hematology
53rd American Society of Hematology (ASH) Annual Meeting and Exposition
Salvage in Multiple Myeloma Patients: New Options Associated with Improved Outcomes
San Diego – In patients with heavily pretreated multiple myeloma, clinically important outcomes are being achieved with new therapeutic agents. A number of phase II and III studies presented at the 2011 American Society of Hematology (ASH) meeting suggest that these novel drugs can revive the activity of previously employed agents, leading to clinically meaningful improvements in such outcomes as progression-free survival. The acceptable tolerability of these newer agents, many of which are administered orally, also suggests progress in extending survival in patients with refractory disease.
New Agents Show Promise
“Patients with refractory multiple myeloma have [historically] had an extremely poor prognosis. In a recent study of patients refractory to bortezomib who relapsed and were not candidates for lenalidomide or another immunomodulatory drug, the median event-free survival was only five months,” reported Dr. Paul G. Richardson, Dana-Farber Cancer Institute, Boston, Massachusetts. Data emanating from recent clinical studies of novel agents, including vorinostat, panobinostat, pomalidomide, and perifosine, suggest that meaningful improvements in outcome can be achieved even in patients with advanced multiple myeloma.
One of the most actively pursued strategies is to resensitize patients to bortezomib by re-introducing this agent in combination with a novel therapy.
According to Dr. Richardson, one of the most actively pursued strategies is to resensitize patients to bortezomib by re-introducing this agent in combination with a novel therapy. In studies employing such combinations, the substantial response rates reported suggest extended disease control. Phase III data were presented here on vorinostat, a histone deacetylase (HDAC) inhibitor. Investigators also presented data from phase II studies of panobinostat (also an HDAC inhibitor), pomalidomide (an immunomodulator), and perifosine (an Akt and P13K inhibitor).
PANORAMA 2: Response to HDAC Inhibitor
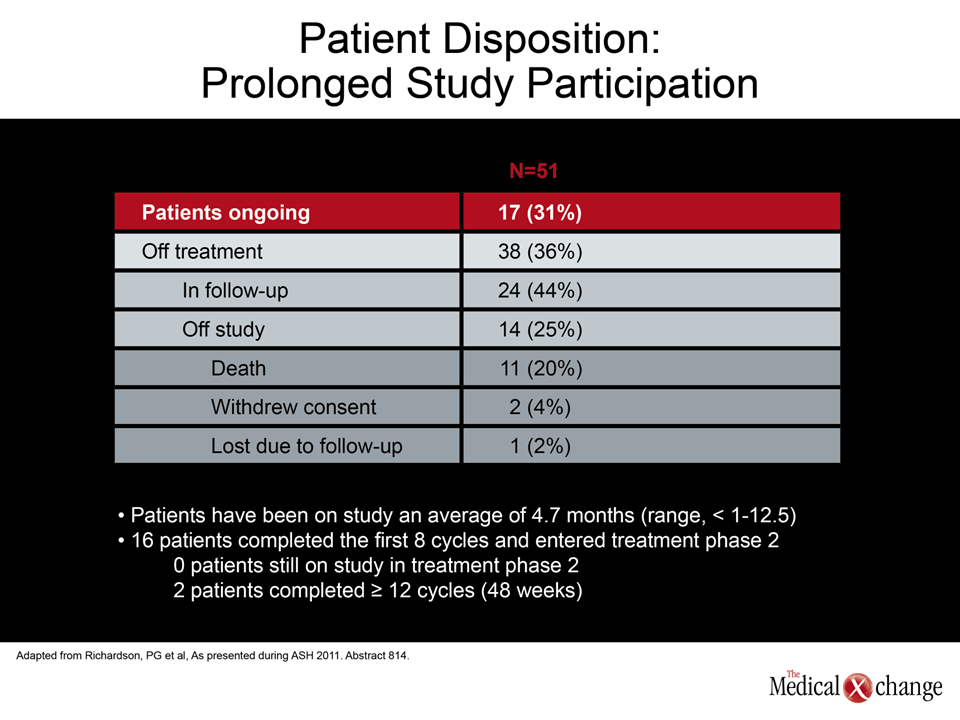
In the PANORAMA 2 study, patients who had progressed within 60 days of initiating their last bortezomib-based therapy were treated with 1.3 mg/m2 bortezomib on days 1, 4, 8 and 11 of a 21-day cycle plus 20 mg of oral panobinostat on days 1, 3, 5, 8, 10 and 12. Patients also received 20 mg of dexamethasone on the day of and day after bortezomib. This phase II analysis was an extension of a phase I study evaluating the same regimen. To enter the phase II study, patients were required to have achieved stable disease or better over 8 cycles in the earlier trial.
“In the phase I study, there were high rates of activity despite the fact that patients had been exposed to a median of 4 prior regimens, with one patient receiving 14 prior regimens. More than half of the patients had received prior stem cell transplant,” Dr. Richardson reported. Of the 53 patients in the phase I study, about 31% have now advanced to the phase II study (Table 1); their response durations correlate with the level of initial response. In two patients with a near complete response (nCR), the duration of treatment has been extended to nearly 9 months.
According to Dr. Richardson, most of the grade 3 and 4 adverse events were hematologic; there was a low incidence of grade 3/4 gastrointestinal adverse events and no grade 3/4 neuropathy. The level of activity, coupled with an acceptable safety profile, allowed investigators to proceed with a phase III trial with this combination (now under way).
VANTAGE 088: Progression-Free Survival
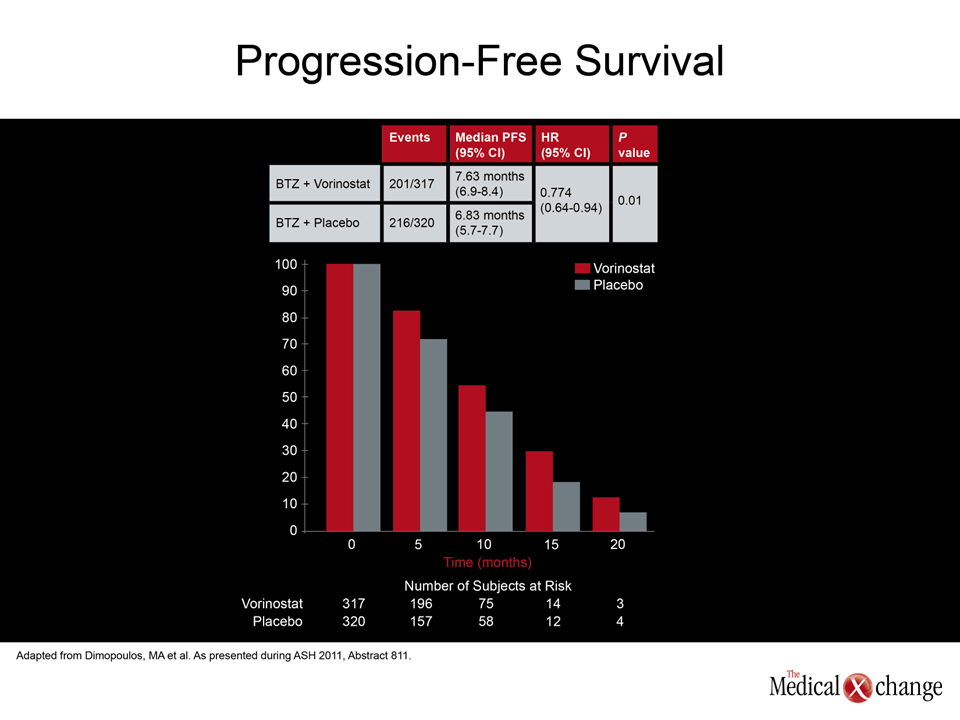
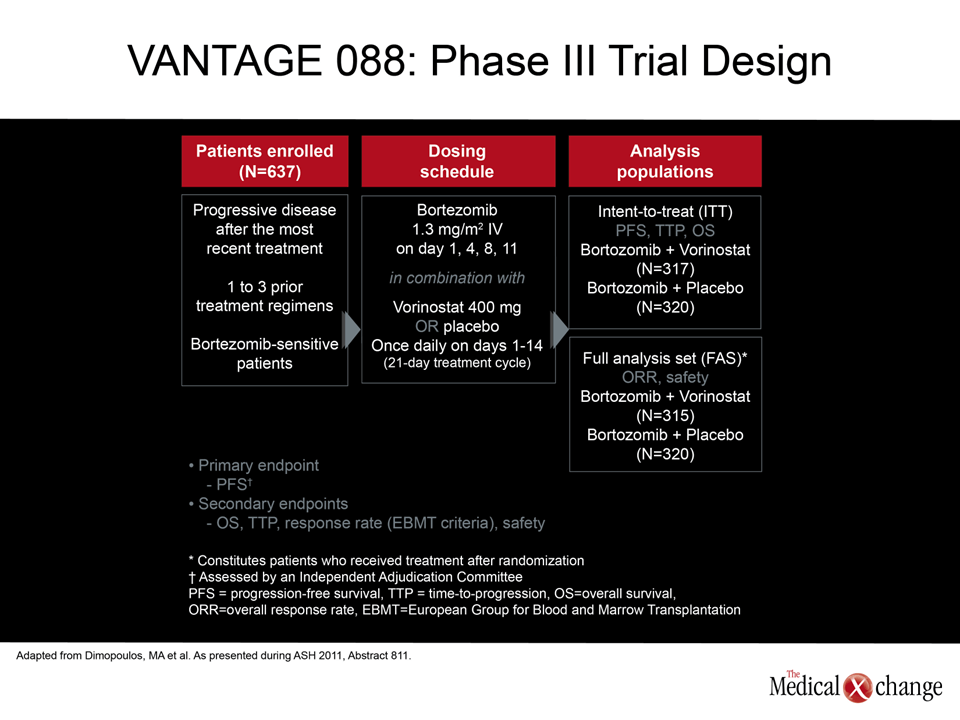
In a multinational study, VANTAGE 088, 637 patients with progressive multiple myeloma who had received up to 3 previous treatment regimens were randomly assigned to receive 400 mg vorinostat or placebo once daily on days 1 to 14 of a 21-day cycle. All patients received bortezomib in the standard dose of 1.3 mg/m2 on days 1, 4, 8, and 11. The primary endpoint was progression-free survival (PFS).
Typical of a population with this disease, the median age was about 61 but approximately 40% of patients were over the age of 65. The mean time elapsed since the start of their initial treatment was 2.9 years. About two thirds of patients had received an immunomodulating drug, such as thalidomide or lenalidomide, and nearly 80% had previously received an alkylating agent. Approximately half had received an anthracycline, about one third had undergone a stem cell transplant, and 25% had previously been exposed to bortezomib.
In this trial, vorinostat plus bortezomib was observed to lead to a 23% improvement in PFS (7.63 vs. 6.83 months; HR 0.77, 95% CI 0.64-0.94; P=0.01) over 25 months of follow-up (Fig. 1).
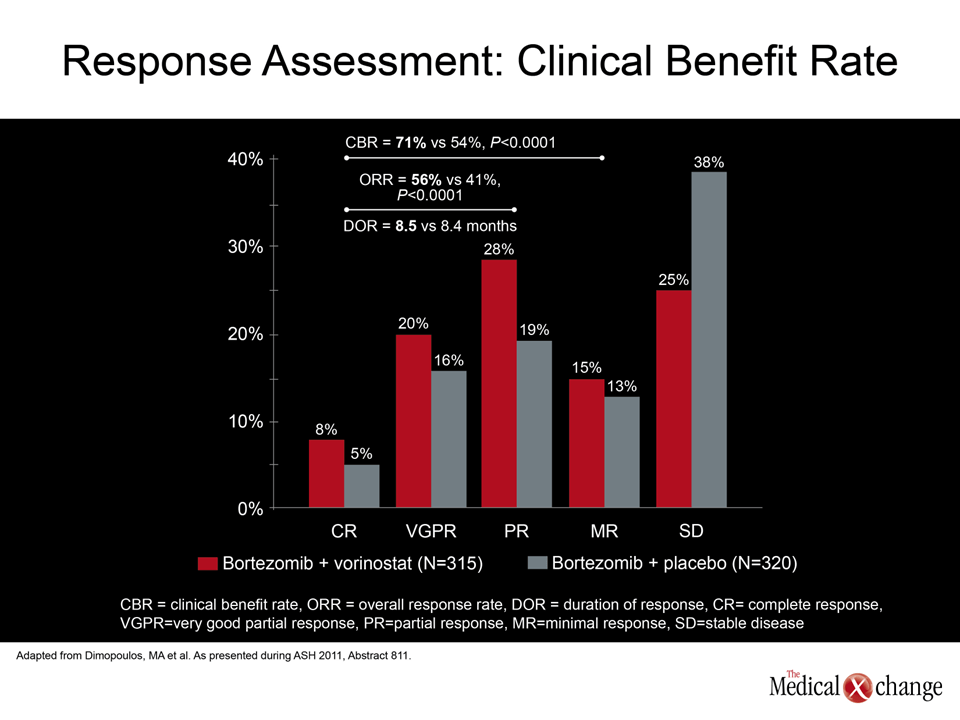
The data for overall survival, a secondary endpoint, are not yet mature but the numbers are promising (HR 0.86, 95% CI 0.62-1.18; P=0.32), according to the senior investigator, Dr. Meletios A. Dimopoulos, Department of Therapeutics, University of Athens, Greece. The activity of vorinostat plus bortezomib relative to bortezomib alone was also substantially greater. The total rate of objective responses was 56% vs. 41% (P<0.0001) while the clinical benefit rate, which included stable disease, was 71% vs. 54% (P<0.0001) (Fig. 2). Time to progression (TTP) had a hazard reduction of 21% (P=0.02) with the combination therapy as compared with bortezomib alone.
“The advantage of vorinostat was statistically significant but it was also clinically significant. In addition to the PFS, there was also a significant improvement in time to progression,” Dr. Dimopoulos stated. “Like the experience with bortezomib, we think that we will see further improvements as we gain experience and refine the regimen.”
Tolerability
The clinical significance of the findings on PFS and TTP was reinforced by the tolerability of the combination regimen, indicated Dr. Dimopoulos. He cited the similar rates of discontinuation due to toxicity observed with the combination and bortezomib alone (21% vs. 22%). The rates of grade 3 and 4 side effects were, in general, raised only slightly with the combination. The exceptions were thrombocytopenia (45% vs. 24%), diarrhea (17% vs. 9%) and fatigue 17% vs. 7%). It was noteworthy that grade 3/4 neuropathy was observed in only 8% of each group, he added.
VANTAGE 095: Encouraging Survival Rates
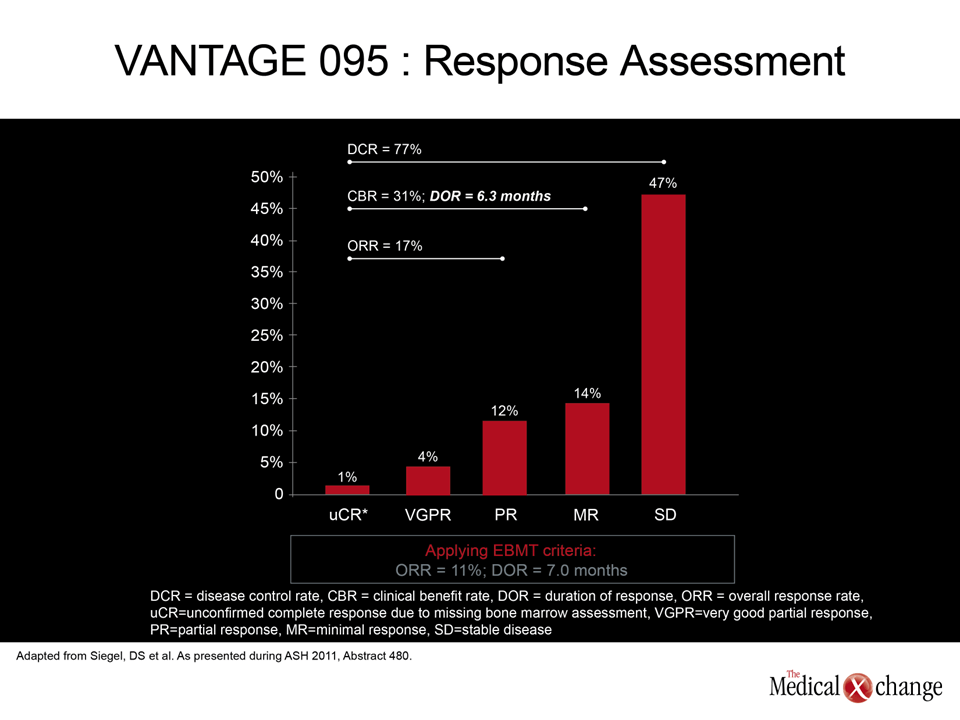
In the VANTAGE 088 study, 60% of patients in both arms were still alive 2 years after initiation of therapy. This finding suggests substantial progress in advanced disease relative to historical rates. Additional encouraging data on patient survival emerged from VANTAGE 095, a multicenter global phase IIB study with a similar treatment protocol but which was restricted to patients refractory to bortezomib. Study patients received bortezomib and vorinostat in the same doses used in VANTAGE 088. Patients with no change or progressive disease after 4 cycles were given 20 mg dexamethasone on the day of and the day after each dose of bortezomib.
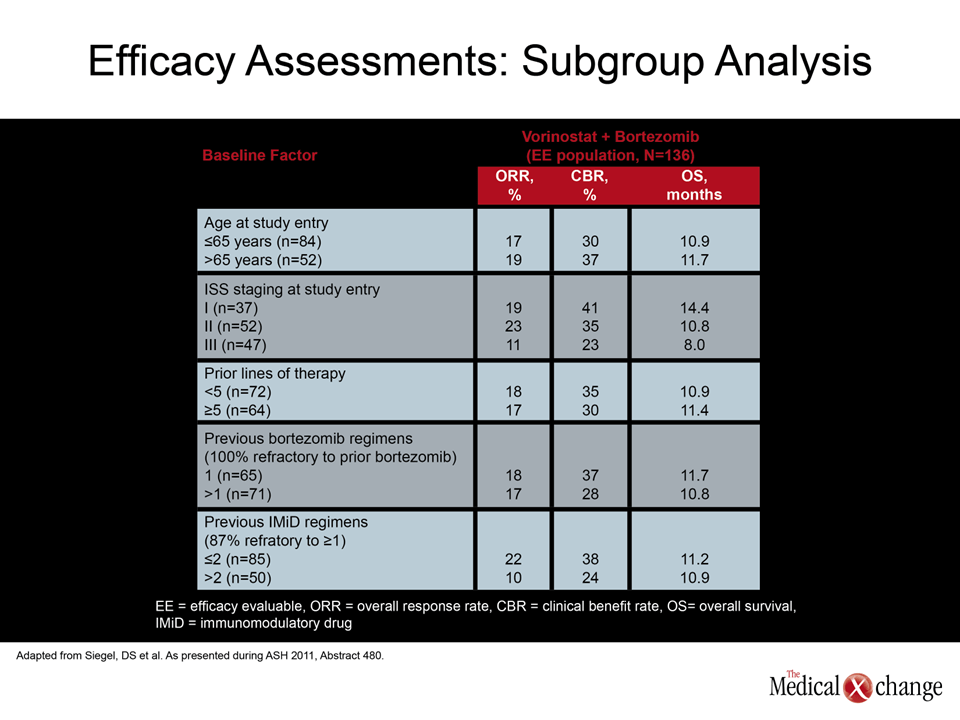
In this study the objective response rate was 17% but the clinical benefit rate climbed to 77% when patients achieving stable disease were included. The median duration of the objective response was 7 months. The 1- and 2-year survival rates, 44% and 32% respectively, are substantially higher than those typically observed in this patient population, according to Dr. David S. Siegel, Hackensack University Medical Center, Hackensack, New Jersey (Fig. 3). The advantage of vorinostat was observed consistently across a broad number of patient stratifications (Table 2).
“The combination was generally well tolerated in heavily pretreated patients, with 27% of the patients receiving 8 or more cycles,” Dr. Siegel reported. He noted that only 19% discontinued therapy due to toxicity. Again, the most common grade 3/4 hematologic side effect was thrombocytopenia (68%). Grade 3/4 anemia was observed in 38% and grade 3/4 neutropenia in 32%. The only non-hematological grade 3/4 side effects observed in more than 10% of patients was diarrhea (17%) and fatigue (13%).
Immunomodulatory Agent Produces Improvements
The potential of novel therapies to extend the lives of heavily pretreated refractory multiple myeloma patients was also documented ina phase II evaluation of pomalidomide. Eighty-four patients were randomized to one of two 28-day treatment cycles. In one, 4 mg of oral pomalidomide was administered daily over 21 days of a 28-day cycle with 40 mg of weekly dexamethasone. In the other, the same doses of oral pomalidomide and dexamethasone were used, but pomalidomide was taken on all 28 days of the cycle. The study was restricted to patients who after previous regimens had no better than a stable disease response or whose disease was refractory to bortezomib and lenalidomide. Of these patients, 69% were refractory to both bortezomib and lenalidomide and progressed on their last line of therapy. The primary endpoint of the trial was the objective response rate.
“The activity was impressive,” reported Dr. Xavier Leleu, Service des Maladies du Sang, Hôpital Claude Huriez, CHRU Lille, France. Specifically, objective responses were achieved in 34.9% of those receiving pomalidomide for 21 days of the cycle and 34.1% in those receiving the drug for 28 days. Most of these were partial responses, but the median PFS was 6.3 months and the median duration of response was 11.4 months in the arm receiving pomalidomide for 21 days of the cycle. The median PFS was 4.2 months for patients with stable disease and 12.6 months for those with an objective response.
Consistent with previous experimental and clinical data, “this study provides further evidence that pomalidomide has no-cross resistance with lenalidomide,” according to Dr. Leleu. He added that further randomized trials of this drug are likely.
Focus on Akt and P13K Inhibitor
Dr. Richardson also presented the results of a phase I/II study of perifosine, an oral agent with action in several signal transduction pathways including JAK2, Akt and NF-kappaB. Perifosine 50 mg daily was administered along with the standard dose of bortezomib plus 20 mg dexamethasone on the day of and the day after bortezomib. All the study participants were heavily pretreated (median number of previous regimens was 5) and were either refractory to or had relapsed after prior exposure to bortezomib.
“For 73 response-evaluable patients, the objective response rate was 41%, including 4% with a complete response,” reported Dr. Richardson. “Of the 53 patients who were refractory to prior bortezomib, the objective response rate was 32%, including a complete response in 2%. In the 20 who relapsed after bortezomib, the objective response was 65%, including two complete responses.” While the median PFS was 6.4 months, Dr. Richardson noted that the longest was more than 3 years.
Characterizing the agent’s toxicity as “manageable,” Dr. Richardson noted that most adverse events were attributed to bortezomib. A phase III randomized trial with this regimen “is currently under way to confirm the efficacy of this approach,” he indicated.
Conclusion
Novel treatment options for multiple myeloma now extend into the relapsed and refractory setting. While front-line treatments have dramatically prolonged survival with an acceptable quality of life, the identification of drugs that can provide activity even in heavily pretreated patients suggests that periods of survival without progression can be further increased. At ASH, several compounds showed promise in the treatment of refractory multiple myeloma.
Additional Slides
Figure 4 (Fig. 4).