hypertension
American Society of Hypertension (ASH) 26th Annual Scientific Meeting and Exposition
Simplified Algorithm Emphasizing Single Pill Combinations Provides Improved Blood Pressure Control
New York – Due to the pill burdens imposed by the control of multiple modifiable cardiovascular (CV) risk factors, a single tablet containing more than one active agent has been a logical and widely used practical approach in the effort to improve outcomes. The effectiveness of combination pills for reaching hypertensive goals in patients being treated for multiple CV risk factors has been assumed but only recently tested. In a new study, patients were randomized to receive a simplified treatment algorithm that included a combination of a calcium channel blocker for hypertension and a statin for hyperlipidemia, or to receive guidelines-based management. At the end of six months, those randomized to a combined-pill strategy had a significantly greater reduction in systolic blood pressure, fulfilling expectations. The absolute advantage of a simplified single-pill strategy over usual care at six months was modest, but the cumulative effect in patients receiving chronic therapy is potentially large.
In patients who do not achieve blood pressure (BP) targets on a single antihypertensive agent, single fixed-dose pills containing two drugs with different mechanisms of action have been recommended by several guidelines, including those issued by the Canadian Hypertension Education Program (CHEP). In patients with both hypertension and hyperlipidemia, single fixed-dose pills containing both an antihypertensive drug and a statin are also appealing for their ability to simplify regimens. A new study that included a fixed dose combination of the calcium channel blocker (CCB) amlodipine and atorvastatin for lipid lowering has demonstrated that this approach is more effective for sustained control of systolic BP.
STITCH2: Benefits of Simplified Regimens
“These data confirm the value of simple algorithms emphasizing the use of single pill combinations for managing hypertension,” reported Dr. George K. Dresser, Associate Professor, Division of Clinical Pharmacology, University of Western Ontario, London. Presenting results of the second STITCH (Simplified Therapeutic Intervention to Control Hypertension and Hypercholesterolemia) trial at the 2011 ASH meeting, Dr. Dresser indicated that simplified regimens have long been attractive but understudied in patient populations with multiple risks modifiable with therapy.
“These data confirm the value of simple algorithms emphasizing the use of single pill combinations for managing hypertension.”
In STITCH2, 35 primary care practices in Ontario were recruited. Each was permitted to enrol up to 50 patients. Enrolled patients were required to have both hypertension and hyperlipidemia, at least one of which was uncontrolled. These were defined as a systolic BP >140 mm Hg, a diastolic BP >90 mm Hg or hyperlipidemia above goal as defined by the third ATP (Adult Treatment Panel) risk definitions. Coronary heart disease or chronic renal impairment were exclusion criteria.
The practices rather than the patients were randomized. This allowed comparison of the two tested strategies across a broader set of variables than adherence alone. Within primary care, conveying information during the limited duration of patient visits is a good example among other challenges in providing effective care. Simplified dosing algorithms are not only relevant to adherence, but also to the barriers of multiple-visit dose titrations inherent to risk management by usual guidelines-based care.
In the simplified dosing algorithm arm, physicians were instructed to favour single-pill combinations. Specifically, patients not controlled on a single agent were initiated on an all-antihypertensive combination pill of an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) plus a diuretic. If uncontrolled, this was followed by the single-pill combination of amlodipine for BP control and atorvastatin for lipid control. Additional steps for control of either hypertension or dyslipidemia were permitted as necessary. Rather than comparing specific agents, the objective was to compare rates of control achieved with a simplified dosing strategy at six months relative to usual guidelines-based care.
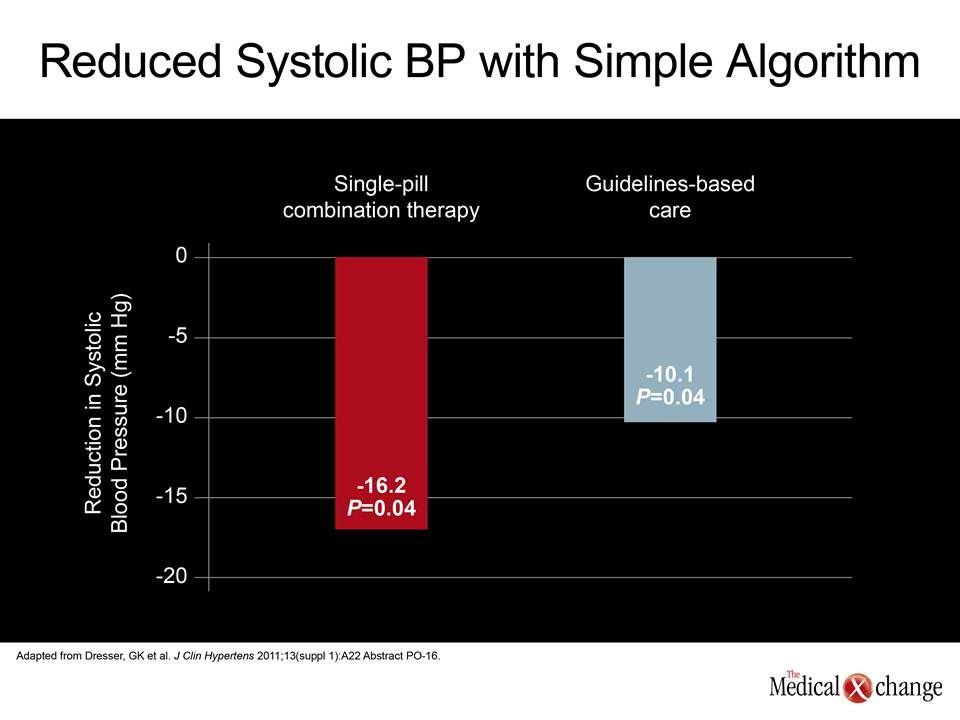
Despite its relative simplification, the single-pill combination strategy provided significantly lower systolic BP at the end of six months when compared to guidelines-based care (-16.2 vs. -10.1 mm Hg; P=0.04) (Fig. 1). Differences in low-density lipoprotein (LDL) were not anticipated nor observed. The proportion of patients within the participating practices who were at goals for guideline-recommended BP and lipid levels was higher in the group receiving the simple drug algorithm, but the difference did not reach statistical significance (31.3% vs. 28.1%; P>0.1).
While the overall results suggest that a simplified algorithm with a single-pill combination of amlodipine and atorvastatin provides better hypertension control in patients who have both hypertension and hyperlipidemia, the more important message is that this approach, which is easier for physicians to administer and makes fewer demands on patients, is at least as good as a more complex treatment scheme with higher pill burdens. These results build on similar findings by the same group of authors in the first STITCH study (Hypertension 2009;53:646-653). In that study, which had a similar design, the authors found that a treatment algorithm beginning with an initial fixed-dose combination of antihypertensive therapy increased the chance of reaching treatment goals by 20% (P=0.028) relative to usual care.
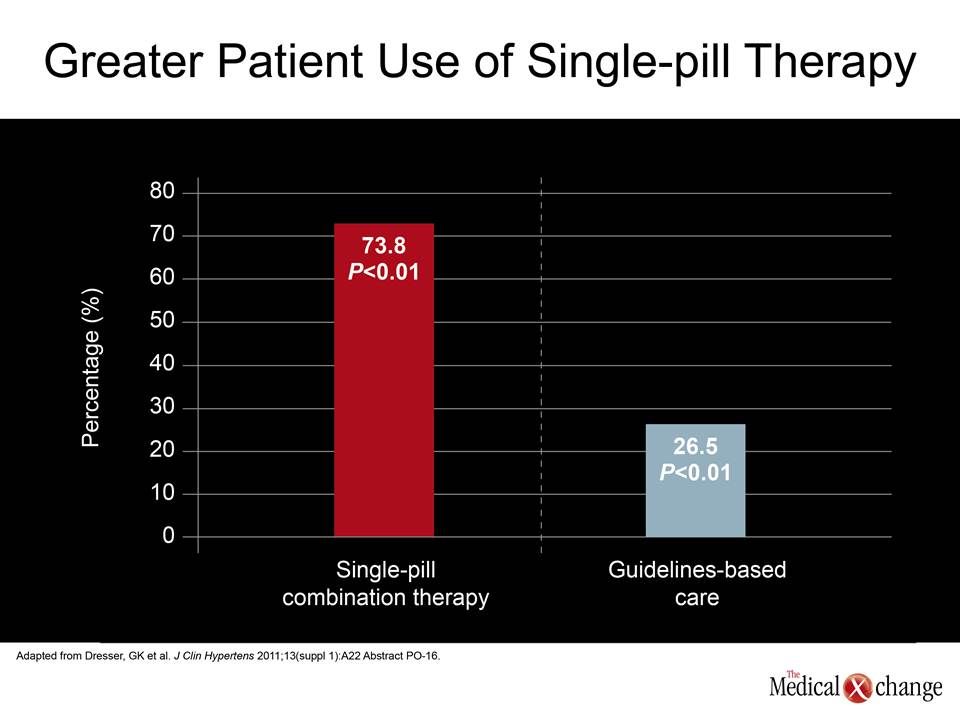
“The STITCH2 algorithm resulted in greater use of any single-pill combination compared to guidelines care.”
“Based on our evidence of improved control rates utilizing a simplified algorithm in the management of hypertension, we proposed to determine if a simplified comprehensive treatment algorithm featuring single pill combinations would improve management of patients with both hypertension and dyslipidemia,” Dr. Dresser explained. He noted that physicians providing usual guidelines-directed care in STITCH2 were permitted to prescribe single pill combinations, but, like the initial STITCH study, a formal approach to simplification increased the proportion of individuals receiving treatment featuring a low pill burden.
“The STITCH2 algorithm resulted in greater use of any single-pill combination compared to guidelines care (73.8% vs. 26.5%; P<0.01),” Dr. Dresser reported (Fig. 2). Patients in the simplified group did not receive a single-pill combination if their hypertension was controlled on a single agent, but a high proportion of patients in the guidelines-directed care group, like the simplified dosing group, were candidates for single pill regimens. One particular advantage of the amlodipine/atorvastatin combination is a side effect profile that approaches that of placebo.
While the absence of the potential for an interaction makes amlodipine and atorvastatin suitable for a single-pill combination, each drug, whether used alone or in combination, is well tolerated, according to Dr. Dresser. All statins pose a risk for muscle complications, but these are rare and none were reported in this study. Amlodipine is also very well tolerated, although it does pose low risks for several nuisance complaints, such as peripheral oedema. Dr. Dresser reported that the single-pill combination in this study did not produce any serious drug-related side effects.
Conclusion
A study designed to compare a simplified risk management strategy in patients with both hypertension and hyperlipidemia has demonstrated greater hypertension control over a six month period relative to a usual-care, guidelines-based approach. The simplified strategy employed an algorithm that emphasized the use of single-pill combinations of distinct therapeutic agents. This included a renin-angiotensin system inhibitor with a diuretic and the CCB amlodipine with the lipid-lowering agent atorvastatin. The association of the single-pill approach with better control over a six-month period has important implications for long-term outcome.