ADHD
AACAP/CACAP Joint Annual Meeting
New Approach Improves Symptoms and Functioning in ADHD
Toronto – A long-acting stimulant is the usual first-line therapy for most patients with attention deficit hyperactivity disorder (ADHD). Still, a substantial minority of individuals – as many as one in three – do not have an adequate response to these agents. In addition, some patients or their parents may prefer or require other therapeutic options. Data presented at this meeting provided insight on the efficacy of new approaches – employing the alpha-2 agonist guanfacine as monotherapy or in addition to a stimulant – in decreasing ADHD symptom scores and improve functioning.
Improvement in Functioning
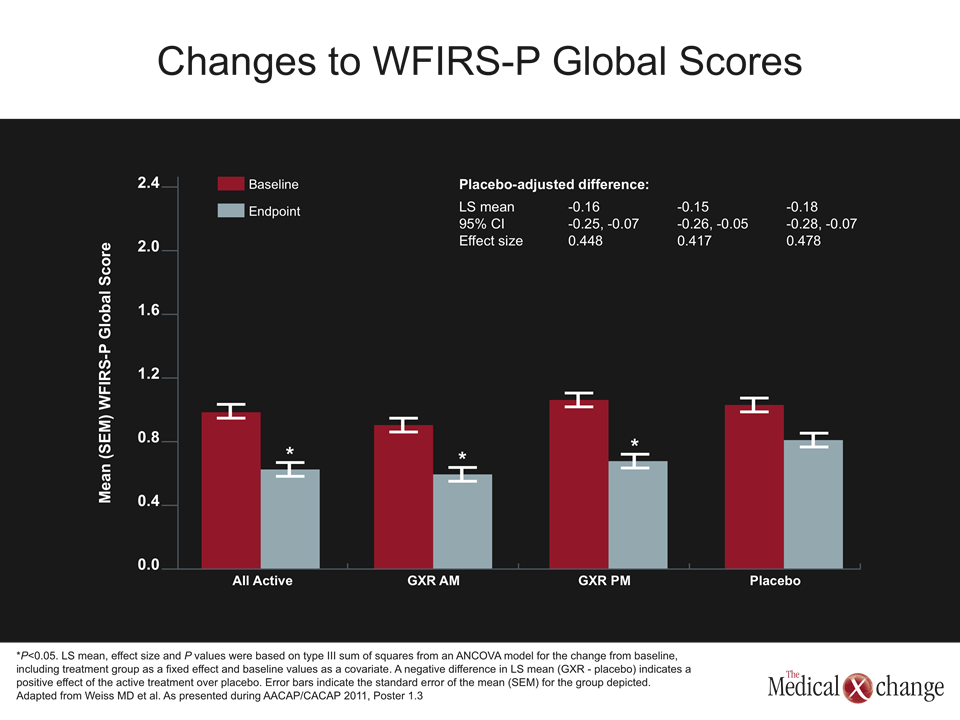
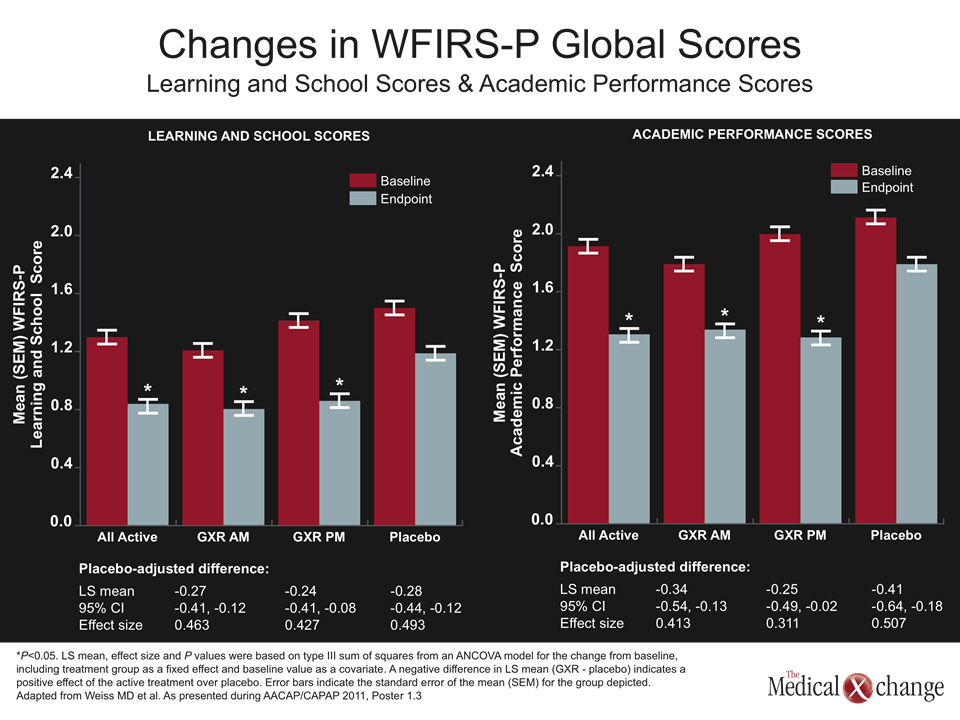
The Weiss Functional Impairment Rating Scale (WFIRS) assesses the impact of attention deficit hyperactivity disorder (ADHD) related behaviour and emotional difficulties on various functional domains. In a study presented at this meeting, Dr. Margaret Weiss, Division of Child & Adolescent Psychiatry, Department of Psychiatry, University of British Columbia, Vancouver, and colleagues examined both the treatment efficacy (changes in ADHD Rating Scale IV scores) and impact on functioning (according to parents’ reports, WFIRS-P), of 8 weeks of treatment with extended-release guanfacine (GXR) vs. placebo.
“In the past, all the clinical trials were on the core symptoms. We never looked at what you really want to know: have you improved the quality of life of the patient? So by looking at functioning as a primary outcome measure we can find out a great deal about whether the drug actually works,” explained Dr. Weiss.
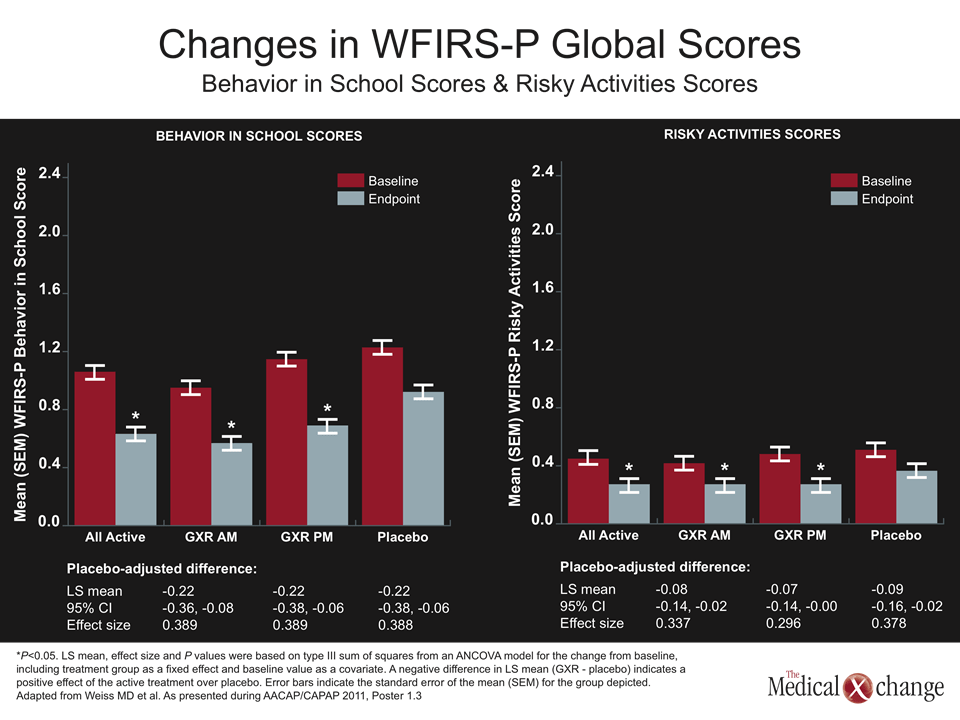
All patients who received an alpha-2 agonist had significantly greater improvement in WFIRS-P global scores.
The study included 333 children (mean age 9 years) with ADHD-RS-IV total score ≥ 28 and a clinical global impressions-severity of illness (CGI) score of ≥4 at baseline. GXR was administered in the morning or evening, titrated to a maximum of 4 mg/day in order to achieve a reduction in ADHD-RS-IV of ≥ 30%; once dose optimization was completed, the patients were maintained on their optimal dose for three weeks, after which dose tapering occurred.
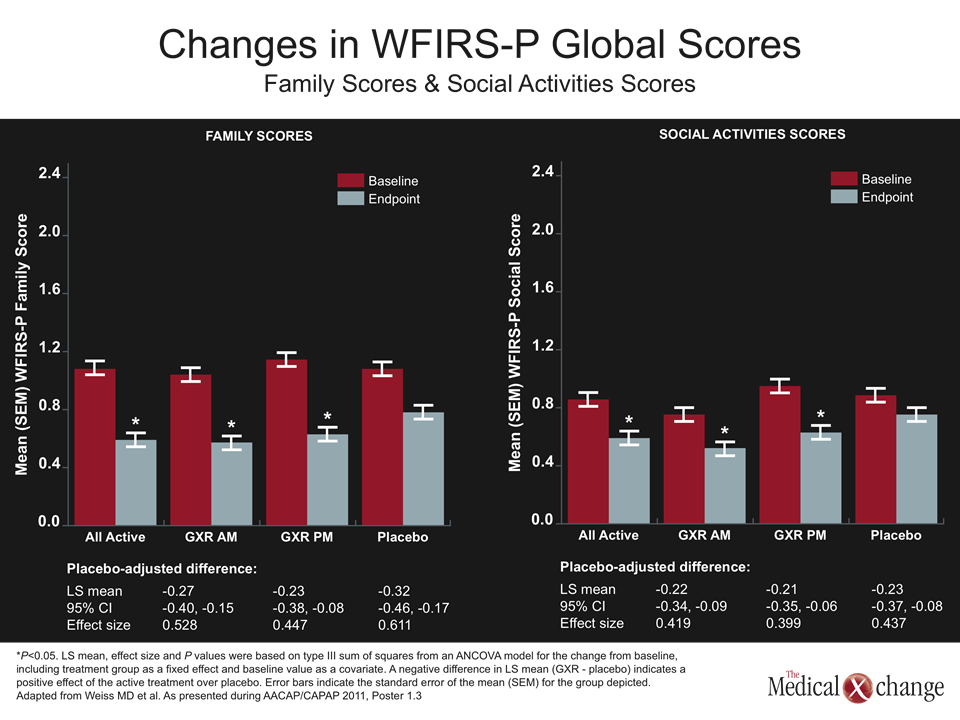
At study endpoint, changes in ADHD-RS-IV scores for patients treated with GXR (morning or evening) were significantly greater than those for patients receiving placebo. Similarly, all patients who received GXR had significantly greater improvement in WFIRS-P global scores (Fig. 1) and in several sub-domains.
The effect sizes, described by the investigators as medium, have a “huge” impact on functioning, Dr. Weiss indicated. “We saw with guanfacine that family scores improved, learning improved – which is really important – academic performance, behaviour, social activities, all improved. Even risky activity scores improved. We were shocked because we didn’t think it would happen [in this younger age group].” Risky activities in this age group include following the lead of a bully and property damage, she clarified.
“One thing that did not improve, but is easy to explain, is self-concept. A lot of children with ADHD have a positive illusory bias…. They [already] feel okay about themselves. It’s the others around them who have trouble,” she added.
Add-on Therapy Beneficial
According to a study headed by Dr. Gregory Mattingly, Associate Clinical Professor, Washington University School of Medicine, St. Louis, Missouri, adding GXR to the regimen of patients receiving a stimulant can ensure a clinically meaningful treatment response and may also be associated with a reduction in stimulant side effects.
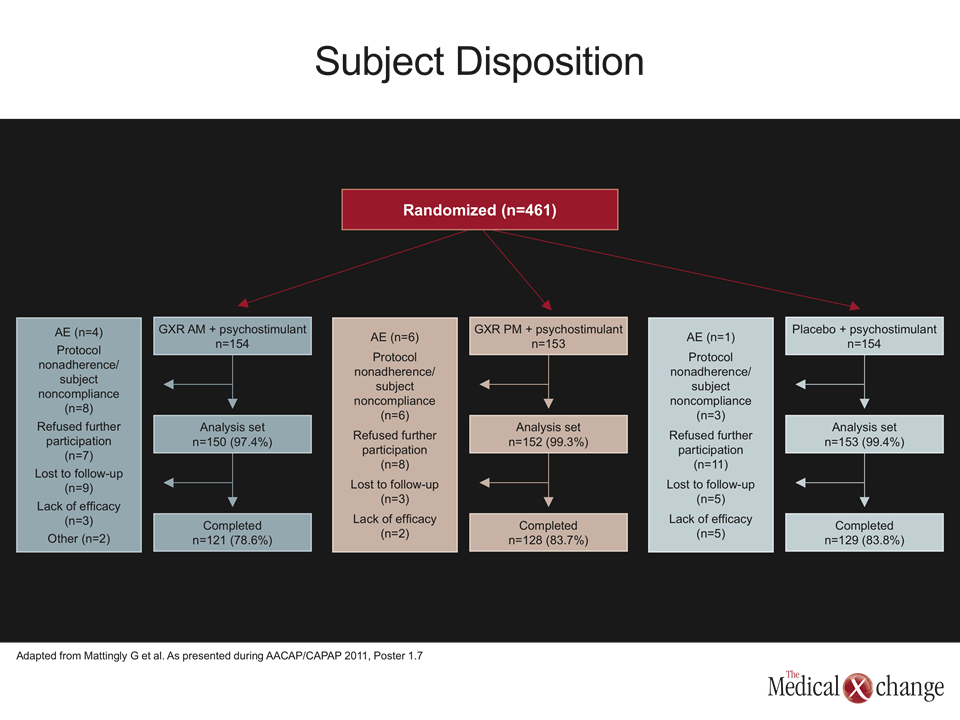
Their study was a post-hoc analysis of an earlier phase 3 trial of GXR used adjunctively with a psychostimulant. It included 455 patients aged 6-17 (mean age 10.8, 72% male) with persistent mild to moderate attention deficit hyperactivity disorder (ADHD) symptoms (ADHD Rating Scale IV [RS-IV] total score ≥ 24 and Clinical Global Impressions-Severity [CGI-S] of ≥3) despite ≥4 weeks of stimulant therapy. The study included two GXR in combination with a stimulant arms (study drug administered morning or evening); in a third arm, patients received a stimulant plus placebo. Dosing was optimized over five weeks to up to GXR 4 mg/day, was maintained at the effective level for three weeks, and then tapered over one week.
Clinically Meaningful Improvement in Symptoms
Adding an alpha-2 agonist as a supplement to a psychostimulant showed improvement in ADHD-RS-IV scores.
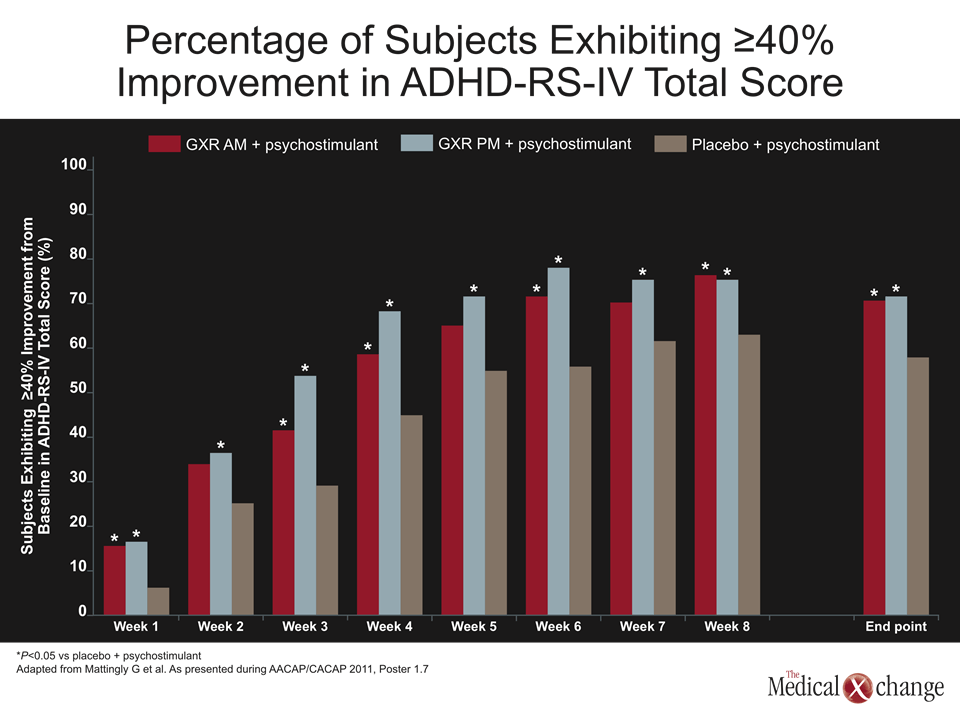
In the original report, subjects who received GXR plus a psychostimulant demonstrated significantly greater improvement in ADHD-RS-IV scores compared with subjects who received a placebo/psychostimulant combination. In the analysis presented here, the aim was to ascertain the percentage of subjects who experienced at least a 40% or 50% reduction from baseline – a decrease associated with clinically meaningful symptomatic improvement.
Over the course of the trial, a significantly greater proportion of patients receiving GXR as a supplement to a stimulant attained these efficacy measures. Figure 2 (Fig. 2) shows the percentages of subjects achieving a ≥40% reduction at each study visit. More than 60% of patients receiving either a morning or evening dose of GXR vs. 46% receiving placebo (P=0.01 and P=0.005) also achieved a ADHD-RS-IV score ≤18, which is used in clinical studies as a cutpoint for symptomatic remission.
Improvement was also observed in patients receiving stimulant monotherapy, a finding reflecting the importance of continued daily administration, Dr. Mattingly indicated. “But what happens in practice? People take it five days a week, then don’t take it on the weekend. They take it for a while, but don’t take it for spring break. This trial showed that consistency with a stimulant works. The [GXR] helped even more.”
“Both [GXR] doses worked; we found the evening doses had a little more side effects,” Dr. Mattingly added. However, he noted, the addition of GXR had a positive effect on stimulant side effects. “Guanfacine slightly lowers the heart rate while stimulants raise it; stimulants can cause insomnia while this causes somnolence. With the combination, there were slightly fewer side effects.” Adverse effects were reported by 76.8% of subjects receiving a GXR/stimulant combination and 63.4% of those receiving placebo. The most common were headache (21.2% in the GXR groups vs. 13.1% in the placebo group) and somnolence (13.6% vs. 4.6%).
Conclusion
The data presented here indicate that in patients for whom current therapies (especially stimulants) are ineffective or undesirable, GXR may be a viable option, Dr. Weiss noted. “This medication has effects for 24 hours given once daily. It makes no difference whether morning or night. That’s an advantage; a lot of kids have trouble taking medication in the morning.” In addition, GXR may be a useful adjunct for patients in whom stimulant therapy is considered inadequate.