only to prevent bacteria from entering the urethral lumen but reducing the risk of adherence essential for infection when sterile technique is imperfect.
Steps to Lower Risk
The best strategy for avoiding healthcare-related UTI stemming from procedures involving the urethra is to reduce the number of procedures performed. Strategies include non-invasive diagnostic evaluations, such as ultrasound, and avoiding urethral catheterization when other means of voiding are feasible. Several studies have provided evidence that urethral catheterization is employed excessively, particularly among the elderly.25, 26, 27 Initiatives to limit these procedures have been advocated in order to reduce morbidity and healthcare costs,28 even though a survey of hospitals in the United States suggests that few acute care facilities have implemented active programs.29 When invasive procedures are unavoidable, the formal strategies recommended for reducing risk of CA-UTIs, such as employing narrow indications, current Infectious Diseases Society of America (IDSA) guidelines recommend establishing protocols for sterile technique and outlining when and how antimicrobial prophylaxis should be applied.13 The importance of rigorous application of well-established infection control practices, such as hand washing, respiratory hygiene, and environmental cleanliness, cannot be over emphasized. The ability of evidence-based infection control practices to reduce nosocomial infection risk, including risk of UTI, is well documented.30 For specifically preventing healthcare-associated UTI stemming from urethral manipulation beyond routine infection control strategies, two factors deserve attention. The first is providing antisepsis in the urethra. The other is avoiding irritation to the urethral epithelium. Although inflammation is a common consequence of infection, urethritis may also lower the innate epithelial defenses against adhesion of bacteria required for colonization and invasion. Pain control may also be important. Although pain arises from inflammation, there is at least experimental evidence to suggest that pain signaling upregulates prostaglandins and other mediators of the inflammatory response,31 which may increase susceptibility of the urethral epithelium to bacterial adhesion and invasion.
Antisepsis, lubrication, and pain control provide the pillars of UTI prevention when performing invasive procedures involving the uretha.
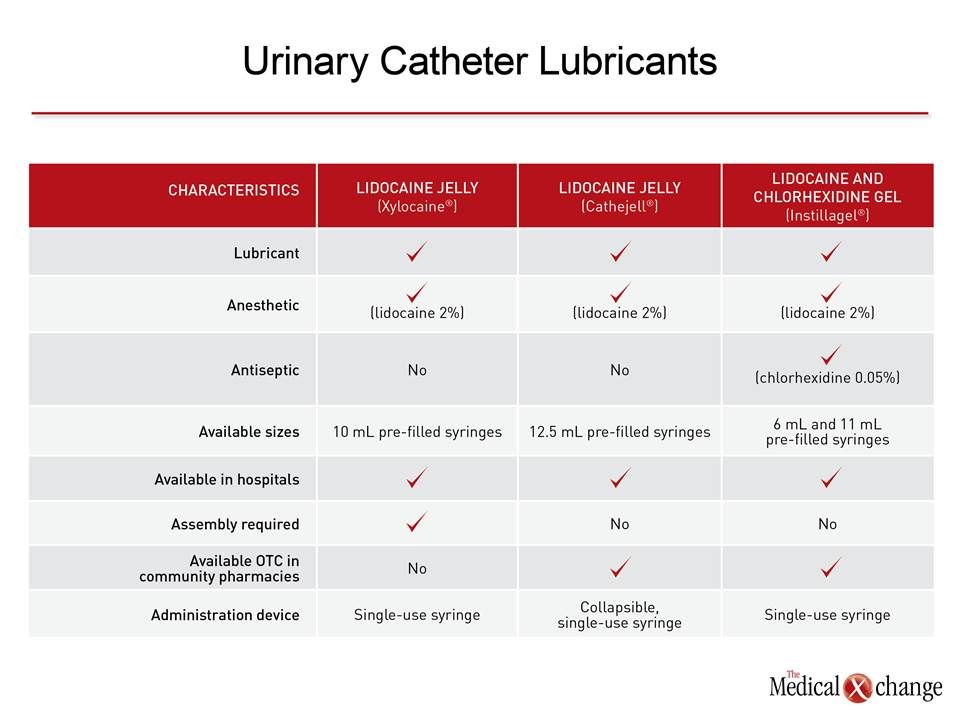
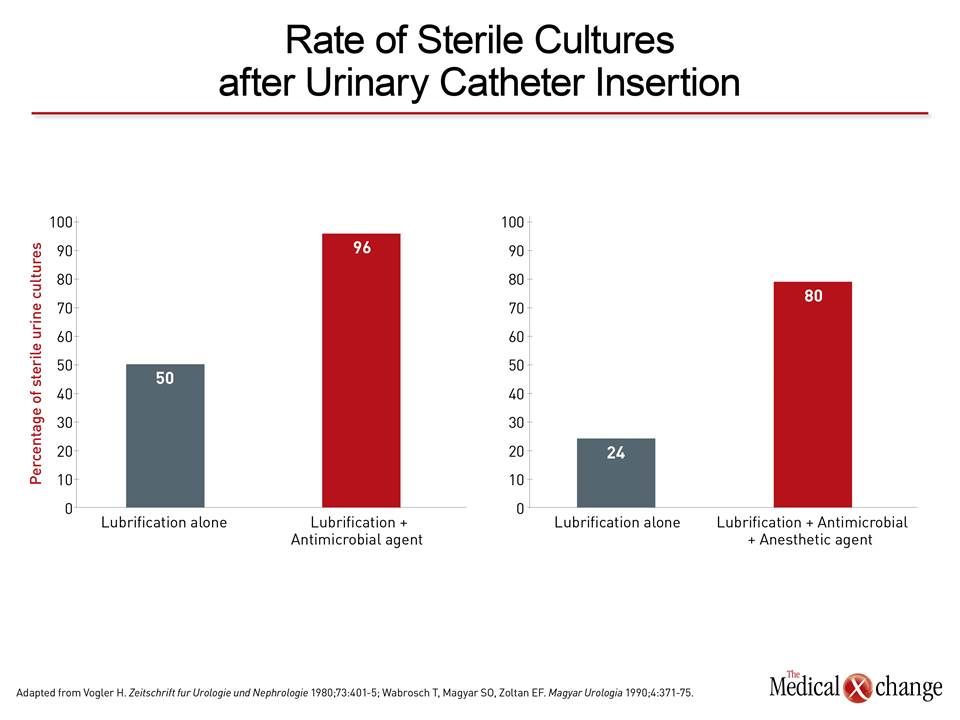
Antisepsis, lubrication, and pain control provide the pillars of UTI prevention when performing invasive procedures involving the urethra. In guidelines from the IDSA for prevention of CA-UTIs, antimicrobial-coated catheters are identified as a potential strategy and systemic antimicrobials are recommended specifically.13 In addition, insertion with aseptic technique and sterile equipment is also a specific IDSA recommendation. The additional value of lubrication and pain control when inserting catheters or other endourethral devices is supported by an extensive literature developed over more than 20 years. Many studies were performed with a product that combines lidocaine as an analgesic and chlorhexidine as an antiseptic. Lubricating ingredients such as propylene glycol have been added to reduce risk of epithelial damage from device insertion (Table 1). The published clinical studies with this combination lidocaine and chlorhexidine agent, which is indicated for surface anesthesia, lubrication, and antisepsis for females and males undergoing cystoscopy, catheter insertion, and other endourethral procedures, employ a variety of efficacy and safety endpoints but include reductions in rate of UTIs. In a study of 149 females undergoing catheter insertion after major gynecologic surgery, the rate of UTI was reduced by 32% in those whose insertion was performed with the combination agent relative to those who were not (20% vs. 13.5%; P<0.05).32 Consistent with other studies performed with this agent, no significant adverse events were reported. In a study comparing the lidocaine and chlorhexidine combination agent to liquid paraffin among 320 patients undergoing catheter insertion (135 patients) or cystoscopy (185 patients), the rate of sterile urine cultures was nearly four times higher in the catheter group (80% vs. 24%) and approximately 2 times higher in the cystoscopy group (63% vs. 36%) among those who received the combination agent.33 Moreover, pain was reported in those patients undergoing cystoscopy who received liquid paraffin but not in those who received the lidocaine and chlorhexidine agent. In another cystoscopy study of 175 patients comparing the combination agent to two other types of gels without antiseptic activity, sterile urethral smears were obtained in 96% of those receiving the combination product versus 50% or fewer with the alternative gels (Fig. 1).34 Similar results were observed in a comparison of the combination agent to xylocaine.35 In addition to yielding data confirming safety,36 published studies have also associated it with relief of pain.37 In one study, the lubricating effect was shown to prevent microlesions in the urethra,38 a potential mechanism for reducing the risk of both urethritis and UTI. This literature provides support for the value of a comprehensive approach to endourethral procedures that combines sterile technique with antisepsis, analgesia, and lubrication. When combined, each has the potential to achieve an incremental reduction in risk of UTI by addressing the independent but interrelated risks that increase susceptibility to infection. The additional clinical value of pain prevention and improved ease of inserting devices into the urethra cannot be discounted. This step in care is broadly applicable for any healthcare-related procedure involving penetration of the urethra, including self-catheterization performed by patients outside of the hospital setting. The value of antisepsis, analgesia, and lubrication should be considered in the context of other recommended steps in UTI prophylaxis.
Conclusion
Due to an exceptional representation among nosocomial infections, UTIs are regarded as an important focus of infection control strategies designed to reduce healthcare-related morbidity and costs. A large proportion of nosocomial UTIs are attributed to penetration of the urethra for diagnostic or therapeutic procedures. A comprehensive and multifaceted approach to UTI prophylaxis in these individuals requires consideration of steps beyond rigorous application of sterile technique. This includes steps to reduce injury to the urethral epithelium in order to sustain its integrity. In the context of other methods of UTI prophylaxis, there is evidence to support an approach that combines antisepsis with pain control and lubrication.
References
1. Nicolle LE. The prevention of hospital-acquired urinary tract infection. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2008;46:251-3. 2. National Nosocomial Infections Surveillance S. National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. American journal of infection control 2004;32:470-85. 3. Tambyah PA, Maki DG. Catheter-associated urinary tract infection is rarely symptomatic: a prospective study of 1,497 catheterized patients. Archives of internal medicine 2000;160:678-82. 4. Nicolle LE. Urinary catheter-associated infections. Infectious disease clinics of North America 2012;26:13-27. 5. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2011;52:e103-20. 6. Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA, Healthcare Infection Control Practices Advisory C. Guideline for prevention of catheter-associated urinary tract infections 2009. Infection control and hospital epidemiology : the official journal of the Society of Hospital Epidemiologists of America 2010;31:319-26. 7. Saint S, Wiese J, Amory JK, et al. Are physicians aware of which of their patients have indwelling urinary catheters? The American journal of medicine 2000;109:476-80. 8. Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of health care-associated infections. The New England journal of medicine 2014;370:1198-208. 9. Hartstein AI, Garber SB, Ward TT, Jones SR, Morthland VH. Nosocomial urinary tract infection: a prospective evaluation of 108 catheterized patients. Infection control : IC 1981;2:380-6. 10. Warren JW, Damron D, Tenney JH, Hoopes JM, Deforge B, Muncie HL, Jr. Fever, bacteremia, and death as complications of bacteriuria in women with long-term urethral catheters. The Journal of infectious diseases 1987;155:1151-8. 11. Warren JW, Muncie HL, Jr., Hebel JR, Hall-Craggs M. Long-term urethral catheterization increases risk of chronic pyelonephritis and renal inflammation. Journal of the American Geriatrics Society 1994;42:1286-90. 12. Haley RW, Schaberg DR, Crossley KB, Von Allmen SD, McGowan JE, Jr. Extra charges and prolongation of stay attributable to nosocomial infections: a prospective interhospital comparison. The American journal of medicine 1981;70:51-8. 13. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2010;50:625-63. 14. Ellis AK, Verma S. Quality of life in women with urinary tract infections: is benign disease a misnomer? The Journal of the American Board of Family Practice / American Board of Family Practice 2000;13:392-7. 15. Schaeffer AJ. What do we know about the urinary tract infection-prone individual? The Journal of infectious diseases 2001;183 Suppl 1:S66-9. 16. Ali AS, Townes CL, Hall J, Pickard RS. Maintaining a sterile urinary tract: the role of antimicrobial peptides. The Journal of urology 2009;182:21-8. 17. Daifuku R, Stamm WE. Association of rectal and urethral colonization with urinary tract infection in patients with indwelling catheters. Jama 1984;252:2028-30. 18. Cohen A. A microbiological comparison of a povidone-iodine lubricating gel and a control as catheter lubricants. The Journal of hospital infection 1985;6 Suppl A:155-61. 19. Tambyah PA, Halvorson KT, Maki DG. A prospective study of pathogenesis of catheter-associated urinary tract infections. Mayo Clinic proceedings 1999;74:131-6. 20. Zasloff M. Antimicrobial peptides, innate immunity, and the normally sterile urinary tract. Journal of the American Society of Nephrology : JASN 2007;18:2810-6. 21. Warren JW. Catheter-associated urinary tract infections. International journal of antimicrobial agents 2001;17:299-303. 22. Morris NS, Stickler DJ, McLean RJ. The development of bacterial biofilms on indwelling urethral catheters. World journal of urology 1999;17:345-50. 23. Donlan RM. Role of biofilms in antimicrobial resistance. ASAIO journal 2000;46:S47-52. 24. Saye DE. Recurring and antimicrobial-resistant infections:considering the potential role of biofilms in clinical practice. Ostomy/wound management 2007;53:46-8, 50, 2 passim. 25. Gokula RR, Hickner JA, Smith MA. Inappropriate use of urinary catheters in elderly patients at a midwestern community teaching hospital. American journal of infection control 2004;32:196-9. 26. Fakih MG, Shemes SP, Pena ME, et al. Urinary catheters in the emergency department: very elderly women are at high risk for unnecessary utilization. American journal of infection control 2010;38:683-8. 27. Jain P, Parada JP, David A, Smith LG. Overuse of the indwelling urinary tract catheter in hospitalized medical patients. Archives of internal medicine 1995;155:1425-9. 28. Cardo D, Dennehy PH, Halverson P, et al. Moving toward elimination of healthcare-associated infections: a call to action. American journal of infection control 2010;38:671-5. 29. Saint S, Kowalski CP, Kaufman SR, et al. Preventing hospital-acquired urinary tract infection in the United States: a national study. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2008;46:243-50. 30. Sehulster L, Chinn RY, Cdc, Hicpac. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recommendations and reports : Morbidity and mortality weekly report Recommendations and reports / Centers for Disease Control 2003;52:1-42. 31. Trebino CE, Stock JL, Gibbons CP, et al. Impaired inflammatory and pain responses in mice lacking an inducible prostaglandin E synthase. Proceedings of the National Academy of Sciences of the United States of America 2003;100:9044-9. 32. Kambal C, Chance J, Cope S, Beck J. Catheter-associated UTIs in patients after major gynaecological surgery. Professional nurse 2004;19:515-8. 33. Wabrosch T, Magyar SO, Zoltan EF. Efficacy of Instillagel versus liquid paraffin for endourethral procedures. Magyar Urologia 1990;4:371-75. 34. Vogler H. [Study of the disinfectant action of lubricants in transurethral electroresection]. Zeitschrift fur Urologie und Nephrologie 1980;73:401-5. 35. Wassman BO, Kutzbergermann F, Hoitler A. Lubrication and antisepsis versus analgesia alone in patients undergoing cystoscopy. Urologe B 1988;28:367-9. 36. Brekkan E, Ehrnebo M, Malmstrom PU, Norlen BJ, Wirbrant A. A controlled study of low and high volume anesthetic jelly as a lubricant and pain reliever during cystoscopy. The Journal of urology 1991;146:24-7. 37. Thompson TJ, Thompson N, O’Brien A, Young MR, McCleane G. To determine whether the temperature of 2% lignocaine gel affects the initial discomfort which may be associated with its instillation into the male urethra. BJU international 1999;84:1035-7. 38. Gunther J. [The use of a disposable anesthetic lubricant (Instillagel) in catheterization of the urethra (author’s transl)]. MMW, Munchener medizinische Wochenschrift 1974;116:959-60.
Reducing UTIs Associated with Urethral Procedures: Concepts and Strategies
Urinary tract infections (UTIs) are a common iatrogenic complication of diagnostic and therapeutic procedures involving urethral manipulation, such as catheterization or cystoscopy. Due to the potential for UTIs to incur additional healthcare costs, adversely affect outcome, and diminish patient satisfaction, steps to reduce risk are warranted in both males and females. Simple steps surrounding the performance of endourethral procedures, such as employing antimicrobial prophylaxis and minimizing injury and trauma to the urethral endothelium through lubricants and anaesthesia, offer opportunities to reduce the risk of infection over that provided by standard infection control practice alone. Many of these steps are well known but applied inconsistently. In performing diagnostic or therapeutic procedures involving the urethra, rigorously implemented UTI risk reduction assures high standards of quality of care.
Show review