Expert Review
United European Gastroenterology Week (UEGW) 2014: Expert Review
Patient Confidence in Biologic IBD Therapies Identified as a Factor in Long-Term Disease Control
John Marshall, MD MSc FRCPC AGAF
Professor of Medicine McMaster University
Member, Farncombe Family Digestive Health Research Institute
Chief of Clinical Service for Gastroenterology, Hamilton Health Sciences, Hamilton, Ontario
Vienna – Biologics, such as tumour necrosis factor inhibitors (TNFi), offer an unprecedented level of efficacy in patients with moderate to severe inflammatory bowel disease (IBD), but relative benefit in the individual patient is difficult to predict. Patient confidence in the choice of biologic appears to be a factor. Several sets of data presented at UEGW, including one looking specifically at patient acceptance of biologic treatment, suggest that patient perception of efficacy and safety has independent influence on disease control. In IBD, it has been proposed that a high rate of satisfaction with treatment leads to closer adherence, which, in turn, increases exposure to active therapy to improve the likelihood of sustained remissions. On this basis, it appears that differences among biologics, such as route of administration, have meaningful influences on long-term IBD benefit.
The proliferation of biologics for the treatment of Crohn’s disease (CD) and ulcerative colitis (UC), as well as other inflammatory diseases such as rheumatoid arthritis and plaque psoriasis, has provided patients and clinicians with an array of valuable options. Patients who have a poor initial response or lose response to one biologic often respond to an alternative. In addition, biologics differ in their formulation, which affect options for administration and patient satisfaction.
PATIENT CONFIDENCE AND ADHERENCE
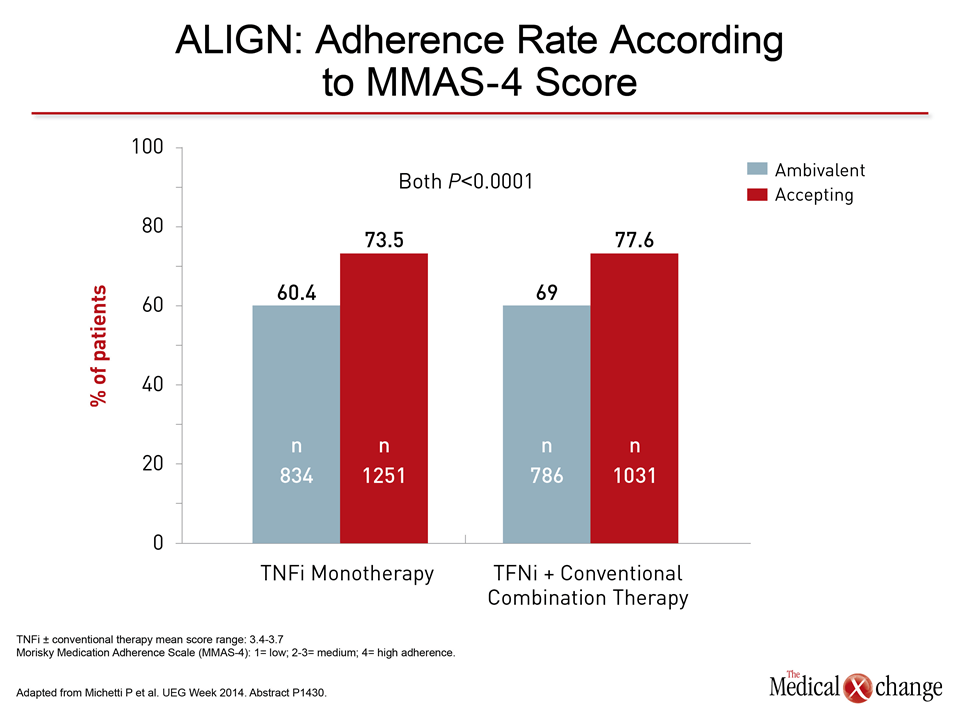
On the premise that patient satisfaction may affect adherence to biologics—a potential influence on efficacy and rates of remission— a study presented by Michetti P. et al. at this year’s UEGW evaluated the correlation between patient attitudes about biologics and adherence (Abstract P1430). In considering biologics with different characteristics that are now available for treatment of inflammatory bowel disease (IBD), the data provided evidence that the relative role of adherence as an influence on long-term outcome may be underappreciated.
In considering biologics with different characteristics that are now available for treatment of inflammatory bowel disease (IBD), the data provided evidence that the relative role of adherence as an influence on long-term outcome may be underappreciated.
In this multinational study, entitled ALIGN (n=7,197), patient level of treatment acceptance was measured with the Beliefs about Medicine Questionnaire (BMQ). The BMQ categorized patients as ambivalent or accepting of treatment. Adherence was measured with the Morisky Medication Adherence Scale (MMAS), which stratified patients into four categories, with level 4 (MMAS-4) signifying the highest level of adherence. Patients with a variety of inflammatory diseases in addition to IBD, including psoriatic arthritis and ankylosing spondylitis, were included. Adherence was evaluated both in those on tumour necrosis factor inhibitor (TNFi) monotherapy and TNFi in combination with a conventional agent, such as an immunosuppressant or steroids. A significantly larger proportion of patients achieved MMAS-4 who scored “acceptance” on BMQ relative to those “ambivalent” about their biologic whether it was taken as a monotherapy (73.5% vs. 60.4%; P<0.0001) or in a combination (77.6% vs. 69%; P<0.0001) (Fig. 1).
Route Administration: Not all Biologics are Interchangeable
The specific features of biologics that conferred an accepting or an ambivalent attitude were not evaluated in this study, but these agents are not interchangeable. Among TNFi agents, which are widely considered the first-line biologic in moderate to severe inflammatory bowel disease (IBD), route of administration is one of most significant distinguishing features from the patient perspective. The first of this class, infliximab, is delivered by intravenous (IV) infusion in weight-based dosing at an ambulatory infusion centre. Newer agents such as adalimumab, certolizumab, golimumab and etanercept are delivered subcutaneously (SC) and may be self-injected. Etanercept is administered twice weekly, while the fully humanized adalimumab and golimumab can be administered every two and four weeks, respectively.
Rates of Biologic Adherence May Vary in Both Adult and Pediatric Populations
However, ease of administration is not the only characteristic that distinguishes biologics. Patient confidence in treatment may be driven by a large variety of other influences, including patient perception of benefit or risk.
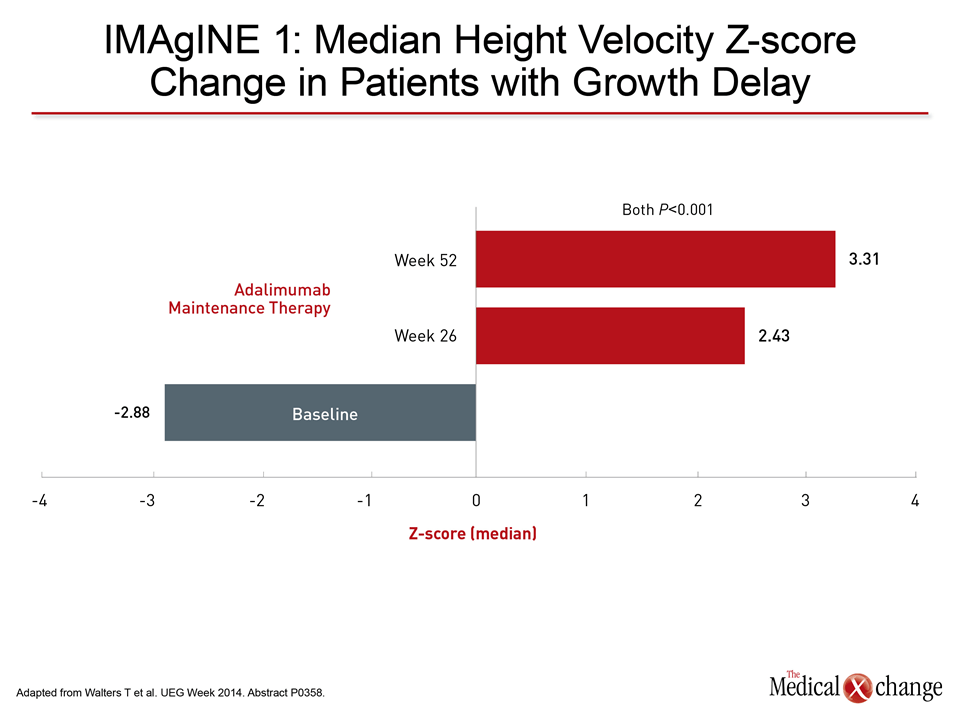
However, ease of administration is not the only characteristic that distinguishes biologics. Patient confidence in treatment may be driven by a large variety of other influences, including patient perception of benefit or risk. To the degree that these perceptions affect adherence, they may, in turn, influence the likelihood of achieving complete remission. Although well-controlled, head-to-head comparisons of biologics have yet to be conducted; other data have suggested that rates of adherence are not necessarily similar between available agents. In a systematic review of 13 studies published last year (Lopez A. et al. Inflamm Bowel Dis 2013;19:1528-33), the data suggested variable biologic adherence rates even though overall rates were high. In the pooled analysis from non-comparative studies using several measures of persistence with medication, including MMAS, acceptable adherence was achieved in 83.1% of those taking adalimumab and 70.7% of those on infliximab. The premise of perceived benefit and risk is as relevant in a pediatric population as it is in adults. In children, the relative differences in efficacy and safety between TNFi agents or between TNFis and other biologics also remain untested with large, randomized and blinded trials, but data from single agent trials do generate varying sets of data that may be relevant to confidence in therapy and subsequent adherence. In the pediatric population, one of the most significant findings regarding biologics presented at the UEGW was evidence of improved growth velocity when adalimumab was administered in those children who had previously exhibited growth delay (Abstract P358). In this study by Walters T. et al, the improvement in growth velocity after initiating adalimumab was most pronounced in those children taking concomitant corticosteroids at baseline as well as in those with severe disease. Such evidence may be compelling to parents weighing the value of biologics in a child. The data presented here represented a substudy analysis from the previously-published IMAgINE 1 trial (Hyams JS et al. Gastroenterol 2012;143:365-74). Change in growth velocity was evaluated after 26 and 52 weeks in patients stratified by high and low doses of adalimumab, previous exposure to infliximab, use of corticosteroids and CD severity. In these groups, the baseline growth delay as calculated with velocity Z scores averaged -2.9 (Fig. 2).
The improvement in growth velocity after initiating adalimumab was consistent across all stratifications, although the degree of improvement was substantially less in children who had previously received infliximab than in those who had not.
The improvement in growth velocity after initiating adalimumab was consistent across all stratifications, although the degree of improvement was substantially less in children who had previously received infliximab than in those who had not. No change in growth velocity was observed in children without growth delay at baseline, but relative growth improvement on adalimumab was greater in those children on corticosteroids at baseline, those with greatest relative disease severity, and those who were naive to previous biologic exposure.
Exploring Transmural Healing
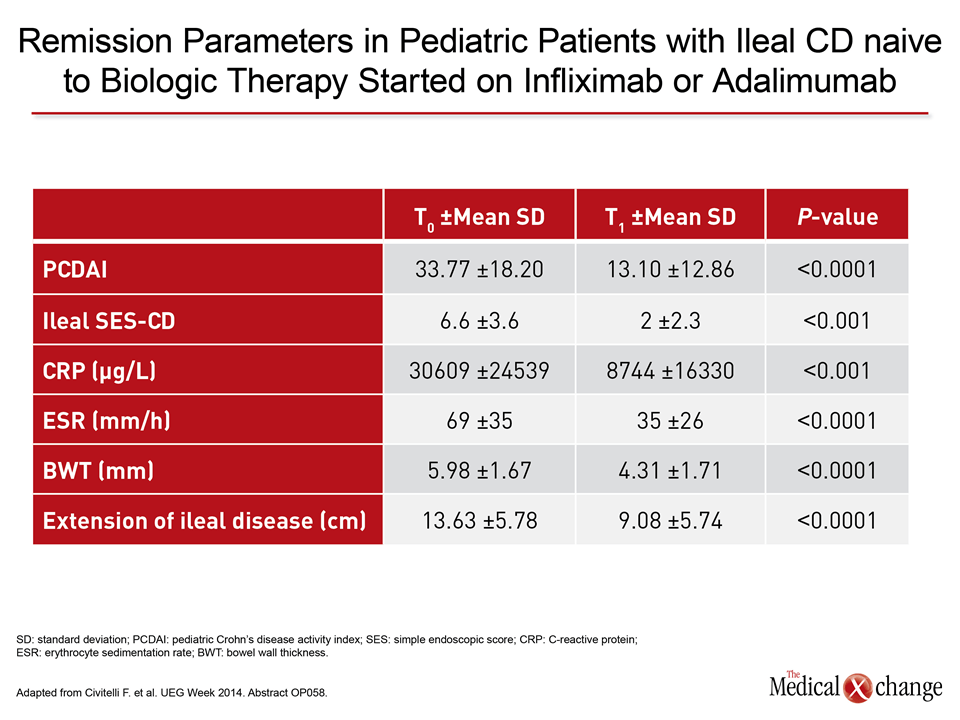
In another pediatric study presented at UEGW, the goal was to further explore the meaning and definition of deep remissions, an end point that builds on the concept of mucosal healing (Abstract OP58). While there is a growing amount of data that suggest complete mucosal healing provides a greater barrier to relapse than partial remission, this study by Civitelli F. et al. evaluated changes in transmural healing (TH), an even more rigorous treatment goal. In this study of 26 pediatric CD patients naive to biologics, small intestine contrast ultrasonography (SICUS) was employed to objectively measure bowel wall parameters in order to evaluate the effect of 9 to 12 months of treatment with adalimumab or infliximab (Table 1). The evidence of transmural involvement in IBD makes such measures potentially relevant to extending the definition of a deep remission.
The evidence of transmural involvement in IBD makes such measures potentially relevant to extending the definition of a deep remission.
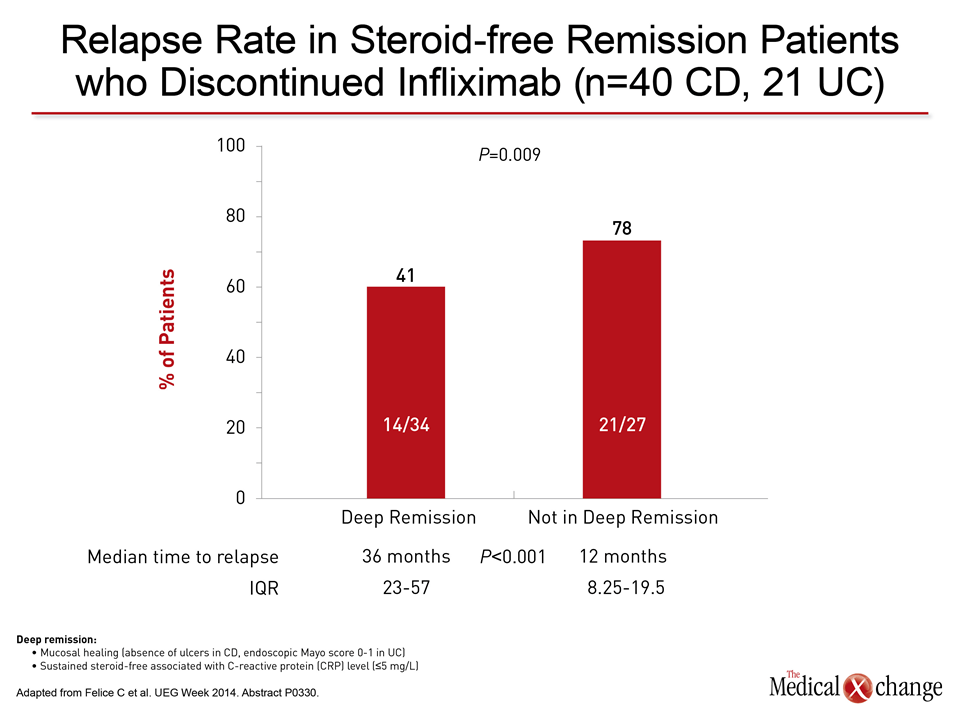
Relative to those who did not achieve a complete remission, responders achieved significantly greater improvement (P<0.02) in multiple SICUS measures of transmural disease, including bowel wall thickness and vascularity. The study led the authors to conclude that early control may be important, because the impact of biologics on these measures was substantially less in those with baseline bowel damage, such as stricture. (Table 1) Further studies are needed to confirm that these measures of deep remission provide an incremental gain over mucosal healing for major outcomes, such as freedom from relapse, but such an advantage would be expected from a growing number of studies suggesting that deep remissions have prognostic importance. Another study at UEGW exploring the prognostic advantage for complete and deep remissions evaluated sustained response after biologic discontinuation (Abstract P330). This study, presented by Felice C. et al, included 34 patients who had achieved deep remission and 27 patients who had not at the time that infliximab was discontinued. Deep remission was defined as mucosal healing, normalization of C-reactive protein (CRP) levels (≤5 mg/L), and absence of symptoms off steroids.
Deep Remission Predicts Relapse
Time to relapse was also significantly shorter in the group that had not achieved deep remission.
After a median follow-up of 36 months following biologic discontinuation, the relapse was 41% among those who met the definition of deep remission vs. 78% among those who had not (Fig. 3). Time to relapse was also significantly shorter in the group that had not achieved deep remission. The data overall suggest that IBD patients who achieve a steroid-free remission on a biologic and then discontinue therapy have a substantial risk of relapse. However, the presence of a deep remission at the time that the biologic is discontinued appears to correspond with a longer period of remission.
Use of Sonography as a Non-invasive Option to Monitor Disease Activity
The value of closely monitoring mucosal healing has led to new proposals on how to follow IBD patients to ensure clinical response. In data presented at UEGW from an ongoing study of 50 patients on adalimumab, disease activity at 4 months correlated well with mucosal healing at 12 months (Abstract P865). In this study by Novak K. et al., the goal was to use sonography to monitor disease activity and response to adalimumab with endoscopy employed as a gold standard to evaluate predictive accuracy.
The presence of a deep remission at the time that the biologic is discontinues appears to correspond with a longer period of remission.
At baseline, agreement between sonography and endoscopy in an initial 30 patients was characterized as excellent with complete agreement in 26 of the 30. Sonography was performed again at 4 months and results were compared to endoscopy performed a second time at 12 months. Active disease on sonography at 4 months could be seen in all of those with active disease at the 12-month endoscopic evaluation. The data are preliminary, but the authors concluded that non-invasive sonography might prove to be a surrogate for endoscopy and a method of measuring treatment response. Non-invasive sonography might prove to be a surrogate for endoscopy and a method of measuring treatment response.The sonographic study was conducted in patients with CD, but the same principles apply to UC, where adverse outcomes also include steroid dependence, in addition to relapse. Biologics can be an essential tool for regaining disease control in these patients. In a study at the UEGW with 37 steroid-dependent UC patients with advanced disease, 40% placed on the biologic adalimumab were steroid-free at the end of 12 months and mucosal healing was achieved in 48% (Abstract P904). While the majority of patients in this study, presented by Barreiro de Acosta M. et al, received concomitant immunosuppressive drugs, the only factors associated with a significantly reduced likelihood of steroid-free remission were previous infliximab therapy and the need to intensify the adalimumab dose. According to the authors of this study, these data reinforce the value of biologics overall and adalimumab, specifically in UC patients with severe disease defined by steroid dependence.
Conclusion
Inflammatory bowel disease (IBD) is a disease of relapses and remissions with the potential for progressive severity. Biologics have been an important advance for achieving remission in those insufficiently controlled on previously-available treatment options. However, the relative advantage of biologics for long-term outcomes appears to be dependent on the degree of response with a current focus not only on complete mucosal healing but, increasingly, on even more rigorous measures of deep remission. Employing biologics that are both easy to administer and well accepted by patients may be among factors which influence the likelihood of the high rates of adherence required for optimal benefit.
Patient Confidence in Biologic IBD Therapies Identified as a Factor in Long-Term Disease Control
Vienna – Biologics, such as tumour necrosis factor inhibitors (TNFi), offer an unprecedented level of efficacy in patients with moderate to severe inflammatory bowel disease (IBD), but relative benefit in the individual patient is difficult to predict. Patient confidence in the choice of biologic appears to be a factor. Several sets of data presented at UEGW, including one looking specifically at patient acceptance of biologic treatment, suggest that patient perception of efficacy and safety has independent influence on disease control. In IBD, it has been proposed that a high rate of satisfaction with treatment leads to closer adherence, which, in turn, increases exposure to active therapy to improve the likelihood of sustained remissions. On this basis, it appears that differences among biologics, such as route of administration, have meaningful influences on long-term IBD benefit.
Show review